Page 1 of 9
PE32.1 | Child Health Ethics and Medicolegal Practice — SDL Guide
Learning Objectives
- Identify the unique ethical dimensions of paediatric healthcare, including the evolving autonomy of children and the role of parents as proxy decision-makers
- Describe the four core principles of biomedical ethics as applied to children (beneficence, non-maleficence, autonomy, justice) and the concept of the best interests of the child
- Explain the legal basis for consent and assent in paediatric practice, including parental rights and the circumstances under which parental refusal of treatment can be legally overridden
- Describe the provisions of the POCSO Act 2012 and the JJ Act 2015 relevant to child healthcare, including mandatory reporting obligations under POCSO Section 19
- Identify clinical indicators of child abuse and neglect across all four categories (physical, emotional, sexual, neglect) and describe the physician's medicolegal duties
- Explain confidentiality, its limits in child protection, and socio-cultural barriers to equitable child healthcare in India
- Describe the process of medicolegal documentation and mandatory reporting, and the physician's interface with Child Welfare Committees and the judicial system
INSTRUCTIONS
Children occupy a uniquely vulnerable position in healthcare: they cannot always articulate their own wishes, they depend on adults whose interests may not always align with their own, and they are protected by a framework of Indian law that places specific mandatory obligations on physicians. Understanding the ethics and medicolegal practice of child healthcare is not optional for the paediatrician — it is a professional and legal duty. This module prepares you to navigate consent dilemmas, recognise and report abuse, work within child protection legislation, and document medicolegal encounters accurately. It directly underpins your competence in all clinical paediatric encounters.
References
- Ghai Essential Pediatrics, 9th ed., Meharban Singh — Chapter on Ethics in Paediatrics (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Kliegman et al. — Chapter on Child Abuse and Neglect; Ethics (textbook)
- Protection of Children from Sexual Offences (POCSO) Act 2012, Government of India (legislation)
- Juvenile Justice (Care and Protection of Children) Act 2015, Government of India (legislation)
- IAP Guidelines on Child Abuse Recognition and Reporting (guideline)
- United Nations Convention on the Rights of the Child (UNCRC) 1989, ratified by India 1992 (international)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the on-call paediatrician at a district hospital. A 7-year-old girl is brought in at night with multiple bruises in different stages of healing — some fresh, some days old — on her arms, back, and thighs. Her mother, who accompanied her, says she fell repeatedly while playing. The child is quiet and avoids eye contact. When you gently ask if anyone hurt her, she shakes her head but looks at her mother. The pattern of injuries does not fit the explanation given. You suspect non-accidental injury. You know that if you are wrong, you risk damaging a family's trust. But if you stay silent, this child may return in a worse state — or not return at all. What are your ethical and legal obligations right now?
WHY THIS MATTERS
Paediatric ethics is not merely a philosophical exercise — it has immediate, practical consequences in every clinical encounter. In India, legislation such as the POCSO Act 2012 imposes mandatory reporting duties on all persons, including doctors, who have knowledge or apprehension of sexual offences against a child. Failure to report carries criminal penalties. Similarly, questions of consent arise daily: a parent who refuses a blood transfusion for a critically ill child, an adolescent seeking confidential advice on reproductive health, a family that declines a recommended vaccine on cultural grounds. Paediatricians who are not literate in child rights law, consent doctrine, and abuse recognition will either over-step their authority or fail in their protective duty. For the final-year student entering clinical practice, this knowledge is non-negotiable.
RECALL
Before proceeding, recall the foundational concepts from your earlier studies:
- Biomedical ethics principles from Beauchamp and Childress: beneficence (act in the patient's best interest), non-maleficence (do no harm), autonomy (respect the patient's right to decide), and justice (fair distribution of resources and care). These principles were introduced in your forensic medicine and community medicine modules.
- Consent law basics: in India, the age of majority is 18 years under the Indian Majority Act 1875. Adults give their own informed consent. For those below 18, a parent or legal guardian provides proxy consent.
- Confidentiality as a general medical duty, and its recognised exceptions (e.g. public safety, court orders).
- Mandatory reporting as a legal concept — certain categories of harm must be reported to authorities regardless of the physician's personal preference.
- The general principle that children are rights-holders, not merely objects of parental care — a principle enshrined in the UN Convention on the Rights of the Child (UNCRC), ratified by India in 1992.
Why Ethics Matters in Paediatric Practice — Orientation
Paediatrics is ethically distinctive in a way that few other specialties are. The adult medicine model assumes a competent patient who can receive information, deliberate, and consent or refuse. The paediatric model shatters this assumption from the outset: the patient may be a neonate who cannot speak, a toddler who cannot understand risk, a school-age child who understands some but not all, or an adolescent capable of complex reasoning but still legally a minor. This creates a three-party relationship — the child patient, the parent or guardian, and the physician — with each party holding distinct interests and authority that do not always align.
Parental authority in India is both legally grounded and culturally powerful. Parents are presumed to act in their child's best interests, and the law recognises their right to make medical decisions on the child's behalf. However, this authority is not absolute. When a parental decision endangers the child's life or welfare, the state — through courts, child welfare authorities, and mandatory reporting frameworks — may intervene. The physician sits at the intersection of these forces: a healer bound by clinical duty, a professional bound by legal obligation, and a citizen bound by the rights of the most vulnerable.
The clinical relevance of this complexity is immediate. Every paediatric consultation that involves consent, every clinical finding that raises suspicion of abuse, every cultural practice that affects a child's health, and every adolescent seeking private advice engages the framework you will learn in this module. The paediatrician is not just a clinician; in child health, the physician is also a child rights guardian.
In India, child health ethics also carries a public-health dimension: gender bias in nutrition and healthcare access, harmful traditional practices (e.g. female genital mutilation, child marriage), vaccine hesitancy rooted in misinformation, and under-reporting of abuse are all ethically-laden challenges that a practising paediatrician will encounter at the community level.
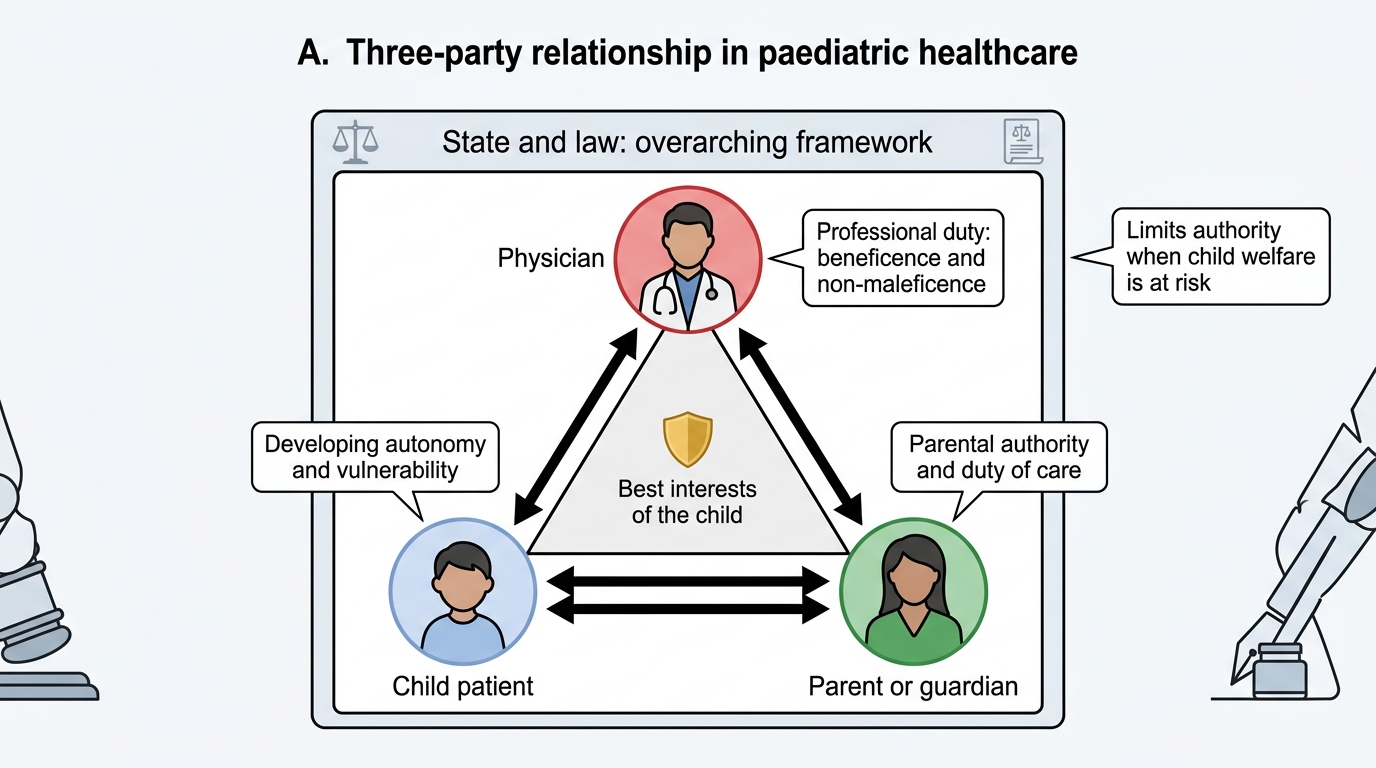
Three-Party Framework in Paediatric Healthcare
Foundations of Child Health Ethics
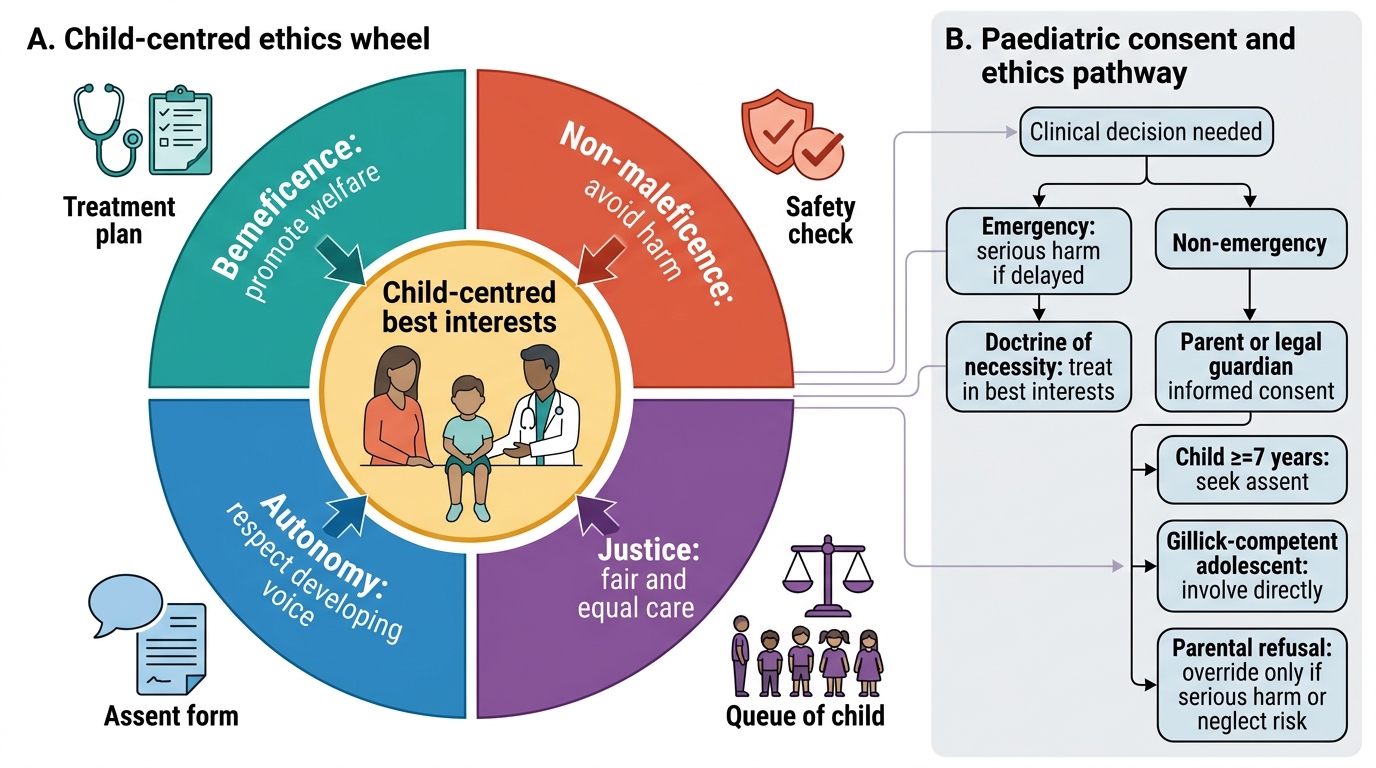
The four principles of biomedical ethics — originally articulated by Beauchamp and Childress for adult medicine — apply to paediatrics with important modifications that reflect the child's developmental status and vulnerability.
Beneficence in paediatrics means acting in the child's best interests, not merely complying with parental preferences. The best interests of the child is the primary legal and ethical standard in all decisions affecting children in Indian law (JJ Act 2015), reflecting UNCRC Article 3. This standard asks: what course of action promotes this child's overall welfare — physical, psychological, and social — most effectively? It is a child-centred standard, not a parent-centred one, though in the vast majority of cases, what parents want IS what is in the child's best interests.
Non-maleficence requires that both the harms of treatment AND the harms of non-treatment be weighed. In paediatrics, withholding a medically necessary intervention because parents refuse it may itself constitute harm — a principle courts have applied when overriding parental refusal of life-saving treatment for children.
Autonomy in paediatrics has two intersecting dimensions. Parental autonomy is the legal right of parents to make medical decisions for their child — a proxy autonomy in the child's interest. Child autonomy is an evolving concept: as children mature cognitively and emotionally, their preferences carry increasing moral (and legal) weight. The concept of Gillick competence, derived from English common law (Gillick v. West Norfolk, 1985) and widely applied in Indian medical ethics, holds that a minor may give or withhold consent for specific health decisions if they demonstrate sufficient understanding and maturity to appreciate the nature and consequences of that decision. In practice, Indian paediatricians apply this principle in adolescent medicine — particularly for reproductive and mental health matters — but formal legal recognition remains incomplete in Indian statute.
Justice in paediatric healthcare addresses equitable access: all children deserve the same standard of care regardless of gender, caste, religion, disability, or socioeconomic status. Justice also informs allocation decisions in resource-constrained settings and is the ethical basis for programmes such as the National Immunization Programme and NRC-based SAM management.
The concept of assent — distinct from consent — is central to child-centred practice. Assent is the child's affirmative agreement to a procedure or treatment. While not legally binding, soliciting assent from children aged approximately 7 years and above is ethically required, as it respects the child's developing autonomy and builds therapeutic trust. A child who is developmentally able to understand and participate in the decision should not have procedures done TO them without engagement.
Biomedical Ethics in Paediatric Care
Consent, Assent, and Parental Rights in Paediatric Care
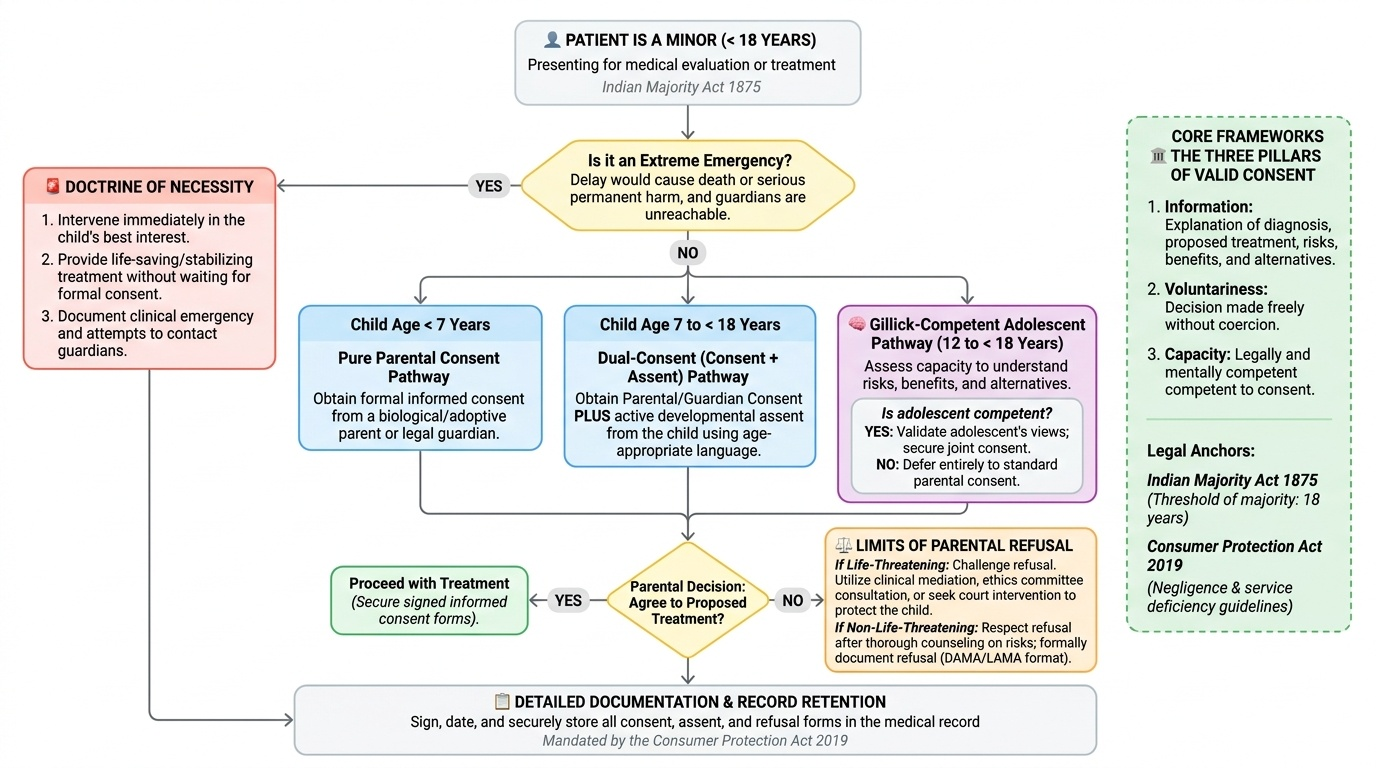
Informed consent in paediatric practice is the bedrock of the physician–family–child relationship. It requires three elements: information (the physician must explain the diagnosis, proposed treatment, risks, benefits, and alternatives in language the parent can understand), voluntariness (the parent must decide freely, without coercion), and capacity (the parent must have legal and mental capacity to consent). In India, the person authorised to give consent for a minor is the parent (biological or adoptive) or, in their absence, the legal guardian. In extreme emergency — when the authorised person cannot be reached and delay would cause serious harm — the doctrine of necessity permits the physician to intervene in the child's best interest without formal consent.
Provided image
The legal framework for consent in Indian paediatric practice rests on several pillars. The Indian Majority Act 1875 sets the age of consent at 18 years. Below this threshold, parental/guardian consent is the rule. The Consumer Protection Act 2019 (which replaced the 1986 Act) has brought medical services within the ambit of consumer protection, meaning that absence of or inadequate consent may give rise to a complaint of medical negligence or deficiency in service. Consent documentation must therefore be detailed, signed, and retained in the medical record.
Parental right to refuse treatment is among the most challenging ethical dilemmas in paediatric practice. Parents have a legal right to decline medical interventions on their child's behalf — but this right is not unlimited. Courts in India have upheld the principle that when parental refusal of treatment poses an immediate risk to the child's life, the physician may seek urgent judicial intervention via the child's constitutional right to life (Article 21 of the Constitution of India). Cases involving refusal of blood transfusion on religious grounds, rejection of chemotherapy for childhood malignancy, or withdrawal from critical care have been litigated in Indian High Courts. The critical threshold is: is this child's life or permanent health at risk? If yes, the physician must escalate — to a senior colleague, a hospital ethics committee if available, and ultimately to legal/judicial authorities — rather than simply deferring to the parent.
| Age Group | Consent Source | Assent Expected | Notes |
|---|---|---|---|
| Neonate/infant (0–2 yr) | Parent/guardian | Not applicable | Proxy consent only |
| Preschool child (2–6 yr) | Parent/guardian | Not expected | May involve explaining in simple terms |
| School-age (7–12 yr) | Parent/guardian | Yes — should be sought | Child's assent is ethically required |
| Early adolescent (13–15 yr) | Parent/guardian | Yes — important | Gillick competence principles begin to apply |
| Late adolescent (16–17 yr) | Parent/guardian (legal default) | Essential | Gillick competence fully applicable; some health decisions may be made independently with clinical judgement |
| 18 yr and above | Patient — self-consent | N/A — full legal capacity |
For adolescent confidentiality, the principle of evolving autonomy applies most strongly. An adolescent seeking advice on sexual health, contraception, or substance use may have a legitimate expectation of privacy that the physician must balance against the parent's role. When there is no risk to the adolescent's life or the welfare of others, the clinician may respect adolescent confidentiality in the interest of maintaining a therapeutic relationship and encouraging health-seeking behaviour.
SELF-CHECK
A 14-year-old girl visits the outpatient clinic alone and requests advice on contraception. Her parents are unaware of the visit. Under which ethical principle do you engage her request confidentially?
A. Beneficence — it is always in the patient's best interest to involve parents in adolescent reproductive care
B. Evolving autonomy — a Gillick-competent adolescent may have a legitimate claim to confidential health advice
C. Non-maleficence — discussing contraception with a minor causes harm by encouraging sexual activity
D. Justice — contraceptive services must be equally available regardless of parental consent
Reveal Answer
Answer: B. Evolving autonomy — a Gillick-competent adolescent may have a legitimate claim to confidential health advice
The concept of evolving autonomy (Gillick competence) holds that a sufficiently mature minor who demonstrates understanding of the nature and consequences of a health decision may receive confidential advice. A 14-year-old seeking contraceptive advice demonstrates health-seeking behaviour that should be supported. Option A conflates 'best interests' with 'parental involvement' — these are not always identical. Option C is a value judgement not grounded in ethics doctrine. Option D is partially true (justice = equitable access) but does not address the confidentiality question specifically.