Page 7 of 17
PE5.3 | Temper Tantrums and Pica — SDL Guide
Learning Objectives
- Describe the clinical features and age range of temper tantrums, distinguishing normal developmental behaviour from pathological presentations.
- Define pica and identify the age threshold above which it is considered pathological.
- Explain the associations between pica and iron deficiency, lead poisoning, and neurodevelopmental conditions.
- Outline the investigation and management of pica, including iron supplementation and lead chelation therapy.
INSTRUCTIONS
Temper tantrums and pica are among the most common behavioural concerns encountered in paediatric practice in India. Tantrums are a normal part of toddler development but can escalate into a significant family stressor if mismanaged. Pica — the persistent ingestion of non-food substances — carries real medical risks including iron-deficiency anaemia and lead poisoning, and is frequently a marker of underlying nutritional deficiency or neurodevelopmental disorder. This module equips you to distinguish normal from pathological, identify the correctable causes of pica, and provide evidence-based management for both problems.
References
- Ghai Essential Pediatrics, 9th ed., Ch 17 (Behavioural Problems) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 31 (Feeding and Behaviour) (textbook)
- IAP Textbook of Pediatrics, 6th ed. — Developmental and Behavioural Pediatrics (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In your paediatric outpatient clinic, two consecutive patients present with challenging behaviours. The first is a 2-year-old boy whose mother says 'He screams and throws himself on the floor in public whenever I say no — I cannot take him anywhere.' The second is a 4-year-old girl referred by her general practitioner because her mother noticed her eating mud and sand from the garden repeatedly over the past three months. Her haemoglobin returns at 8.4 g/dL. Are these normal childhood behaviours or red-flag presentations requiring investigation? What is the connection between the girl's soil-eating and her anaemia, and what must you screen for beyond iron deficiency?
WHY THIS MATTERS
Temper tantrums, affecting 50–80% of 2-year-olds, are the most common behavioural concern in toddlerhood. When mismanaged — through parental capitulation or excessive punishment — they escalate into entrenched oppositional behaviour that affects family functioning and school readiness. Pica affects 10–32% of children with intellectual disability and up to 15–27% of children with autism spectrum disorder, but also occurs in otherwise typically developing children who are iron deficient. The medical risks of pica are substantial: iron-deficiency anaemia, lead poisoning (from ingesting paint, kajal, or contaminated soil), parasitic infection, and bowel obstruction. Identifying and treating the underlying cause — most commonly iron deficiency — is transformative. The paediatrician must recognise both conditions early and avoid the twin errors of pathologising normal tantrums and dismissing pica as a mere habit.
RECALL
Before proceeding, recall:
• Developmental autonomy in toddlerhood: between 18 months and 3 years, children develop a sense of self and a drive for independence ('autonomy vs shame and doubt' — Erikson stage 2); this is the psychological substrate of temper tantrums.
• Iron-deficiency anaemia: Hb <11 g/dL in children under 5 years; iron is a cofactor in dopamine receptor synthesis and central nervous system myelination — iron deficiency affects brain function beyond haematopoiesis.
• Lead toxicity: lead inhibits ALA dehydratase and ferrochelatase (haem synthesis enzymes), accumulates in bone and the CNS, causes cognitive impairment; no blood lead level is definitively 'safe'.
• Pica is distinct from normal mouthing: children under 18 months normally mouth objects as part of oral exploration; this is NOT pica — pica requires the behaviour to be persistent (≥1 month) in a child old enough (≥18–24 months) to know the substance is not food.
Clinical Presentation of Temper Tantrums and Pica
This module covers two distinct behavioural problems that are commonly grouped together in the behavioural paediatrics curriculum: temper tantrums and pica. Each has its own clinical presentation, aetiology, and management; they are covered together because both represent normal-to-pathological continua that the paediatrician must be able to navigate at the outpatient level.
Temper tantrums are episodes of emotional dysregulation in young children characterised by crying, screaming, breath-holding (without loss of consciousness or colour change — distinguishing them from BHS), throwing objects, and falling to the floor. They occur almost exclusively in the toddler age range (18 months to 3 years) and represent the child's inability to regulate frustration when their wishes are denied or their communication fails. The frequency peaks at 18–24 months and declines as language develops. They typically last 1–5 minutes and resolve spontaneously. Normal tantrums do not cause injury to the child or others and do not persist beyond age 4–5 years.
Features that suggest a pathological tantrum pattern and require further evaluation include:
• Frequency >5 per day consistently.
• Duration >20–30 minutes regularly.
• Persistence beyond 5 years of age without improvement.
• Tantrums associated with self-injurious behaviour (head-banging, biting self).
• Violent aggression toward others.
• Associated developmental delay or language regression.
• Tantrums occurring at school (suggests generalised regulation difficulty, not just a home context).
Pica is defined as the persistent ingestion of non-food, non-nutritive substances for ≥1 month in a child developmentally older than 18–24 months (the age by which children normally learn that these substances are not food). Common substances ingested vary by region and culture:
• Geophagy (soil, clay, sand) — the most common form in India and Africa; associated with iron and zinc deficiency.
• Plumbism (lead paint, kajal/surma, soil contaminated with lead) — carries the highest medical risk.
• Pagophagia (ice) — strongly associated with iron deficiency.
• Trichophagia (hair) — may cause trichobezoar (hair ball) with gastric outlet obstruction.
• Paper, chalk, plaster, faeces (coprophagia — rare, associated with severe intellectual disability).
The child with pica may present with pallor and fatigue (iron deficiency), developmental delay or cognitive regression (lead poisoning), or abdominal pain and constipation (bezoar or intestinal obstruction).
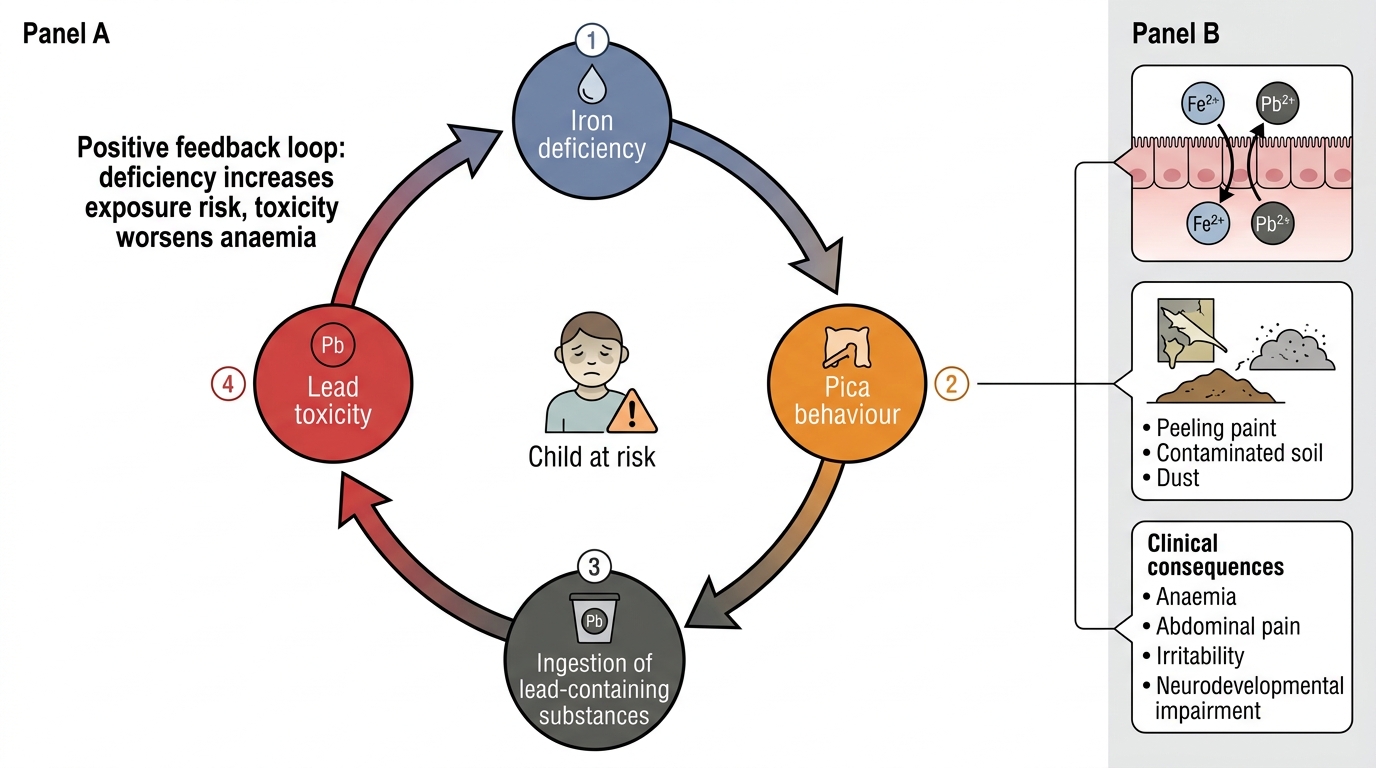
Iron Deficiency, Pica, and Lead Toxicity: Positive Feedback Loop
Pathophysiology and Aetiology
Understanding the underlying mechanisms for both conditions enables targeted management rather than symptomatic control alone. The aetiology of temper tantrums is fundamentally developmental, while pica has both nutritional and neurodevelopmental substrates.
Temper tantrums — developmental aetiology:
Between 18 months and 3 years, the child's prefrontal cortex (responsible for emotional regulation, impulse control, and inhibition) is developmentally immature. The limbic system, particularly the amygdala, generates strong emotional responses, but the cortical circuits that regulate these responses have not yet fully developed or myelinated. When a toddler is frustrated — by a denied request, a failed motor task, or a transition (leaving the playground) — the emotional arousal from the amygdala overwhelms the immature frontal lobe's capacity for regulation, producing the uncontrolled emotional outburst we call a tantrum. Language development is the primary mitigator: as expressive language improves (typically from 18–24 months onward), the child gains an alternative channel for communicating frustration, and tantrum frequency declines. Environmental factors that increase tantrum frequency include hunger, fatigue, excessive demands, inconsistent parenting (intermittent reinforcement of tantrums), and sensory overstimulation.
Pica — multifactorial aetiology:
The aetiology of pica is not fully understood but several mechanisms have been proposed, the most important of which are:
Iron deficiency: Iron is a cofactor in the synthesis of dopamine receptors in the CNS. Iron-deficient children show altered dopaminergic signalling, which is thought to produce abnormal cravings or reduce the aversion to non-food substances. Iron supplementation resolves pica in the majority of iron-deficient children — this is the strongest evidence for a direct causal link. Pagophagia (ice-eating) is particularly closely linked to iron deficiency.
Neurodevelopmental conditions: Pica is significantly more common in children with intellectual disability (prevalence 10–32%) and autism spectrum disorder (prevalence 15–27%). In these children, the mechanism relates to impaired sensory processing, reduced social learning (not learning that a substance is inedible), and restricted/repetitive behaviour patterns.
Nutritional deficiency beyond iron: Zinc deficiency and calcium deficiency have been associated with geophagy in some studies, though the evidence is less robust than for iron.
Psychosocial factors: Neglect, poverty, food insecurity, and parental mental illness are associated with pica, particularly in developing country settings. Stress and anxiety may also trigger or perpetuate pica.
Lead poisoning — a consequence of pica: Children who ingest lead-containing substances (flaking paint from old buildings, kajal/surma, contaminated soil) develop lead poisoning. Lead inhibits ALA dehydratase and ferrochelatase (enzymes in haem synthesis), causing a hypochromic microcytic anaemia that mimics — and coexists with — iron deficiency. Lead also crosses the blood-brain barrier, accumulates in the developing CNS, and causes irreversible neurotoxic injury: impaired cognition, reduced IQ, attention deficits, and behavioural problems. Critically, iron deficiency increases lead absorption from the gut by upregulating the DMT-1 transporter (which absorbs both Fe²⁺ and Pb²⁺); thus, iron-deficient children who develop pica and ingest lead-containing substances are at heightened risk of lead toxicity — creating a dangerous amplifying loop.
SELF-CHECK
A 3-year-old girl from a low-income household has been eating mud and clay from the garden for the past 4 months. Her haemoglobin is 8.2 g/dL with microcytic hypochromic red cells. Which of the following investigations is MOST urgently required beyond a serum ferritin?
A. Bone marrow biopsy
B. Blood lead level
C. Serum zinc level
D. Stool culture for parasites
Reveal Answer
Answer: B. Blood lead level
Pica with geophagy in the context of iron-deficiency anaemia mandates blood lead level measurement, as soil and clay ingestion frequently introduces lead. Iron deficiency itself increases intestinal lead absorption via the DMT-1 transporter, compounding the risk. Lead neurotoxicity at BLL ≥5 µg/dL requires environmental investigation and follow-up; BLL ≥45 µg/dL requires DMSA chelation. Bone marrow biopsy is not indicated. Zinc and stool cultures may be relevant but are secondary to ruling out lead poisoning, which has irreversible neurocognitive consequences.
Diagnosis and Investigation
The diagnostic approach integrates a structured history to characterise the tantrum pattern or pica behaviour, targeted investigations for correctable causes of pica, and developmental assessment to identify underlying neurodevelopmental conditions.
History for temper tantrums should document: frequency (tantrums per day), duration, nature of triggers (specific situations or pervasive), presence of self-injurious or aggressive behaviour, family response (what happens after the tantrum — does the child get what they wanted?), and developmental milestones including expressive language. Parental stress levels and consistency of parenting responses should be explored, as inconsistent responses are the most powerful perpetuating factor.
History for pica should document: what substance is being ingested (is it soil, paint, ice, hair?), frequency, duration (≥1 month), access to identified substances in the home or environment, associated symptoms (pallor, fatigue, abdominal pain, developmental regression), dietary history (foods offered, refusal, overall variety), and family/social circumstances.
Physical examination for pica: assess weight, height, MUAC; look for pallor (conjunctival, palmar — iron deficiency or lead-related anaemia); gingival lead line (Burton's line — a blue-black line on the gum margin in chronic lead poisoning, more visible in poor oral hygiene); trichophagy may reveal a bezoar on abdominal examination (palpable epigastric mass); developmental assessment for intellectual disability and ASD features.
Investigations for pica:
All children with pica should have:
• Full blood count and serum ferritin — to screen for iron-deficiency anaemia; hypochromic microcytic anaemia with low ferritin confirms IDA.
• Blood lead level (BLL) — essential if geophagy, paint/kajal ingestion, or other lead exposure is possible; normal <5 µg/dL (CDC reference value 2012).
Additional investigations based on findings:
• Serum zinc and calcium if geophagy persists after iron correction.
• Abdominal X-ray if trichobezoar or intestinal obstruction is suspected (opaque hair mass).
• Developmental screening (Developmental Screening Test/DASII, M-CHAT for ASD) if neurodevelopmental concerns.
• Peripheral blood smear: look for basophilic stippling of red cells (characteristic of lead poisoning) alongside microcytic hypochromic morphology.
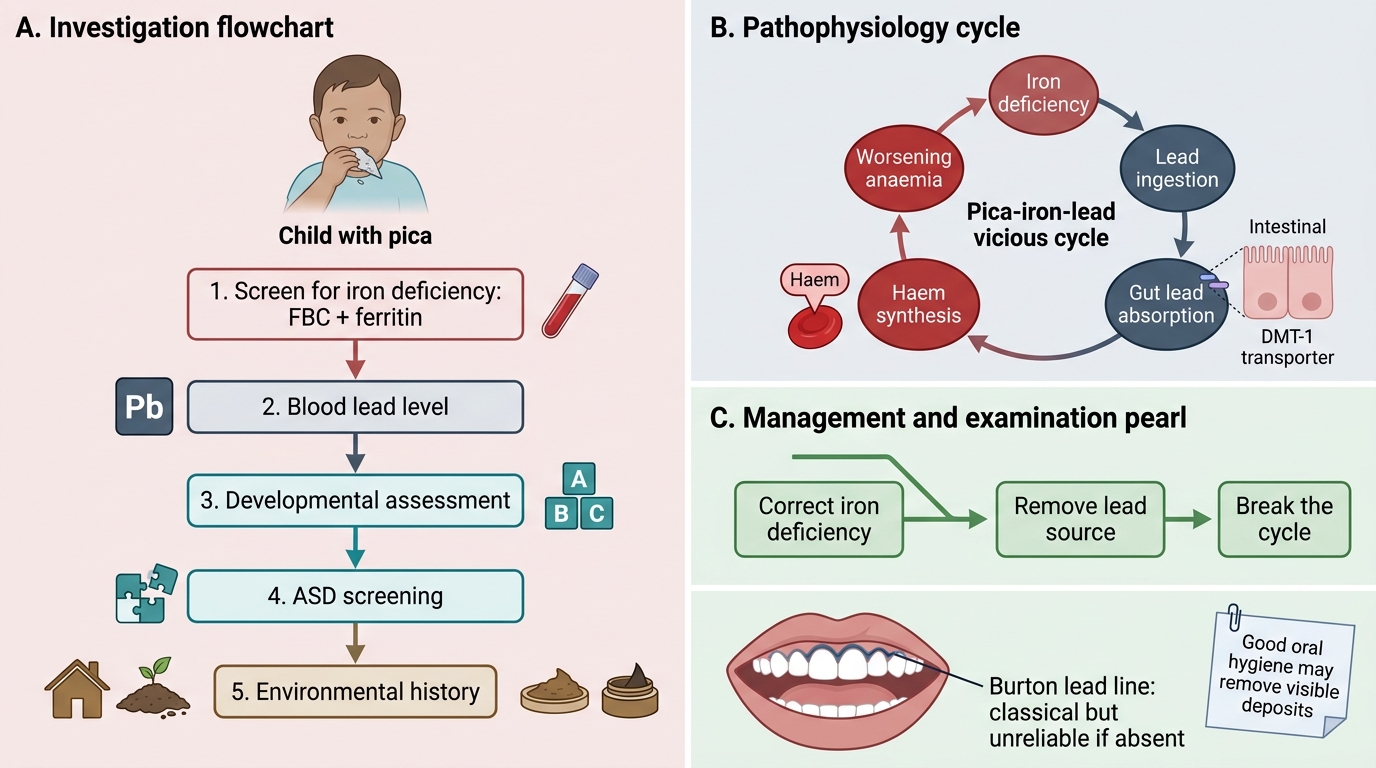
Clinical Investigation Flowchart for a Child with Pica
CLINICAL PEARL
Pica and iron deficiency form a vicious cycle. Iron-deficient children develop pica; if they eat soil or kajal (which often contains lead), their iron-deficient gut absorbs more lead via the DMT-1 transporter; lead inhibits haem synthesis, worsening the anaemia; and the worsening iron deficiency perpetuates the pica. Breaking the cycle requires both correcting the iron deficiency AND eliminating access to the lead-containing substance. Simply treating the anaemia without addressing the environmental lead source, or removing the substance without treating the iron deficiency, is incomplete management. Also: the gingival Burton's lead line (blue-black gum margin) is a classical examination finding in chronic lead poisoning — but it is only visible when gum hygiene is poor (the lead sulphide deposits are washed away by good oral hygiene). Do not rely on its absence to exclude lead poisoning.