Page 10 of 32
PE31.9 | Fever Approach — SDL Guide
Learning Objectives
- Define fever and fever of unknown origin (FUO) with their diagnostic criteria
- Enumerate the common causes of fever in children in the Indian context
- Describe the etiopathogenesis, clinical features, and complications of enteric fever, dengue, and malaria in children
- Identify dengue warning signs and explain when to escalate management
- Select the appropriate investigations and describe the first-line management for each common cause of fever
INSTRUCTIONS
Fever is the most common reason a child is brought to a doctor in India. The differential diagnosis — infections, autoimmune conditions, malignancies — is vast, but in the Indian paediatric context, a small set of organisms accounts for the overwhelming majority of cases: Salmonella typhi (enteric fever), dengue virus, and Plasmodium species (malaria). Knowing how to rapidly identify which organism is responsible, which tests to order in which sequence, and how to manage each condition — including recognising the dengue warning signs that indicate impending shock — can mean the difference between uncomplicated recovery and death. This module provides a systematic framework for approaching any febrile child, with focused depth on the three major treatable infections.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 8 — Fever and Ch. 9 — Infectious Diseases (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 206 — Fever (textbook)
- WHO Dengue Guidelines for Diagnosis, Treatment, Prevention and Control, 2009 (guideline)
- NVBDCP (National Vector-Borne Disease Control Programme) — Drug Policy for Malaria, 2023 (guideline)
- IAP Standard Treatment Guidelines — Enteric Fever, 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 7-year-old girl is brought to the emergency at night with 5 days of high fever. Her parents say she seemed better on days 3 and 4 but is now much worse — she is lethargic, has vomited three times today, and her abdomen hurts. On examination: temperature 39.8°C, pulse 110/min, blood pressure 90/60 mmHg with cold extremities, liver palpable 3 cm below the costal margin. CBC shows WBC 3,200, platelet 54,000, haematocrit 42% (was 36% 24 hours ago). This child has dengue with warning signs — she is on the verge of dengue shock syndrome. Recognising the warning signs and acting within hours changes the outcome from death to recovery.
WHY THIS MATTERS
Fever is the leading presenting complaint in paediatric practice in India, accounting for 30–40% of all paediatric consultations. Yet the consequences of inadequately managed fever span from the trivial — a viral URTI that resolves with symptomatic treatment — to the catastrophic — dengue shock syndrome, cerebral malaria, or enteric fever with intestinal perforation. The skill this module develops is not treating fever as a number to be brought down with paracetamol, but recognising the pattern of fever, identifying the most likely aetiology, selecting targeted investigations, and managing both the symptoms and the underlying cause. The warning signs of dengue are explicitly high-yield for examinations, licensing, and clinical emergencies: every doctor in India must know them by heart.
RECALL
Activate the following prior knowledge before proceeding:
• Body temperature regulation: the hypothalamus is the body's thermostat; temperature is maintained by balancing heat production (metabolism) and heat loss (radiation, convection, sweating); recall from Physiology.
• Normal temperature range: axillary temperature 36.0–37.4°C; oral 36.5–37.5°C; rectal (most accurate) 36.6–38.0°C in children.
• Common paediatric fever causes in India: Salmonella typhi (enteric fever), dengue virus (4 serotypes), Plasmodium spp. (malaria), respiratory infections, urinary tract infections, tuberculosis.
• CBC interpretation: leukocytosis → bacterial infection; leucopenia + thrombocytopenia → dengue or typhoid; eosinophilia → parasitic; lymphocytosis → viral; recall from Pathology.
• Shock recognition: tachycardia, cold extremities, prolonged capillary refill >2 seconds, narrow pulse pressure, hypotension (late sign) — recall from PE emergency blocks.
Clinical Presentation: Approach to a Febrile Child
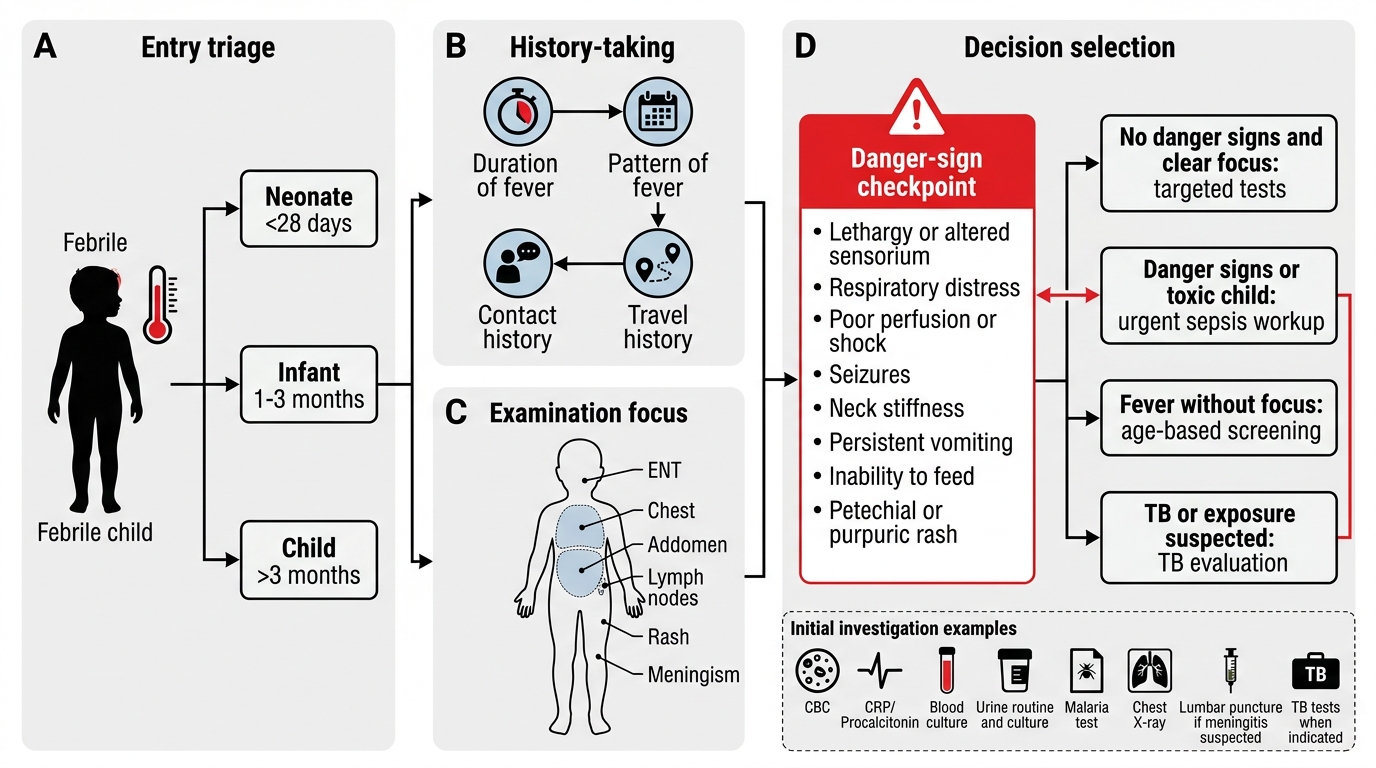
Fever in a child is defined as an axillary temperature consistently above 37.4°C (some references use 37.5°C) or a rectal temperature above 38°C. The first and most crucial decision is not the temperature itself, but whether the child is acutely unwell and whether there are danger signs that require immediate action. The clinical approach to a febrile child must be systematic and reproducible — beginning with a rapid 30-second assessment for IMNCI general danger signs (which, if present, override all other clinical steps and trigger immediate resuscitation and referral), followed by a structured history to identify aetiological clues, a focused examination to locate the site of infection, and targeted investigation precisely guided by the leading clinical hypothesis.
History essentials (aetiological clues):
• Duration and pattern: <7 days = acute fever (infections, most viral and bacterial); 7–14 days = subacute; >14 days = prolonged fever requiring a FUO workup
• Fever pattern: step-ladder rising pattern (enteric fever), brief daily spikes with normal intervals (intermittent malaria), persistent high fever with daily variation but never reaching normal (remittent fever of most infections), saddle-back pattern (dengue — brief defervescence followed by second rise)
• Contact history: household TB contact, school outbreak of viral illness, return from a forest or rural area (malaria risk)
• Travel history: malaria-endemic areas, dengue-endemic urban areas
• Vaccination status: NIS coverage — measles, typhoid, hepatitis A (if received)
• Associated symptoms: rash (dengue, measles, rickettsia), joint pain (dengue, chikungunya), abdominal pain/bleeding (enteric fever, dengue warning sign), headache/photophobia (meningitis), cough/breathlessness (pneumonia)
IMNCI general danger signs (any one → urgent referral/admission):
• Unable to drink or breastfeed
• Vomiting everything
• Convulsions (current or history)
• Lethargic or unconscious
• Stiff neck (meningism)
Fever of Unknown Origin (FUO): Defined as fever >38.3°C documented on ≥3 separate occasions, lasting >14 days, and without a diagnosis after 1 week of thorough inpatient workup. Causes in children include infections (TB, salmonella, Epstein-Barr virus, abscess), connective tissue diseases (JIA, SLE), and malignancies (lymphoma, leukaemia). This is a distinct diagnostic category requiring a systematic, stepwise investigation protocol.
Approach to a Febrile Child
Pathophysiology of Fever
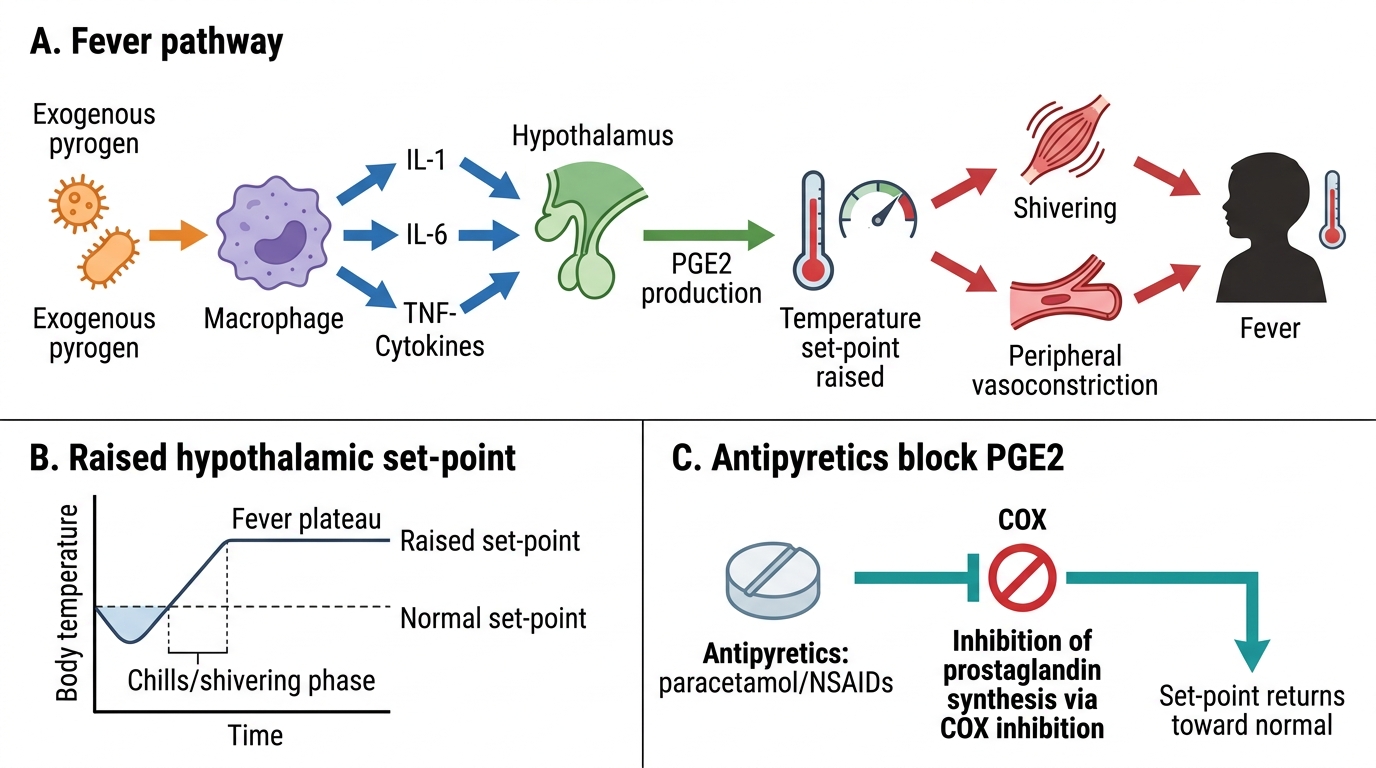
Understanding why fever occurs — and when it is harmful versus when it may be beneficial — is essential for rational management. Fever is not a disease in itself; it is an evolved physiological response to tissue injury or infection, mediated by a precisely regulated cascade of immunological signals. The mechanism proceeds sequentially through two distinct stages: the exogenous trigger from the pathogen, and the endogenous mediator response culminating at the hypothalamic thermoregulatory centre.
Stage 1 — Exogenous pyrogens: Pathogens and their products (bacterial lipopolysaccharide/LPS, viral antigens, toxins) act as exogenous pyrogens. These do not cross the blood-brain barrier directly. Instead, they stimulate monocytes, macrophages, and dendritic cells to produce endogenous pyrogens — the cytokines that actually mediate fever.
Stage 2 — Endogenous cytokine cascade:
• IL-1β, IL-6, TNF-α, IFN-γ — the major endogenous pyrogens — act on the hypothalamic preoptic area (the body's thermostat)
• These cytokines stimulate cyclooxygenase-2 (COX-2) in the hypothalamic endothelium to synthesise prostaglandin E2 (PGE2)
• PGE2 binds EP3 receptors on hypothalamic neurons and raises the thermal set-point — the hypothalamus now 'thinks' the normal body temperature is dangerously low
• The body responds to this elevated set-point by activating heat-generating mechanisms: shivering (skeletal muscle thermogenesis), vasoconstriction (reduces cutaneous heat loss), piloerection, and increased metabolic rate
• Once the set-point is restored (by treatment or pathogen clearance), sweating and vasodilation dissipate the accumulated heat — producing the characteristic 'breaking of fever'
Antipyretic mechanism: Paracetamol (acetaminophen) and NSAIDs (ibuprofen) inhibit COX-2, reducing PGE2 synthesis and thereby lowering the hypothalamic set-point — bringing the temperature down. They do not kill the organism; they only reduce the febrile response. Aspirin is contraindicated in children under 12 years because of the risk of Reye's syndrome (acute encephalopathy + hepatic failure), especially in viral fevers including dengue.
Is fever beneficial? Moderate fever (38–40°C) may enhance immune function (increased phagocytosis, lymphocyte proliferation, IFN production) and impair microbial replication. However, fever above 41°C risks febrile seizures (in susceptible children 6 months to 5 years), metabolic derangements, and hyperthermia-related organ dysfunction. The balance — treat fever that distresses the child or risks seizures; do not suppress every degree of elevation — is the practical clinical principle.
Mechanism of Fever and Antipyretic Action
SELF-CHECK
A 6-year-old boy has 4 days of fever with severe headache. His mother reports that he had a 'temperature break' with sweating on day 3 but the fever returned higher on day 4. His CBC shows WBC 3,800, platelet 68,000, haematocrit 44%. Which dengue warning sign is MOST prominently present in this child?
A. Abdominal pain or tenderness
B. Rapid rise in haematocrit concurrent with rapid fall in platelet count
C. Mucosal bleeding
D. Liver enlargement >2 cm
Reveal Answer
Answer: B. Rapid rise in haematocrit concurrent with rapid fall in platelet count
The WHO 2009 dengue warning signs include rapid haematocrit rise (≥20% from baseline) concurrent with rapid platelet fall. A haematocrit of 44% (from an assumed baseline ~36%) represents haemoconcentration — plasma leakage — while platelets have fallen rapidly to 68,000. This is a critical warning sign indicating plasma leakage (moving toward dengue haemorrhagic fever/dengue shock syndrome) and requires immediate hospitalisation and fluid management. The saddle-back fever pattern (defervescence on day 3 then return of fever on day 4) is also highly characteristic of dengue.
Investigation of Fever: Diagnosis by Pattern and Test
The investigation of fever must be targeted to the most likely diagnosis based on the clinical picture — pattern, duration, age, season, geography, and examination findings. Ordering all available tests for every febrile child is both wasteful and clinically harmful: it drives up costs, delays the diagnosis by generating multiple simultaneous results requiring interpretation, and leads to false-positive findings that trigger unnecessary treatment. The correct clinical reasoning process is pattern recognition first — observing the fever characteristics, the patient demographics, and the epidemiological context — then choosing the one or two tests most likely to confirm or exclude the leading hypothesis. This approach, practised consistently, is the hallmark of a clinician who understands disease rather than one who outsources diagnosis to the laboratory.
Provided image
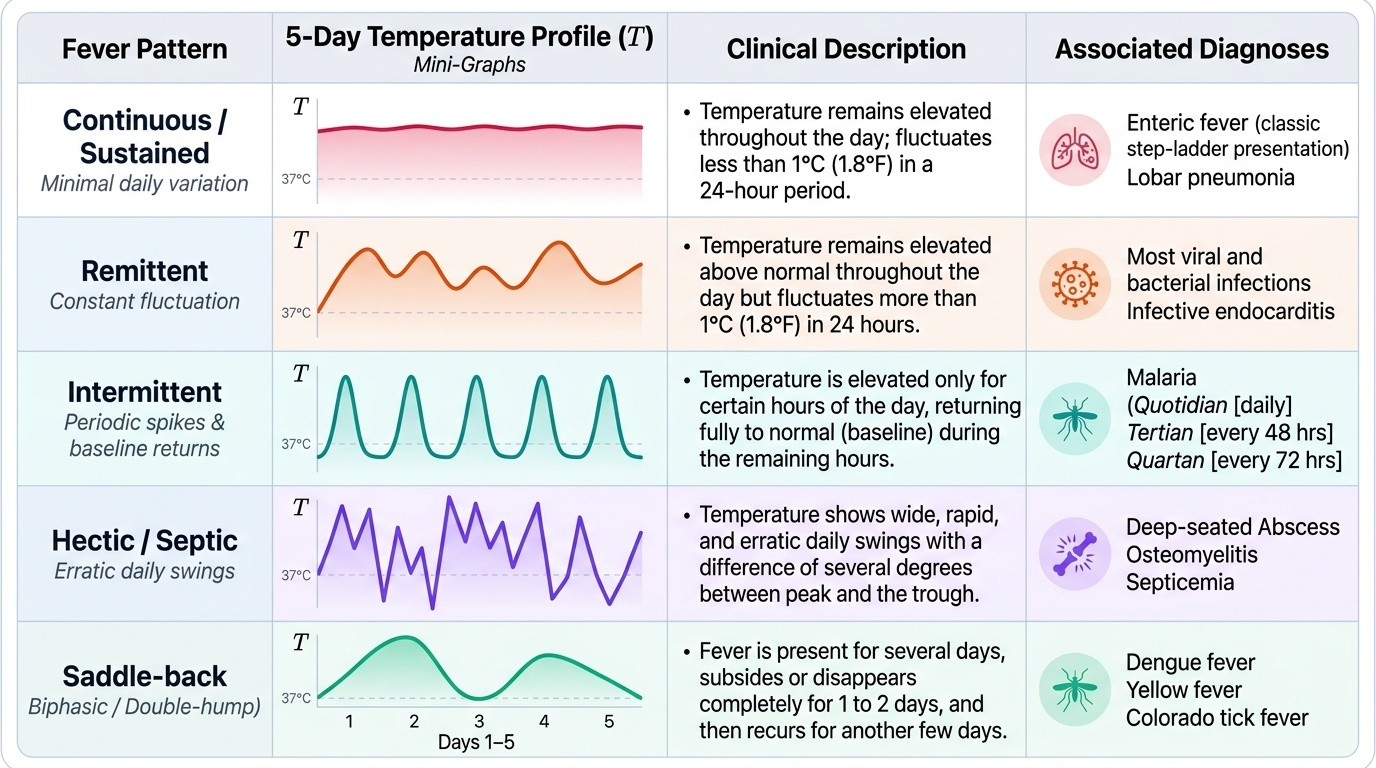
Fever patterns as diagnostic clues:
| Pattern | Description | Common Causes |
|---|---|---|
| Continuous/sustained | Temperature elevated all day, minimal daily variation | Enteric fever (classic step-ladder), lobar pneumonia |
| Remittent | Elevated daily, but never returns to normal, variation >2°C | Most bacterial infections, dengue |
| Intermittent | Returns to normal between spikes | Malaria (quotidian P. falciparum, tertian P. vivax, quartan P. malariae), pyogenic abscess |
| Saddle-back | Initial fever, brief defervescence, then second rise | Dengue (critical phase begins at defervescence) |
| Hectic/Septic | Wide swings with chills and sweating | Bacterial sepsis, osteomyelitis, endocarditis |
Diagnostic tests by suspected cause (PE31.9):
Enteric fever (Salmonella typhi): Blood culture is the gold standard — highest yield in the first 7–10 days; 80–90% sensitive in untreated patients. Widal test (serology): O agglutinin titre ≥1:160 and H agglutinin titre ≥1:160 are conventionally positive, but the Widal has poor specificity due to cross-reactivity (prior typhoid vaccination, non-typhoid salmonellae, other infections); a four-fold rise in paired sera is more meaningful than a single titre. Platelet count is often low (relative neutropenia/leucopenia characteristic). Newer tests: Typhidot IgM (rapid card test) has better specificity.
Dengue: The testing strategy depends on the day of illness:
• Days 1–5 (febrile phase): NS1 antigen (dengue NS1 ELISA or rapid card test) — highly sensitive and specific in first 5 days
• Day 5 onward: IgM antibody (dengue IgM ELISA) — positive from day 5, peaks at 2 weeks
• CBC: thrombocytopenia (<100,000/µL) + haemoconcentration (rising haematocrit ≥20%) is the hallmark of plasma leakage
Malaria: Peripheral blood smear (Giemsa-stained thick and thin film) — the gold standard; identifies species and quantifies parasitaemia; thick smear detects low parasitaemia, thin smear identifies species. Rapid Diagnostic Test (RDT) — detects HRP-2 (P. falciparum antigen) or pLDH (pan-Plasmodium); useful at peripheral health facilities without microscopy. Both peripheral smear and RDT are available free at NVBDCP centres.
FUO workup: After exclusion of common causes — CBC with differential, blood cultures, urinalysis/urine culture, CXR, TST, Mantoux, ESR, CRP; then second-level: ANA, anti-dsDNA (autoimmune), LDH, uric acid (lymphoma/leukaemia), bone marrow biopsy (if haematological malignancy suspected), CT abdomen (abscess, lymphadenopathy).
CLINICAL PEARL
The dengue warning signs — memorise all 7 (WHO 2009): Abdominal pain or tenderness; Persistent vomiting (≥3 episodes in 1 hour); Clinical fluid accumulation (ascites, pleural effusion, pericardial effusion); Mucosal bleeding (gum bleed, epistaxis, petechiae); Lethargy or restlessness; Liver enlargement >2 cm below costal margin; Rapid haematocrit rise concurrent with rapid platelet fall. Any one of these in a dengue patient signals the critical phase — plasma leakage into third space — and mandates hospitalisation and aggressive fluid monitoring. NEVER give aspirin or NSAIDs in dengue — they worsen thrombocytopenia and bleeding risk. Paracetamol is the only safe antipyretic in dengue.
SELF-CHECK
A 5-year-old returns from a forest area with 3 days of fever. Peripheral blood smear shows: large ring forms occupying <1/5 of RBC diameter, multiple infection of a single RBC, presence of banana-shaped gametocytes, and no enlargement of infected RBCs. Which Plasmodium species is MOST likely responsible?
A. Plasmodium vivax — large amoeboid trophozoites, enlarged RBCs, Schüffner's dots
B. Plasmodium falciparum — multiple small ring forms per RBC, banana-shaped gametocytes, no RBC enlargement
C. Plasmodium malariae — quartan fever, band-form trophozoites
D. Plasmodium ovale — enlarged and fimbriated RBCs (James' dots)
Reveal Answer
Answer: B. Plasmodium falciparum — multiple small ring forms per RBC, banana-shaped gametocytes, no RBC enlargement
The smear findings are pathognomonic of Plasmodium falciparum: small ring-form trophozoites (occupying <1/5 of RBC diameter), multiple rings per RBC (double infection), banana/crescent-shaped gametocytes (unique to falciparum), and no enlargement of infected red blood cells. P. vivax shows large amoeboid trophozoites with Schüffner's stippling in enlarged RBCs. P. falciparum is the species responsible for severe malaria (cerebral malaria, severe anaemia) and must be treated urgently with artemisinin-based combination therapy (ACT) per NVBDCP guidelines.