Page 4 of 14
PE14.2 | Organophosphorus Poisoning — SDL Guide
Learning Objectives
- Identify the risk factors and epidemiological context of organophosphorus poisoning in Indian children
- Explain the pathophysiology of cholinesterase inhibition and acetylcholine accumulation causing the cholinergic toxidrome
- Recognise the full spectrum of muscarinic, nicotinic, and CNS clinical features using the SLUDGE/DUMBELS framework
- Interpret relevant investigations including serum cholinesterase levels
- Apply the correct management: decontamination, atropine titration to atropinisation endpoint, pralidoxime within the 24-48 hour window, and airway support
- Explain why pralidoxime (PAM) becomes ineffective after 24-48 hours due to irreversible ageing
INSTRUCTIONS
Organophosphorus (OP) poisoning is a life-threatening emergency with a specific and teachable toxidrome — the cholinergic crisis. Its management requires understanding two distinct antidote mechanisms: atropine (which counters muscarinic effects) and pralidoxime (which reactivates the inhibited enzyme, but only within a critical 24–48 hour window). Missing that window renders pralidoxime useless. This module builds your ability to recognise the toxidrome, administer antidotes correctly, and avoid the common error of undertreating with atropine.
References
- Ghai Essential Pediatrics, 9th Edition — Chapter on Poisoning (textbook)
- Nelson Textbook of Pediatrics, 21st Edition — Poisoning (textbook)
- IAP Guidelines on Management of Organophosphorus Poisoning in Children (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-year-old girl is brought to the emergency department unconscious. Her mother reports finding her in the agricultural storeroom 45 minutes ago with an open bottle of pesticide. On examination she is deeply unconscious, with bilateral pinpoint pupils, profuse salivation and bronchial secretions, a respiratory rate of 36 with audible wheeze and crepitations, and bradycardia of 48/min. Her limbs show visible muscle fasciculations. The paramedic who transported her gave her atropine 0.5 mg IV once — 'a full dose' — but she has not improved. The emergency nurse asks for your orders. What is your immediate plan, and why is the atropine dose given so far critically insufficient?
WHY THIS MATTERS
Organophosphorus poisoning is one of the leading causes of poisoning deaths in India across all age groups, and represents a significant proportion of paediatric poisoning admissions, particularly in agricultural communities. Children are exposed through accidental ingestion of pesticide containers stored in homes and agricultural stores — often in unlabelled bottles or accessible locations. The cholinergic toxidrome it produces is dramatic, rapidly progressive, and potentially fatal from respiratory failure if not recognised and treated immediately. The management is protocol-driven and highly teachable: two antidotes with specific mechanisms and time-sensitive windows, guided by a clear clinical endpoint (atropinisation). As a future physician practising in India — where organophosphate pesticide use is widespread — you must be able to recognise a cholinergic crisis instantly and initiate correct antidote therapy without hesitation.
RECALL
Before studying organophosphorus toxicology, recall these foundational concepts:
- Cholinergic synapse: Acetylcholine (ACh) is released from the presynaptic terminal, binds receptors, and is then rapidly broken down by acetylcholinesterase (AChE) to terminate the signal. This termination is essential — without it, ACh accumulates and continuously stimulates the receptor.
- Muscarinic receptors are located on smooth muscle, cardiac muscle, and glands (PSNS targets). Stimulation produces: bradycardia, bronchoconstriction, increased secretions (salivary, lacrimal, bronchial, gastric), miosis, and increased gut motility. Atropine is the prototype muscarinic antagonist.
- Nicotinic receptors are at the neuromuscular junction (skeletal muscle) and autonomic ganglia. NMJ stimulation causes fasciculations; with sustained depolarisation block, weakness and paralysis follow — critically including the respiratory muscles.
- CNS acetylcholine receptors: Both muscarinic and nicotinic subtypes in the brain mediate cognition, consciousness, and autonomic regulation.
Clinical Presentation: The Cholinergic Toxidrome
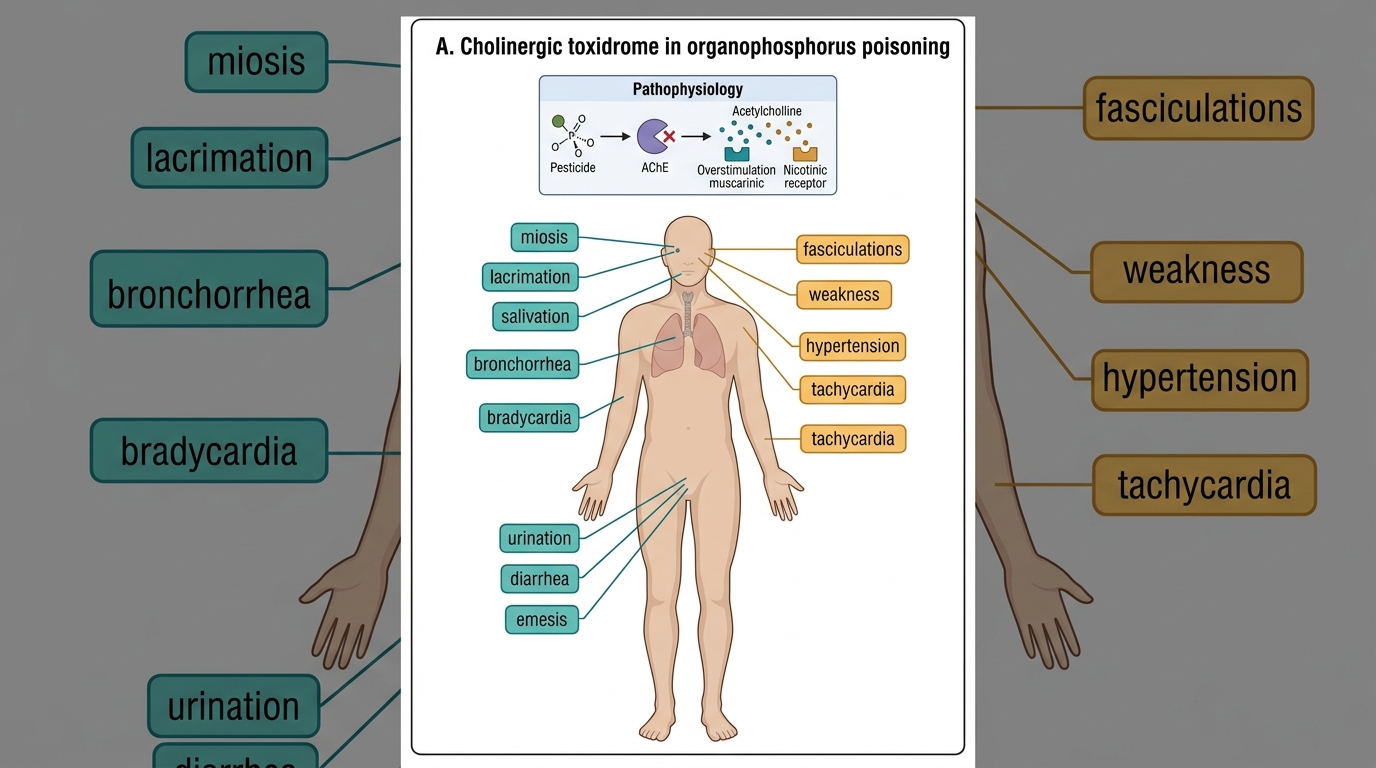
The clinical presentation of organophosphorus poisoning is the cholinergic toxidrome — a constellation of features directly explainable by acetylcholine accumulation at muscarinic and nicotinic synapses throughout the body. Recognising this pattern rapidly is the clinician's most critical skill: the toxidrome is consistent, systematic, and distinguishable from other comatose or convulsing children by its specific combination of features. Unlike many toxic presentations where the diagnosis is retrospective, the cholinergic toxidrome is sufficiently distinctive that an experienced clinician can identify it from the foot of the bed — profuse secretions, pinpoint pupils, visible fasciculations, and bradycardia are a pattern that has no close differential when they occur together. Final-year students should be able to work through the full picture organ by organ using the SLUDGE or DUMBELS mnemonic, mapping each feature to its underlying receptor overstimulation, as this reasoning directly drives the antidote choice.
Muscarinic features (SLUDGE / DUMBELS): The muscarinic features arise from overstimulation of parasympathetic target organs and are the most immediately recognisable:
- Salivation — profuse drooling
- Lacrimation — excessive tearing
- Urination — urinary incontinence
- Defaecation — faecal incontinence
- GI cramps — abdominal pain, vomiting
- Emesis — vomiting
(Or DUMBELS: Defaecation/Diarrhoea, Urination, Miosis, Bronchospasm/Bradycardia/hypersalivation, Emesis, Lacrimation, Salivation.)
Of these, the bronchospasm with bronchial hypersecretion ("kill the patient's lungs with secretions") and bradycardia are immediately life-threatening. Miosis (pinpoint pupils) is highly characteristic and one of the most diagnostically useful bedside findings.
Nicotinic features arise from overstimulation of the neuromuscular junction and autonomic ganglia:
- Muscle fasciculations — visible twitching of muscle groups (particularly limb muscles and abdominal wall), sometimes described as a "bag of worms"
- Muscle weakness progressing to flaccid paralysis — the diaphragm and intercostal muscles may be affected, causing respiratory failure (the most common cause of death)
- Paradoxically, nicotinic stimulation at the adrenal medulla and ganglia can produce tachycardia, sweating, and hypertension early in the course — these nicotinic effects may partially oppose the muscarinic bradycardia
CNS features reflect acetylcholine accumulation in the brain:
- Anxiety, agitation, restlessness
- Seizures
- Coma — in severe poisoning, the child is deeply unconscious
| Feature Class | Key Features | Life-Threatening |
|---|---|---|
| Muscarinic | Miosis, salivation, bronchospasm, bradycardia, secretions, incontinence | Bronchospasm + secretions → respiratory failure; bradycardia → cardiac arrest |
| Nicotinic | Fasciculations, muscle weakness, paralysis | Respiratory muscle paralysis → apnoea |
| CNS | Anxiety, seizures, coma | Coma, seizures |
Cholinergic Effects in Organophosphorus Poisoning
Pathophysiology: Cholinesterase Inhibition and Acetylcholine Accumulation
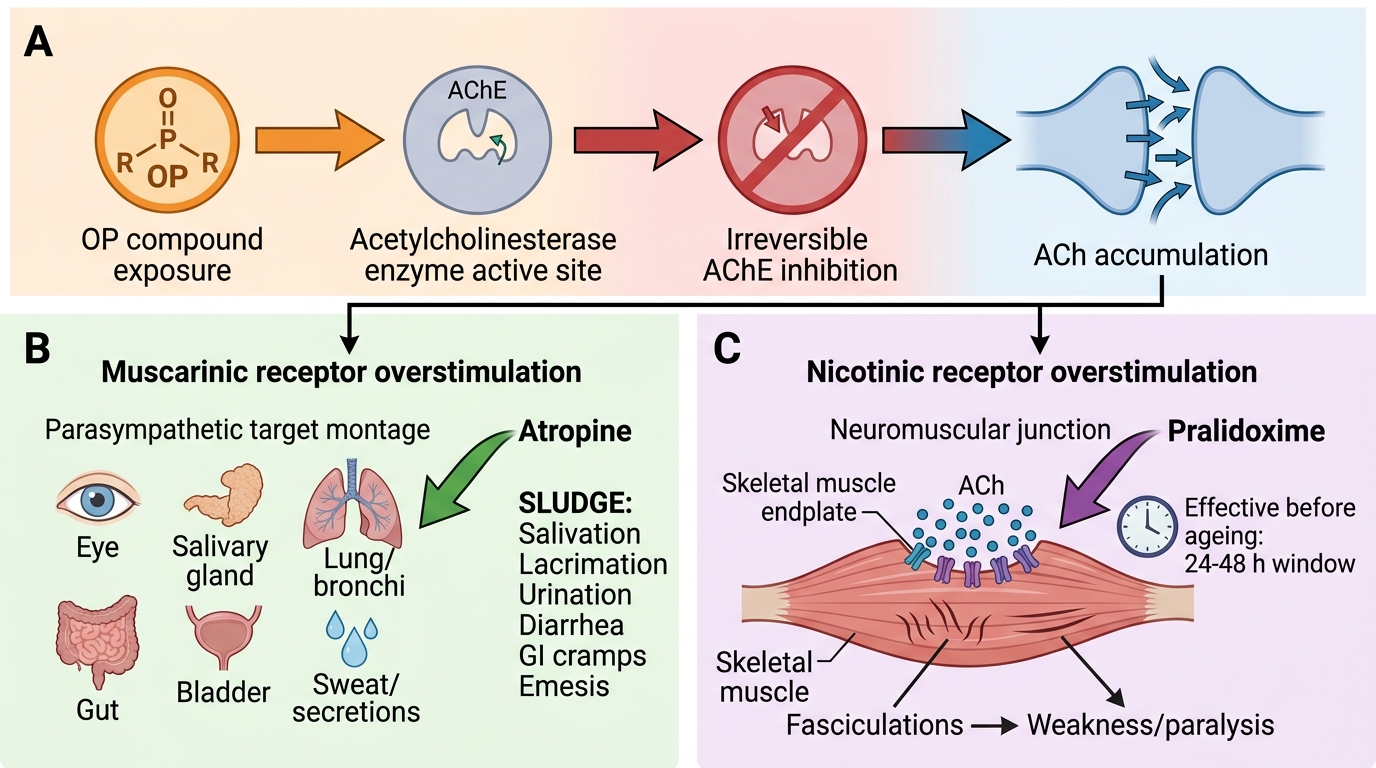
The pathophysiology of organophosphorus poisoning flows directly from a single molecular event — the irreversible inhibition of acetylcholinesterase (AChE) — which then propagates consequences across every cholinergic synapse in the body. Understanding this mechanism precisely is what makes the antidote rationale logical rather than memorised.
Mechanism of AChE inhibition: Organophosphorus compounds (used as agricultural pesticides and chemical warfare nerve agents) contain a phosphate group that binds covalently to the serine residue in the active site of AChE. This binding initially forms a reversible intermediate, but it subsequently undergoes a time-dependent structural change called ageing — in which the phosphate-enzyme bond becomes irreversible and cannot be broken by any reactivating agent. Once ageing is complete (typically within 24–48 hours of exposure, though the exact time varies by compound), the enzyme is permanently inactivated and cannot be rescued pharmacologically. The body must synthesise new AChE — a process that takes days to weeks — before cholinergic transmission normalises.
Consequence — acetylcholine accumulation: With AChE inhibited, ACh released at every cholinergic synapse is not degraded. It accumulates, continues to bind receptors, and produces prolonged, exaggerated stimulation of:
1. Muscarinic receptors (smooth muscle, cardiac muscle, glands) → SLUDGE features
2. Nicotinic receptors at the NMJ → fasciculations → depolarisation block → paralysis
3. Nicotinic receptors at autonomic ganglia → complex mixed sympathetic/parasympathetic effects
4. CNS cholinergic receptors → seizures, coma
Why two antidotes are needed: Atropine blocks muscarinic receptors (countering SLUDGE/bronchospasm/bradycardia) but has no effect on nicotinic receptors and does NOT reactivate AChE. Pralidoxime (PAM), an oxime compound, attacks the phosphate group and breaks the OP-AChE bond, reactivating the enzyme — but ONLY before ageing is complete. This is the critical 24–48 hour window: pralidoxime given after ageing is complete has no effect on cholinesterase activity.
Mechanism of Organophosphorus Poisoning
Risk Factors and Epidemiology in India
Organophosphorus poisoning in children reflects the intersection of agricultural practice, domestic storage patterns, and developmental vulnerability. In India, organophosphate pesticides are among the most widely used agricultural chemicals — they are effective, inexpensive, and available in large quantities at rural households. Understanding the epidemiology and risk factors is not merely academic background; it directly informs the counselling and prevention strategies that every paediatrician must deliver to at-risk families. The result is a unique epidemiological profile that differs markedly from high-income countries where such compounds are tightly regulated and largely inaccessible to household members.
Epidemiological profile: OP poisoning is most common in children aged 1–5 years (accidental ingestion) and in adolescents (intentional self-harm — a different clinical scenario managed similarly but with important differences in consent, documentation, and psychiatric follow-up). Agricultural families are disproportionately affected. States with heavy pesticide use (Punjab, Haryana, Maharashtra, Andhra Pradesh) have higher incidence.
Routes of exposure:
- Ingestion is the most common route in young children — they find and drink from pesticide containers that are improperly stored
- Dermal absorption — organophosphates penetrate skin readily; exposure can occur from contaminated clothing, agricultural water, or direct contact with sprayed crops
- Inhalation — less common in children; relevant during crop spraying or in enclosed spaces
Risk factors:
- Storage of pesticides in unlabelled containers or food/drink bottles, within reach of children
- Lack of secure storage (locked sheds, high shelves) for agricultural chemicals
- Limited parental awareness of pesticide toxicity
- Poor access to poison control information and early medical care
- No childproof closures on commercial pesticide containers in many Indian settings

Routes of Organophosphorus Exposure in Children
SELF-CHECK
A 3-year-old child with organophosphorus poisoning presents with miosis, profuse salivation, wheeze, and bradycardia. After three doses of atropine 0.05 mg/kg IV, her heart rate is 88/min but bronchial secretions persist. What is the correct assessment and next step?
A. She is adequately atropinised — heart rate >80 confirms she has received enough atropine
B. Atropine is contraindicated in the presence of bronchospasm
C. Atropinisation endpoint is drying of secretions, NOT merely heart rate — continue atropine until secretions dry
D. Switch to pralidoxime only, as atropine maximum dose has been reached
Reveal Answer
Answer: C. Atropinisation endpoint is drying of secretions, NOT merely heart rate — continue atropine until secretions dry
The endpoint of atropine therapy in OP poisoning is drying of secretions (and clearing of bronchospasm) — NOT a fixed heart rate target. Heart rate >80/min is a guide to avoid over-atropinisation, but if secretions persist the muscarinic blockade is incomplete. Atropine has NO fixed upper dose limit in OP poisoning — doses of hundreds of milligrams may be required in severe poisoning. Pralidoxime (PAM) is given concurrently but does not replace atropine. Continue atropine (0.02–0.05 mg/kg IV every 5–10 min) until secretions dry.