Page 3 of 9
PE32.1 | Child Health Ethics and Medicolegal Practice — SDL Guide (Part 3)
Documentation, Mandatory Reporting, and Child Welfare Collaboration
Medicolegal documentation in child health cases must meet a higher standard than routine clinical notes, because these records may become evidence in criminal proceedings, child custody hearings, or CWC enquiries. Unlike ordinary clinical documentation — whose primary purpose is communication between treating clinicians — medicolegal records must be comprehensible to, and withstand scrutiny from, police investigators, Child Welfare Committee members, lawyers, and judges who may have no medical training. A poorly written record that is vague, retrospectively amended, or fails to capture the caregiver's exact words can undermine an entire child protection case. The core principles of forensic documentation that guide all medicolegal records apply here with particular force: accuracy (record only what you directly observe and hear, not your inference), objectivity (no emotional language or conclusory labels), timeliness (document at or immediately after the encounter, before memory fades), and completeness (every injury, every history discrepancy, every person present must be noted).
What to document when abuse is suspected:
• Date and time of presentation, and who brought the child.
• Chief complaint in the caregiver's own words — quote verbatim, in quotation marks.
• Developmental history and prior medical history relevant to injury risk.
• Physical examination findings: describe each injury precisely (size in centimetres, colour, shape, location referenced to anatomical landmarks, whether fresh or healing). Body maps/diagrams should be used where available.
• Photographs of visible injuries (with consent or in emergency settings, noting the clinical necessity) — date, time, and photographer identified.
• Laboratory and imaging findings relevant to the alleged mechanism.
• Your clinical impression, stated as 'findings consistent with/inconsistent with the given history' — avoid conclusory language such as 'this child has been abused' unless the diagnosis is certain. State what you observed.
Mandatory reporting under POCSO Act 2012 (Section 19):
Any person — including a physician — who has knowledge or apprehension that a sexual offence against a child has been committed or is being committed MUST report to the Special Juvenile Police Unit (SJPU) or the nearest local police. Reporting can be done in writing, orally (recorded in writing), or by any available means. No fee is required; failure to report is a criminal offence (Section 21 — up to 6 months' imprisonment ± fine). The physician is NOT required to investigate or confirm the offence; reporting a reasonable suspicion is sufficient and protected by law.
Mandatory reporting under JJ Act 2015:
For all categories of child abuse and neglect (not just sexual abuse), the obligation is to report to the police or the Child Welfare Committee (CWC). The CWC is a statutory body with magistrate-equivalent powers for child welfare proceedings. It has authority to order emergency placement, medical examination, and rehabilitation. Physicians may be called to give expert testimony before the CWC.
Working with child welfare agencies: The physician's role is not to investigate or prosecute — it is to (a) provide medical care, (b) document accurately, (c) report, and (d) cooperate with the CWC, police, and courts as expert witnesses. Inter-agency collaboration in child protection (health, police, social services, judiciary) is more effective than any single agency acting alone. Physicians should know their hospital's child protection policy and, where one exists, their designated child protection officer.
Court interface: In medicolegal cases, the physician may be summoned as a witness of fact (to testify about clinical findings) or as an expert witness (to provide opinion on the medical significance of findings). The physician must provide honest, objective testimony that does not exceed clinical competence. Court attendance requires advance preparation of the medical record.
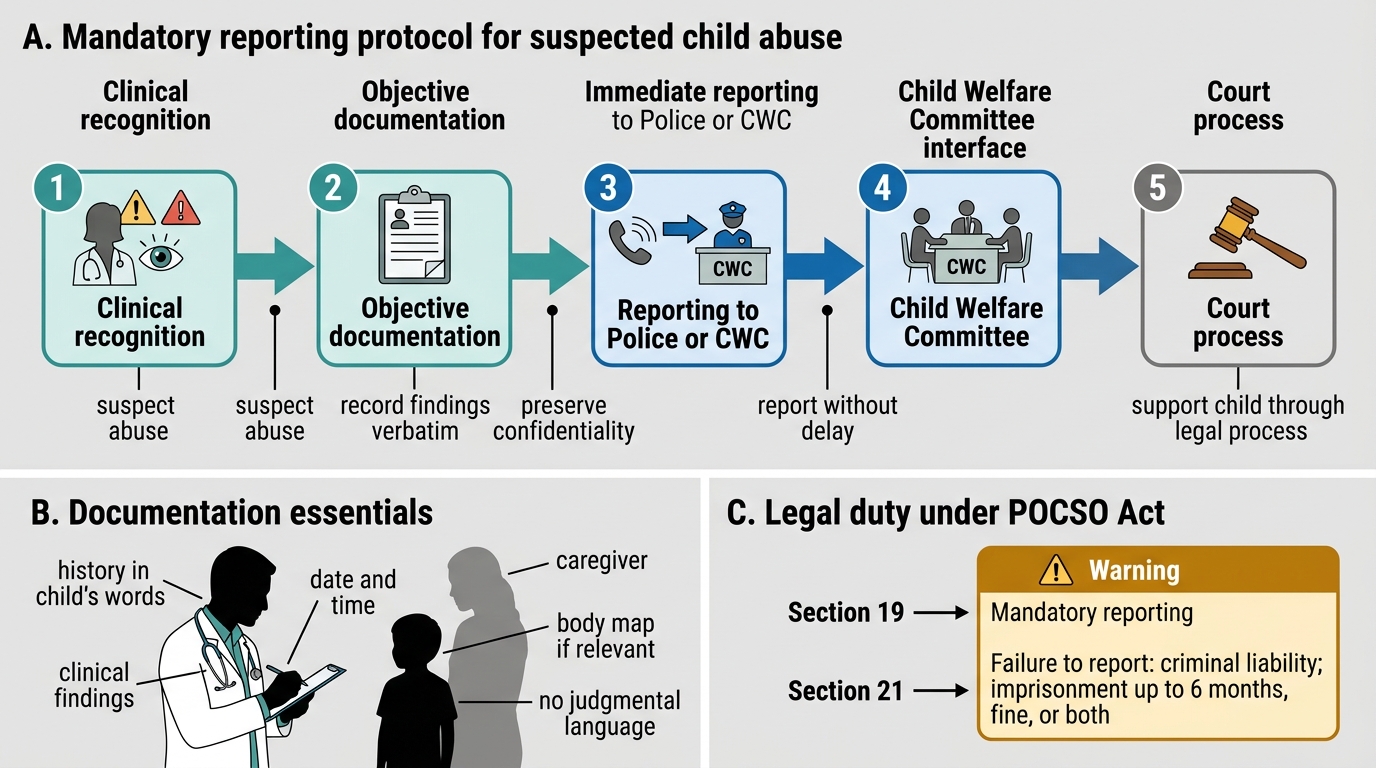
Mandatory Reporting Protocol for Suspected Child Abuse
SELF-CHECK
Under the POCSO Act 2012 (Section 21), a doctor who suspects that a child has been sexually abused but chooses not to report it to the police faces which consequence?
A. No legal consequence — reporting is discretionary for medical professionals
B. Civil liability only — the doctor may face a complaint to the Medical Council
C. Criminal liability — imprisonment up to 6 months, or a fine, or both
D. Administrative penalty — their medical licence may be suspended by the MCI/NMC
Reveal Answer
Answer: C. Criminal liability — imprisonment up to 6 months, or a fine, or both
Section 21 of the POCSO Act 2012 explicitly makes failure to report a criminal offence, punishable with imprisonment of up to 6 months, a fine, or both. Reporting under Section 19 is mandatory for ALL persons (not just doctors, and not discretionary). Options A and B are incorrect — the liability is criminal, not merely civil or administrative. Option D (licence suspension) is a separate possible consequence through professional regulatory bodies but is not what Section 21 specifies. The POCSO framework prioritises criminal accountability to ensure compliance.
Self-Assessment
Use these scenarios to test your understanding of the key concepts from this module. Attempt each question before reading the explanation.
Scenario 1: Consent and parental refusal
A 2-year-old child is admitted with severe pneumonia and hypoxia requiring supplemental oxygen and IV antibiotics. The father refuses hospitalisation and IV treatment on the grounds that 'natural healing' is his family's practice. He insists on taking the child home with oral medicines only. The child is in moderate respiratory distress.
Question: What is the ethically and legally correct course of action?
Response: The child's life is at imminent risk. The physician must first attempt to counsel the father, addressing concerns, explaining risks in terms he understands, and offering to involve other family members or a senior colleague. If refusal persists, the physician must invoke the child's constitutional right to life (Article 21) and escalate to the hospital medical superintendent, a hospital ethics committee if available, and consider emergency judicial intervention. The father's parental authority does not include the right to deny a child life-saving treatment. Document all discussions carefully. The physician must not simply defer to the father in the face of a life-threatening situation.
Scenario 2: Mandatory reporting and confidentiality
A 15-year-old girl presents to a clinic with vaginal discharge. During history-taking (with her mother absent), she discloses that she has been sexually active with a 28-year-old male relative. She begs you not to tell her parents.
Question: What are your obligations under POCSO and confidentiality?
Response: Under POCSO Act 2012, any sexual intercourse with a person below 18 years constitutes a sexual offence regardless of apparent 'consent' — consent of a minor to sexual activity is not recognised in Indian law. Section 19 mandates that you report this to the SJPU/police. You CANNOT maintain confidentiality about an ongoing POCSO offence. You must sensitively explain to the girl that you are legally required to report, that this is for her protection, that she will be supported through the process, and that you will try to ensure she is not harmed by the disclosure. Her request for confidentiality is understandable but cannot override a criminal law obligation. Document the disclosure in her own words.
Scenario 3: Recognising neglect
An 18-month-old is brought to the immunisation clinic. He weighs 7.2 kg (expected ~10–11 kg for age; MUAC is 11.0 cm, <11.5 cm threshold for SAM). His immunisation card shows he has received none of the scheduled vaccines after the birth dose. The mother says 'we forgot'. On examination he is alert but pale, with thin muscles, mild oedema of the feet (bilateral pedal oedema = SAM criterion), and three missed vaccine visits.
Question: Is this child neglect? What are your next steps?
Response: This child meets criteria for severe acute malnutrition (SAM): MUAC <11.5 cm AND bilateral pedal oedema. The combination of SAM, missed immunisations across multiple scheduled visits, and 'forgetting' in a context of progressive undernutrition raises serious concern for medical and nutritional neglect. The steps are: (a) manage the SAM acutely — assess and treat complications, initiate either NRC-based or home-based management as appropriate; (b) take a detailed history to distinguish poverty from neglect (can the family afford food? is there psychosocial dysfunction?); (c) if neglect is substantiated, report to the Child Welfare Committee under JJ Act 2015; (d) engage social support services for the family; (e) document all findings and discussions thoroughly.