Page 10 of 28
PE6.5 | Adolescent Eating Disorders — SDL Guide (Part 2)
Medical Complications of Eating Disorders
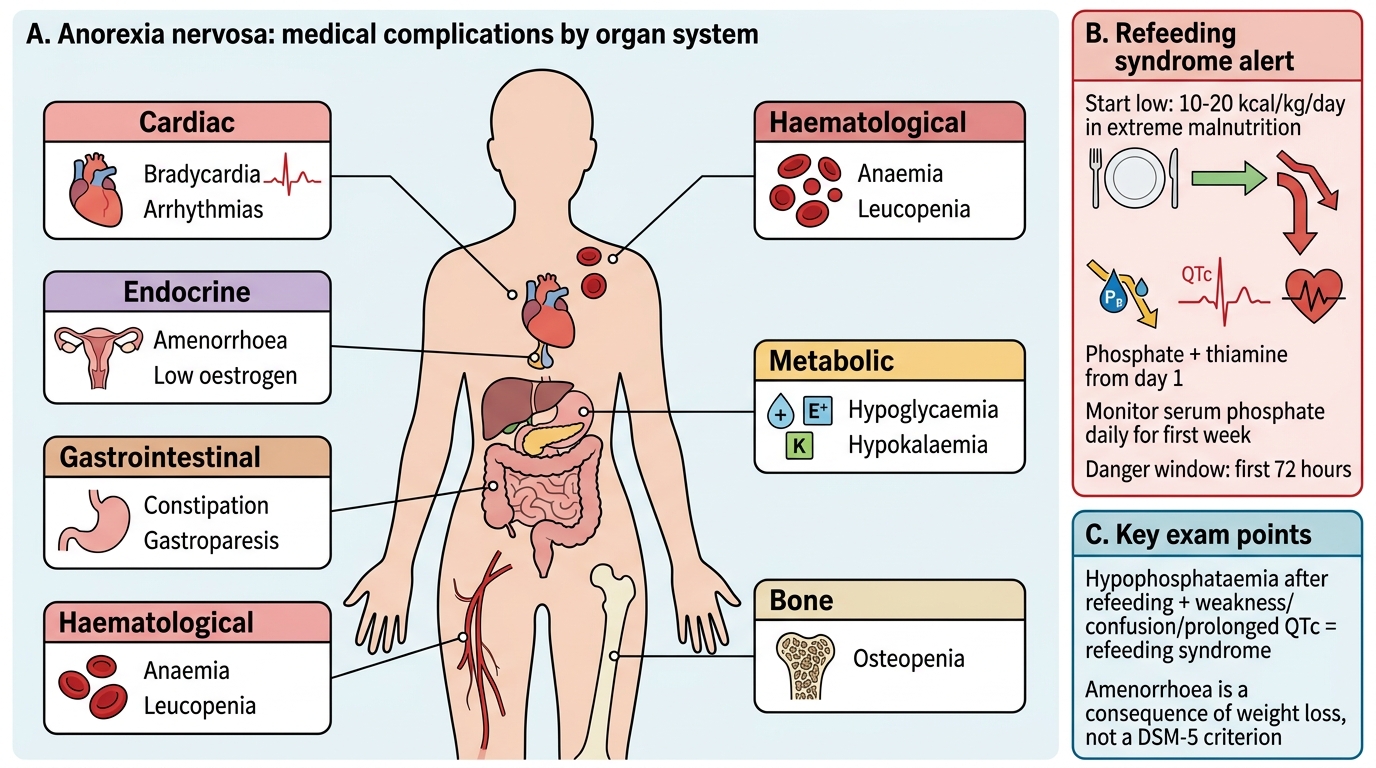
The medical complications of eating disorders are systemic, progressive, and in the most severe cases, fatal. Anorexia nervosa affects virtually every organ system through the combined consequences of starvation (caloric deficit), micronutrient deficiency, hormonal dysregulation from hypothalamic suppression, and in the binge-purge subtype, the additional burden of electrolyte disturbances from purging. Bulimia nervosa produces a more targeted set of complications concentrated in the cardiovascular, dental, gastrointestinal, and electrolyte domains. Understanding these complications serves two purposes: first, to determine who needs urgent inpatient admission (haemodynamic instability, dangerous electrolyte disturbances); and second, to monitor for the emergence of new complications during the treatment and recovery process. A systematic organ-by-organ approach ensures nothing is missed in the initial assessment.
Complications of Anorexia Nervosa — organ-system approach:
- Cardiovascular: bradycardia (most common — resting HR <50 bpm in severe cases), hypotension, prolonged QTc interval (risk of ventricular arrhythmias and sudden death), decreased cardiac muscle mass, mitral valve prolapse
- Endocrine: amenorrhoea (hypothalamic suppression of GnRH → low LH/FSH → low oestrogen), low T3/T4 (euthyroid sick), hypercortisolaemia, growth retardation if onset pre-pubertal
- Bone: osteopenia and osteoporosis from prolonged oestrogen deficiency and low IGF-1; fracture risk elevated; bone loss may be irreversible even after recovery
- Gastrointestinal: constipation, delayed gastric emptying (gastroparesis), superior mesenteric artery (SMA) syndrome, elevated liver enzymes
- Haematological: anaemia, leucopenia (neutropenia), thrombocytopenia from bone marrow suppression
- Neurological: peripheral neuropathy, cognitive impairment (concentration, memory)
- Metabolic: hypoglycaemia, hypothermia, dehydration
Complications specific to BN (purging behaviours):
- Russell's sign: as described above — callusing of dorsal hand
- Hypokalaemia: from repeated vomiting or laxative use → cardiac arrhythmias, muscle weakness; potentially life-threatening
- Metabolic alkalosis: from loss of hydrochloric acid via vomiting
- Dental erosion: enamel loss on lingual surfaces of upper teeth from gastric acid exposure
- Parotid/salivary gland hypertrophy: bilateral asymptomatic enlargement
- Mallory-Weiss tear: oesophageal mucosal tear from forceful repeated vomiting
- Peripheral oedema: from electrolyte disturbances or after stopping laxatives
Refeeding Syndrome — a critical complication of treatment:
Refeeding syndrome is a potentially fatal metabolic complication that occurs when nutrition is reintroduced — whether orally, enterally, or parenterally — to a severely malnourished patient. During prolonged starvation, the body depletes intracellular electrolytes (phosphate, potassium, magnesium) while maintaining serum levels. On refeeding, carbohydrate intake stimulates insulin release, which drives phosphate, potassium, and magnesium from the extracellular to the intracellular compartment, causing sudden and potentially dangerous drops in serum levels. The defining feature is hypophosphataemia (serum phosphate <0.5 mmol/L in severe cases), which causes:
- Cardiac: arrhythmias, heart failure
- Neurological: confusion, seizures, Wernicke's encephalopathy (if thiamine not co-supplemented)
- Haematological: haemolytic anaemia, leukocyte dysfunction
- Respiratory: respiratory muscle weakness, failure to wean from ventilation
Prevention: refeeding must begin at a LOW caloric intake (10–20 kcal/kg/day initially), with gradual escalation ('start low, go slow'), close monitoring of serum phosphate, potassium, and magnesium, and prophylactic thiamine supplementation. Never increase calorie intake rapidly in a severely malnourished patient.
Medical Complications of Anorexia Nervosa
CLINICAL PEARL
Refeeding syndrome alert: When starting nutritional rehabilitation in a severely malnourished AN patient, NEVER increase calories rapidly. Begin at 10–20 kcal/kg/day (for extreme cases) with phosphate and thiamine supplementation from day 1. Monitor serum phosphate daily for the first week. Hypophosphataemia can cause fatal cardiac arrhythmias within the first 72 hours of refeeding if calories are escalated too quickly. The NICE guidelines recommend increasing calories by no more than 200–300 kcal every 3–4 days in very severe cases. Also remember: amenorrhoea is a consequence of weight loss in AN, not a DSM-5 criterion (it was removed in DSM-5). Do not tell a male patient or a post-menopausal woman that they 'cannot have AN' because of the absence of amenorrhoea.
SELF-CHECK
A 14-year-old girl with anorexia nervosa (BMI 14.2 kg/m²) is admitted for nutritional rehabilitation. On day 3 of refeeding, she develops weakness, confusion, and an ECG shows a prolonged QTc interval. Her serum phosphate is 0.3 mmol/L. What is the MOST likely diagnosis?
A. Hypoglycaemia from inadequate calorie intake
B. Refeeding syndrome from rapid reintroduction of nutrition causing hypophosphataemia
C. Hypokalaemia from purging behaviour during the admission
D. Superior mesenteric artery syndrome from rapid gastric filling
Reveal Answer
Answer: B. Refeeding syndrome from rapid reintroduction of nutrition causing hypophosphataemia
Refeeding syndrome is characterised by hypophosphataemia (and often hypokalaemia/hypomagnesaemia) that occurs on reintroduction of nutrition in a severely malnourished patient. During starvation, intracellular electrolytes are depleted while serum levels are maintained. On refeeding, carbohydrate stimulates insulin release, which drives phosphate intracellularly, causing sudden hypophosphataemia. The consequences include cardiac arrhythmias (QTc prolongation, ventricular fibrillation), neurological dysfunction (confusion, Wernicke's encephalopathy if thiamine not given), and haematological complications. Serum phosphate <0.5 mmol/L is the cardinal finding. Management: slow the rate of feeding, give IV/oral phosphate, supplement thiamine, monitor closely. This is a preventable complication — refeeding should always begin slowly in severely malnourished patients.
Management of Adolescent Eating Disorders
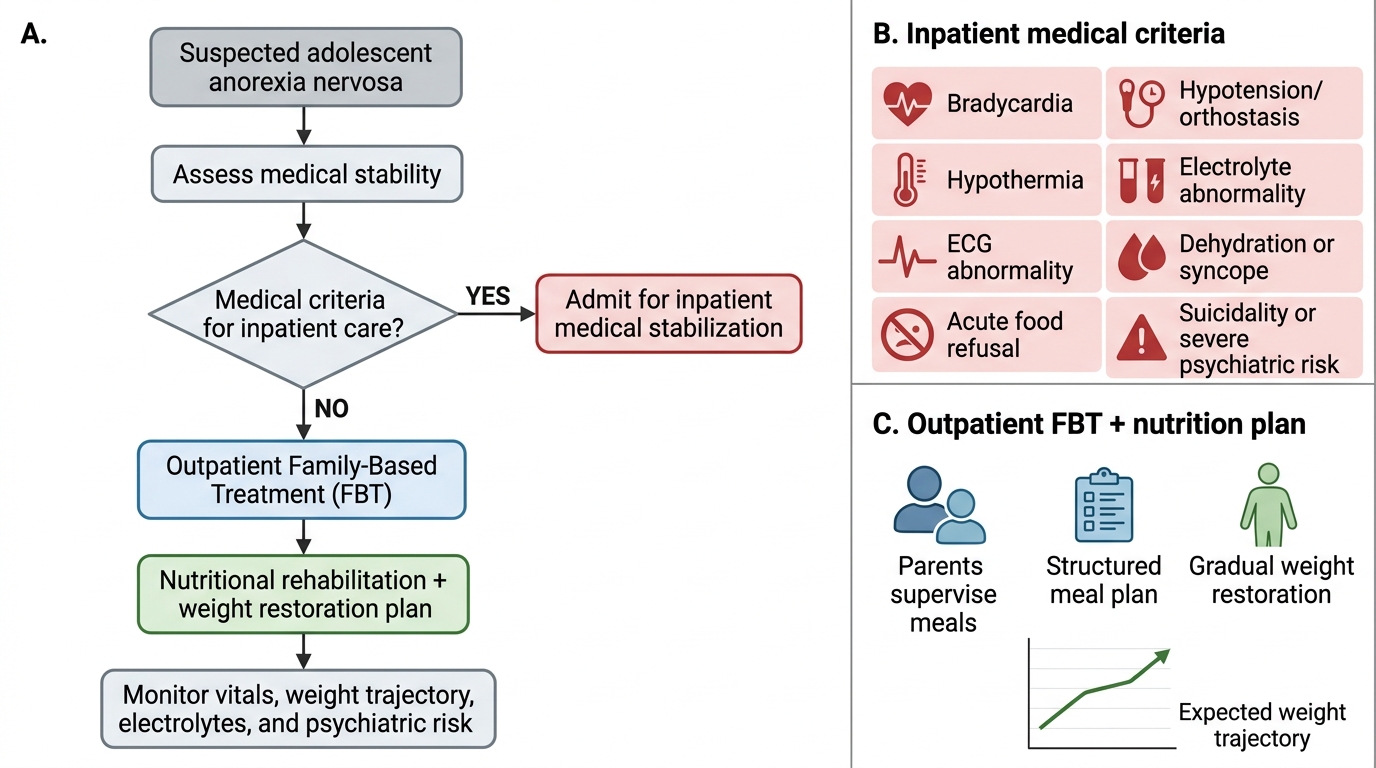
Management of adolescent eating disorders is fundamentally different from the management of most paediatric medical conditions because the illness is simultaneously a medical emergency (in severe cases) and a psychiatric disorder that the patient typically does not want treated. Effective management therefore requires a structured multidisciplinary team — paediatrician, psychiatrist or psychologist, dietitian, and social worker — each addressing a different dimension of the illness. No single professional can manage AN or BN in isolation. The initial clinical decision that structures the entire treatment pathway is the triage question: does this patient require inpatient hospital admission for medical stabilisation, or is outpatient treatment safe and feasible? This decision depends on the presence or absence of haemodynamic instability, dangerous electrolyte disturbances, extreme weight loss, or failed prior outpatient treatment.
Indications for inpatient hospitalisation in AN:
- Heart rate <50 bpm; QTc prolongation; syncope or cardiac arrhythmia
- Systolic BP <90 mmHg, or orthostatic hypotension
- BMI <15 kg/m² (extreme severity) or rapid weight loss (>1 kg/week)
- Serum potassium <3.0 mmol/L; phosphate <0.5 mmol/L
- Temperature <36°C
- Intractable vomiting; inability to maintain oral intake
- Suicidal ideation or severe psychiatric comorbidity
- Failed outpatient management
Family-Based Treatment (FBT, Maudsley Approach): the current gold-standard outpatient treatment for AN in adolescents. FBT is a three-phase manualised family therapy approach:
- Phase 1 (externalisation and weight restoration): parents are empowered to take complete charge of their child's nutrition, with the therapist externalising the eating disorder as an external enemy the family is fighting together. The patient is not blamed. Weight restoration to healthy range is the primary goal.
- Phase 2 (returning control to the adolescent): as weight is restored and medical stability is achieved, nutritional control is gradually returned to the adolescent.
- Phase 3 (establishing healthy identity): supporting the adolescent to develop an identity independent of the eating disorder.
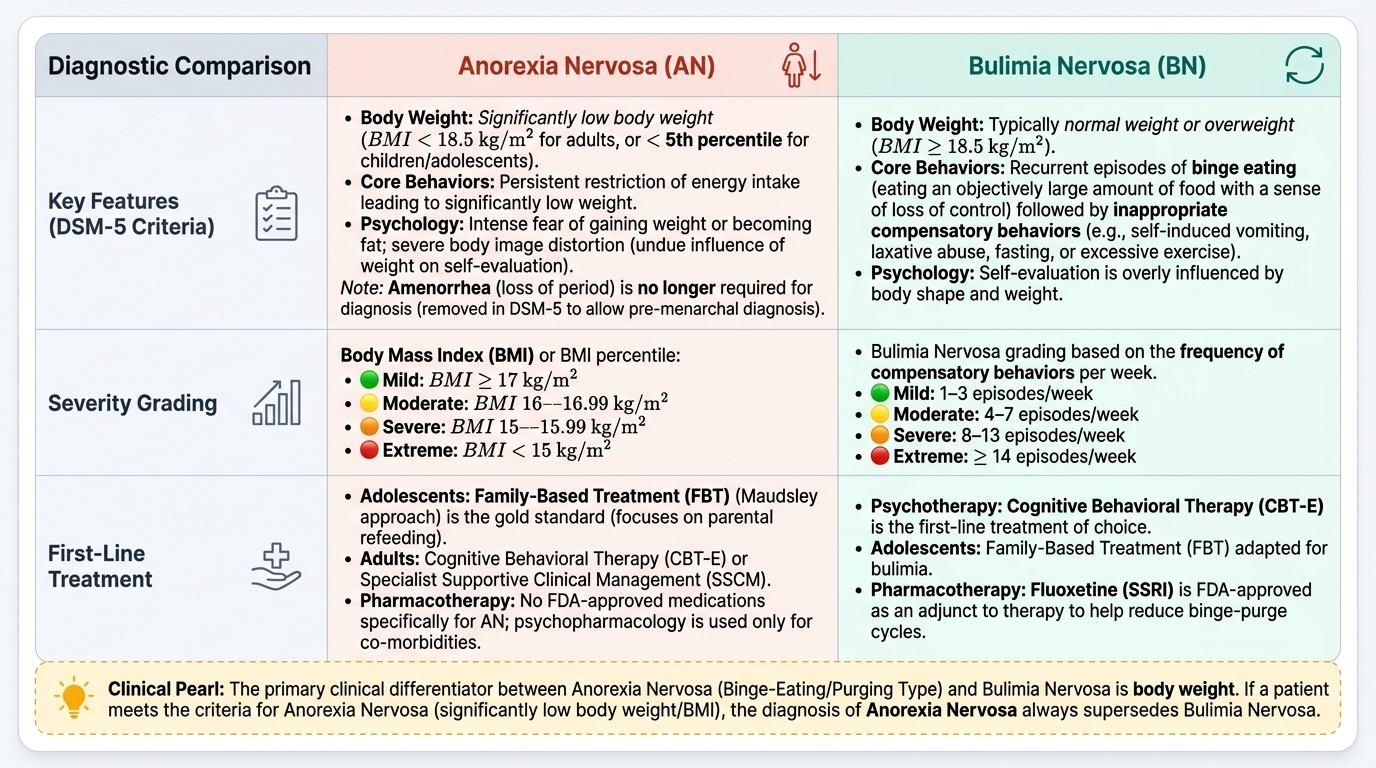
FBT has the strongest evidence base for AN in adolescents (randomised controlled trials showing superior outcomes compared to individual therapy at this age group). It is different from adult treatment, which typically uses Cognitive Behavioural Therapy for Eating Disorders (CBT-E).
Nutritional rehabilitation is the cornerstone of medical management. Goals:
- For inpatients: supervised meals, nasogastric feeding if oral intake insufficient, refeeding starting at 10–20 kcal/kg/day with escalation as tolerated
- Target weight gain: 0.5–1 kg/week for inpatients, 0.5 kg/week for outpatients
- Micronutrient supplementation: thiamine, phosphate, zinc, vitamin D, calcium
- Weight restoration restores menstruation in most patients (no hormone replacement is needed primarily)
Management of BN: the evidence-based treatment is Cognitive Behavioural Therapy (CBT-E) delivered individually or in guided self-help format. Fluoxetine 60 mg/day (SSRI) is the ONLY medication with FDA approval specifically for BN and is used as an adjunct to CBT or as monotherapy when therapy is unavailable. FBT also has evidence for BN in adolescents.
Pharmacotherapy in AN: no medication is approved for AN itself. Pharmacotherapy targets comorbidities — antidepressants for depression, anxiolytics if needed, olanzapine occasionally used for severe obsessive features (modest evidence). Avoid medications that prolong QTc in a patient already at cardiac risk.
| Criteria | Inpatient Admission | Outpatient Management |
|---|---|---|
| Vital signs | HR <50, SBP <90, QTc prolonged | Medically stable, HR >50, SBP stable |
| Weight | BMI <15 or rapid weight loss | BMI ≥15, slow/stable loss |
| Electrolytes | K <3.0, PO₄ <0.5 | Within safe range with monitoring |
| Oral intake | Unable to maintain | Some oral intake achievable |
| Psychiatry | Suicidal ideation, severe comorbidity | No imminent risk, partial insight |
| Treatment response | Failed outpatient | First presentation, motivated family |
Initial Management Decision in Adolescent Anorexia Nervosa
Self-Assessment — Adolescent Eating Disorders
Test your diagnostic and management reasoning with these scenario-based questions.
Provided image
Question 1: A 13-year-old girl has restricted her eating for 4 months and lost 8 kg. She has intense fear of becoming fat and sees herself as 'still needing to lose weight' despite having a BMI at the 3rd percentile. She has not yet had her first period (pre-menarchal). Can she be diagnosed with anorexia nervosa?
Answer: YES. DSM-5 removed amenorrhoea as a required criterion for AN. She meets Criteria A (significant restriction leading to low weight), B (intense fear of weight gain), and C (body image distortion). Pre-menarchal status does not prevent the diagnosis — this is one reason DSM-5 removed the amenorrhoea requirement.
Question 2: What is the minimum DSM-5 frequency criterion for a diagnosis of bulimia nervosa?
Answer: Binge eating AND compensatory behaviour occurring at least once per week for at least 3 months.
Question 3: What is the first investigation you must obtain before starting nutritional rehabilitation in a severely malnourished adolescent with AN, and what complication are you trying to prevent?
Answer: Serum phosphate (along with potassium, magnesium, and an ECG). You are trying to identify baseline electrolyte status to prevent refeeding syndrome — the potentially fatal hypophosphataemia that occurs when carbohydrate is reintroduced in a starved patient.
SELF-CHECK
Which of the following DSM-5 changes from DSM-IV is MOST clinically significant for diagnosing eating disorders in adolescents?
A. Addition of binge eating disorder as a distinct diagnosis
B. Removal of amenorrhoea as a required criterion for anorexia nervosa — allowing diagnosis in pre-menarchal girls, males, and post-menopausal women
C. Lowering the frequency threshold for bulimia nervosa from twice weekly to once weekly
D. Addition of the binge-purge subtype to anorexia nervosa
Reveal Answer
Answer: B. Removal of amenorrhoea as a required criterion for anorexia nervosa — allowing diagnosis in pre-menarchal girls, males, and post-menopausal women
The removal of amenorrhoea as a required (criterion D) diagnosis of AN in DSM-5 is the most clinically significant change for adolescent practice. In DSM-IV, amenorrhoea was required for the AN diagnosis, which meant pre-menarchal girls (who have not yet had their first period), biological males, and post-menopausal women could not technically receive the diagnosis — despite meeting all other clinical criteria. DSM-5 corrects this by removing the amenorrhoea criterion and expanding the definition to include all patients meeting criteria A, B, and C. This allows earlier diagnosis in young adolescent girls before menarche and in male adolescents with eating disorders (who were significantly under-diagnosed under DSM-IV). Note: binge eating disorder was indeed added as a distinct category in DSM-5 (option A), and the frequency for BN was lowered from twice to once weekly (option C) — but these are less clinically significant for adolescent paediatric practice than the amenorrhoea removal.