Page 1 of 17
PE5.1 | Feeding Problems — SDL Guide
Learning Objectives
- Enumerate the common causes of feeding problems in infants and young children, distinguishing organic from behavioural aetiologies.
- Describe the clinical features and red flag signs that warrant urgent investigation.
- Outline a systematic diagnostic approach including history, growth assessment, and targeted investigations.
- Describe the management of feeding problems including treatment of organic causes, behavioural strategies, and nutritional rehabilitation.
INSTRUCTIONS
Feeding problems are among the most common concerns brought to paediatricians in India, affecting up to 25–45% of children with normal development and up to 80% of those with developmental disabilities. Distinguishing a normal variation of appetite from a significant organic or behavioural disorder has a direct impact on the child's nutritional status, growth, and the family's wellbeing. This module equips you to recognise, evaluate, and manage the full spectrum of childhood feeding problems.
References
- Ghai Essential Pediatrics, 9th ed., Ch 7 (Feeding and Nutrition) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 31 (Feeding Healthy Infants) (textbook)
- IAP Guidelines on Complementary Feeding and Behavioural Feeding Disorders (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 14-month-old boy is brought to your outpatient clinic by his anxious mother, who reports that he 'refuses to eat anything.' She describes mealtimes as battles lasting over an hour, during which he spits out food, throws his plate, and cries. His birth weight was 3.2 kg; today he weighs 8.5 kg. His growth chart shows crossing downward from the 25th to the 5th centile over the last four months. He has no fever, vomiting, or diarrhoea. Is this normal toddler behaviour, a behavioural feeding problem, or is something organic being missed?
WHY THIS MATTERS
Feeding problems represent one of the commonest reasons for paediatric consultations in both primary care and hospital outpatient settings across India. When unrecognised or mismanaged, they lead to nutritional deficiencies, faltering growth, and in severe cases, severe acute malnutrition (SAM). Beyond nutrition, prolonged feeding difficulties create significant parental anxiety and adversely affect the parent–child relationship, which itself affects developmental outcomes. The paediatrician must be equipped to distinguish a transient developmental variation from a clinically significant disorder, to identify the minority of children with an underlying organic cause, and to offer evidence-based management to the majority with behavioural or functional feeding problems.
RECALL
Before proceeding, recall from your physiology and nutrition modules:
• Breastfeeding reflexes (rooting, sucking, swallowing) are present at birth and mature over the first weeks; the extrusion reflex that pushes solids out normally diminishes by 4–6 months.
• Developmental readiness for complementary feeding occurs at around 6 months: the infant can sit with support, shows interest in food, and has adequate oral-motor coordination.
• WHO/IAP growth standards use weight-for-age, weight-for-height, and height-for-age z-scores; normal range is −2 SD to +2 SD.
• SAM is defined as weight-for-height below −3 SD, MUAC <11.5 cm (in children 6–59 months), or bilateral pitting oedema.
• Stomach capacity increases rapidly: from ~10–20 mL at birth to ~200 mL at 1 year; apparent 'small appetite' in a toddler often reflects a developmentally appropriate intake for their body size.
Clinical Presentation of Feeding Problems
Feeding problems encompass a spectrum of difficulties in the acceptance, intake, or tolerance of food that result in parental concern, inadequate nutritional intake, or impaired growth. The clinical presentation varies widely depending on the child's age and the underlying aetiology, and the paediatrician must take a structured history to characterise the problem precisely.
In neonates and young infants (0–4 months), feeding difficulties most commonly manifest as ineffective sucking, prolonged feed times (>30 minutes per breastfeed), excessive crying or arching during feeds, frequent regurgitation, or poor weight gain. Gastro-oesophageal reflux (GOR) — the effortless return of gastric contents — is a normal physiological phenomenon in this age group and does not by itself constitute a disorder; gastro-oesophageal reflux disease (GORD) is diagnosed when reflux causes complications such as oesophagitis, failure to thrive, or respiratory symptoms. Pyloric stenosis presents classically at 3–6 weeks of age with projectile non-bilious vomiting immediately after feeding; the infant is hungry and feeds eagerly between episodes. An olive-shaped mass may be palpable in the right epigastrium, and a test feed may reveal visible left-to-right gastric peristalsis.
In older infants and toddlers (6 months to 3 years), behavioural manifestations predominate: food refusal (refusing to open the mouth or turning the head away), selective eating (accepting only a very limited range of foods), prolonged mealtimes, and gagging or vomiting in response to new textures. Infantile anorexia is a recognised clinical entity characterised by persistent refusal to eat adequate amounts beginning in the first three years of life, in the absence of an organic cause; it is associated with temperament and parent–child interaction patterns. Picky or selective eating is extremely common and, provided growth is maintained, is usually self-limiting.
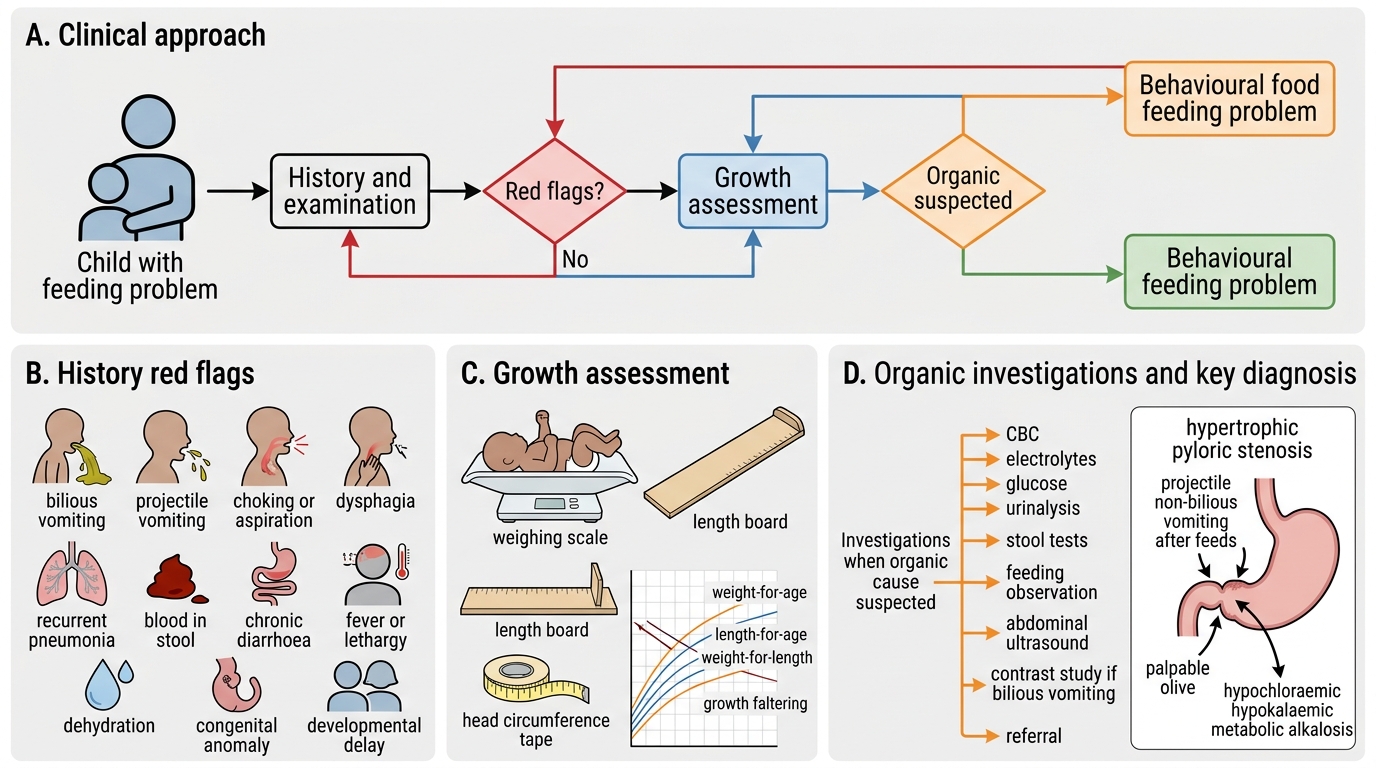
Red flag features that should prompt urgent evaluation include:
• Faltering growth — weight crossing two major centile lines downward, or weight-for-height below −2 SD.
• Dysphagia — difficulty or pain on swallowing, suggesting a structural or neuromuscular problem.
• Recurrent aspiration or unexplained respiratory symptoms.
• Vomiting with bile — always a surgical emergency until proven otherwise.
• Projectile vomiting in a young infant — consider pyloric stenosis.
• Blood in stool or recurrent diarrhoea — consider cow's milk protein allergy (CMPA) or other gastrointestinal pathology.
• Developmental regression or neurological signs.
• Pain behaviours during feeds — arching, stiffening, crying — which may indicate oesophagitis from GORD.
IMEGE_NEEDED markers are essential here; the table below summarises red flag features.
| Red Flag Feature | Possible Aetiology | Action |
|---|---|---|
| Projectile non-bilious vomiting, 3–6 weeks | Pyloric stenosis | Urgent surgical referral |
| Bilious vomiting at any age | Intestinal obstruction/malrotation | Emergency referral |
| Dysphagia/drooling with neurological signs | Cerebral palsy, bulbar palsy | Neurological evaluation |
| Recurrent chest infections + feeding difficulty | Aspiration, tracheo-oesophageal fistula | Imaging; ENT/pulmonology referral |
| Blood/mucus in stool + food refusal | CMPA, enterocolitis | Dietary elimination; allergy work-up |
| Growth faltering (>2 centile lines) | Organic or severe behavioural cause | Full nutritional and medical evaluation |
Pathophysiology and Classification of Feeding Problems
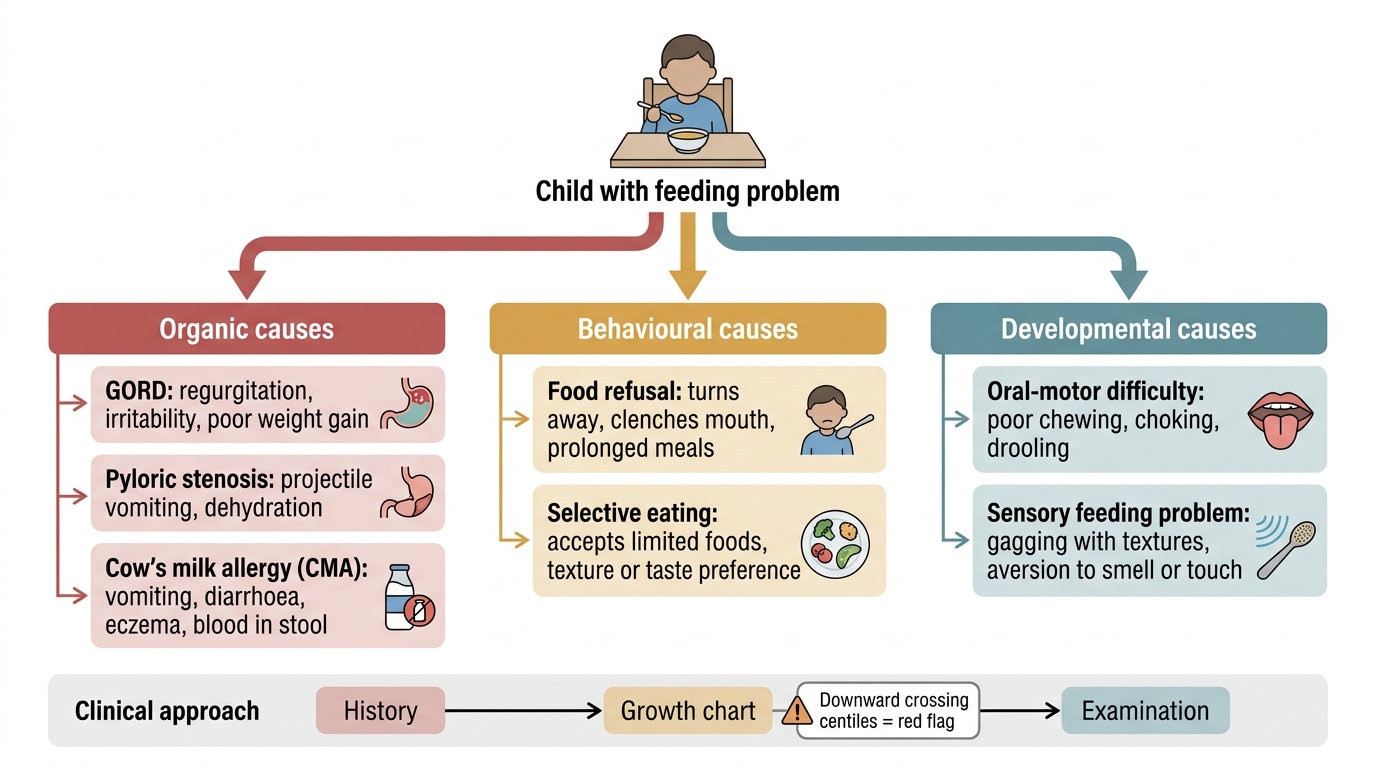
Feeding is a complex, coordinated process involving sensory processing (vision, smell, taste, texture, temperature), oral-motor function (sucking, chewing, swallowing), gastrointestinal motility, appetite regulation (ghrelin, leptin, cholecystokinin), and the psychosocial context of mealtimes. Disruption at any level can produce a clinically significant feeding problem. Understanding the physiological underpinnings helps the clinician identify which level has been disrupted and select targeted treatment. The immature gastrointestinal tract of infants, the developing oral-motor skills of toddlers, and the psychosocial dynamics of mealtimes all contribute to the high prevalence of feeding difficulties across different age groups. A practical three-category classification — organic, behavioural/functional, and developmental — helps structure the clinical approach and avoids the twin errors of missing a treatable organic cause in a child labelled 'just picky' or over-medicalising a normal developmental variation.
1. Organic feeding problems have a definable physiological or structural basis:
- GORD: Transient lower oesophageal sphincter relaxation allows gastric acid to contact the oesophageal mucosa; the infant experiences pain (oesophagitis) and may associate feeding with discomfort, leading to subsequent refusal. Sandifer syndrome — a paroxysmal dystonic posturing of the neck and trunk — is a specific GORD-associated presentation that may be mistaken for seizures.
- Pyloric stenosis: Hypertrophy and hyperplasia of the pyloric muscle (exact aetiology unclear; multifactorial — associated with macrolide antibiotic exposure in neonates and breastfeeding) cause progressive gastric outlet obstruction; the resultant vomiting is forceful and post-prandial, and metabolic alkalosis (hypochloraemia, hypokalaemia) develops over days to weeks.
- Cow's milk protein allergy (CMPA): The most common food allergy in infancy, affecting ~2–3% of infants; both IgE-mediated (immediate urticaria, vomiting, wheeze) and non-IgE-mediated (delayed: FPIES with profuse vomiting 1–4 hours post-ingestion; proctocolitis with blood in stool; enteropathy with malabsorption) forms exist.
- Structural anomalies: Cleft palate, choanal atresia, tracheo-oesophageal fistula, and craniofacial abnormalities impair the mechanics of sucking or swallowing.
- Neurological/neuromuscular: Cerebral palsy, hypoxic-ischaemic encephalopathy, and neuromuscular diseases impair oral-motor coordination, causing inefficient feeding and aspiration risk.
2. Behavioural/functional feeding problems arise from learned aversive associations, parent–child interaction difficulties, or developmental temperament:
- Food refusal and infantile anorexia: The infant or toddler lacks interest in food, shows distraction during meals, or refuses eating without apparent hunger. This is the commonest category seen in well-nourished children.
- Selective/picky eating: Acceptance of only a narrow range of textures, colours, or food types; common in toddlerhood and associated with neophobia (fear of new foods); usually does not compromise growth unless extreme.
- Post-traumatic feeding disorder: Food refusal or aversion triggered by a frightening or painful oral event (choking episode, prolonged nasogastric tube use, painful intubation).
3. Developmental feeding problems overlap with behavioural causes but have a neurodevelopmental basis:
- Sensory processing difficulties: Hypersensitivity to texture, temperature, or smell causes gagging or refusal even to normally palatable foods.
- Oral-motor dysfunction: Immature or disordered chewing/swallowing patterns in children with autism spectrum disorder or developmental delay.
Classification of Feeding Problems in Children
Diagnosis and Investigation
The diagnostic approach to a child with a feeding problem centres on a careful history, physical examination, and growth assessment, with investigations reserved for suspected organic causes. The vast majority of feeding problems are behavioural and do not require laboratory testing. The history is the most powerful diagnostic tool available; a well-structured history will identify red flag features, characterise the feeding behaviour, reveal precipitating events, and expose the mealtime dynamics that sustain the problem. Physical examination confirms growth status and identifies any organic signs. The growth chart is the single most important objective measure — a child who is growing well along their centile despite parental concern about eating is almost certainly not experiencing a clinically significant feeding problem, while a child whose weight is crossing centile lines downward requires prompt evaluation regardless of the parental narrative.
History taking should cover:
- Nature and onset: When did the problem start? Was there a precipitant (illness, hospitalisation, introduction of solids)? Is the problem with liquids, solids, or both? Are specific textures or tastes refused?
- Feeding behaviour: Duration of meals, parental response to refusal (coaxing, force-feeding, distraction), where feeding takes place, mealtime environment.
- Associated symptoms: Vomiting (nature — effortless or projectile; timing — during or after feeds; bilious or not), diarrhoea, blood in stool, skin rash, wheeze, recurrent chest infections, excessive crying, back-arching.
- Developmental history: Attainment of oral-motor milestones; any regression.
- Family and psychosocial history: Parental anxiety about feeding; family food-related behaviours; socioeconomic factors; access to adequate food.
Growth assessment is the cornerstone of evaluation. Plot all available measurements on WHO/IAP growth charts and calculate:
- Weight-for-age z-score (WAZ): useful for overall weight status.
- Weight-for-height z-score (WHZ): most sensitive for acute malnutrition.
- Height-for-age z-score (HAZ): reflects chronic undernutrition (stunting).
- MUAC: quick screening; <11.5 cm in children 6–59 months = SAM.
A child whose weight is declining across centile lines requires urgent attention, while a child tracking along a low centile without decline and with normal development may simply be constitutionally small.
Physical examination: Assess weight, length, head circumference; look for signs of malnutrition (oedema, muscle wasting, hair changes); examine the oral cavity (cleft palate, dental caries, tongue-tie); assess neurodevelopmental status and muscle tone; palpate abdomen (pyloric mass, hepatosplenomegaly); observe a feed if possible.
Investigations are not needed routinely but should be ordered when organic disease is suspected:
- Pyloric stenosis: ultrasound (pyloric muscle thickness >4 mm, channel length >16 mm); serum electrolytes (hypochloraemic, hypokalaemic metabolic alkalosis).
- GORD: usually clinical; upper GI contrast study or pH-impedance monitoring if diagnosis uncertain or complications suspected; oesophagoscopy if oesophagitis suspected.
- CMPA: elimination diet (cow's milk protein–free for 2–4 weeks) followed by oral challenge is the gold standard; skin-prick test and specific IgE for IgE-mediated forms; note that most CMPA in infancy is non-IgE-mediated and allergy tests may be negative.
- Organic disease screen: full blood count, iron studies, serum albumin, thyroid function, swallowing study (video-fluoroscopy) if aspiration is suspected.
Clinical Approach to Feeding Problems in Children
SELF-CHECK
A 5-week-old infant presents with projectile, non-bilious vomiting after every feed for the past two weeks. The infant is hungry and feeds eagerly, but vomits forcefully immediately after. On examination, a small olive-shaped mass is palpable in the right upper quadrant. Serum electrolytes show hypochloraemia and hypokalaemia. What is the most likely diagnosis?
A. Gastro-oesophageal reflux disease
B. Cow's milk protein allergy
C. Hypertrophic pyloric stenosis
D. Intestinal malrotation with volvulus
Reveal Answer
Answer: C. Hypertrophic pyloric stenosis
Hypertrophic pyloric stenosis presents classically at 3–6 weeks with projectile non-bilious vomiting after feeds, an eager hungry infant, a palpable pyloric 'olive', and hypochloraemic hypokalaemic metabolic alkalosis from repeated vomiting of gastric acid. GORD presents with effortless regurgitation. CMPA typically presents with vomiting plus diarrhoea/blood in stool/skin manifestations. Intestinal malrotation/volvulus causes bilious vomiting and is a surgical emergency.