Page 12 of 28
PE6.6 | Adolescent Mental Health — SDL Guide
Learning Objectives
- Describe the clinical presentations of depression, anxiety disorders, ADHD, and suicidal ideation/self-harm in adolescents
- Apply the DSM-5 criteria for major depressive disorder (including adolescent-specific modifications) and generalised anxiety disorder
- Use the PHQ-A screening tool to identify adolescent depression and interpret the severity score
- Assess suicide risk in an adolescent using a systematic framework and describe the appropriate clinical response
- Describe the evidence-based management of adolescent depression including the role of fluoxetine and CBT
INSTRUCTIONS
Half of all lifetime mental health disorders begin before age 14. Adolescents with depression miss school, drop out, develop substance use disorders, and die by suicide. Yet depression and anxiety in this age group are routinely missed in primary care — partly because adolescents present atypically (irritability rather than sadness, somatic complaints rather than psychological language) and partly because clinicians are not trained to screen for them. This module gives you the DSM-5 criteria, the validated screening tools, the suicide risk assessment framework, and the first-line management approach for the most prevalent adolescent mental health conditions you will encounter in clinical practice.
References
- Ghai Essential Pediatrics, 9th ed., Chapter on Adolescent Health — Mental Health (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Chapter on Mood Disorders, Anxiety, and ADHD in Adolescents (textbook)
- DSM-5 — Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, APA, 2013 (classification)
- IAP Standard Treatment Guidelines — Adolescent Mental Health, 2022 (guideline)
- Mental Healthcare Act 2017, Ministry of Health and Family Welfare, Government of India (law)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 15-year-old boy is referred to you by his school counsellor because his grades have dropped from A's to C's over the past three months, he has been missing school frequently, and he got into two fights last week — something that was never his pattern before. His mother, who came with him reluctantly, says he has 'just become lazy and disrespectful.' The boy himself says he is 'fine' but avoids eye contact and responds in monosyllables. On direct questioning, he admits he has been sleeping 12 hours a day and still feels tired, has stopped playing football which he used to love, and has been eating very little. When you ask if he has ever had thoughts of hurting himself, there is a long pause before he says 'sometimes.' How do you proceed?
WHY THIS MATTERS
Mental health disorders are among the leading causes of disability in adolescence worldwide. According to the WHO, approximately 50% of all lifetime mental health disorders have their onset before age 14, and 75% before age 24 — making adolescence the critical window for detection and early intervention. In India, the National Mental Health Survey (NMHS, 2015–16) found that 7.3% of adolescents aged 13–17 years met criteria for a mental disorder, with depressive disorders being the most prevalent. Despite this burden, the treatment gap in India remains enormous: fewer than 10% of affected adolescents receive any treatment. Suicide is among the leading causes of death in Indian adolescents — the Mental Healthcare Act 2017 decriminalised suicide attempts, recognising suicide as a public health rather than a criminal issue. The clinician in primary care is often the only healthcare professional an adolescent will encounter; systematic screening and timely referral are the difference between early intervention and a preventable death.
RECALL
Recall from your Psychiatry rotation the basic concepts of major depressive disorder: the symptom criteria, the minimum duration (2 weeks), and the requirement that symptoms cause functional impairment. Recall that in children and adolescents, mood disorders often present differently from adults — irritability may be the primary mood presentation rather than sadness, and somatic complaints (headache, abdominal pain, fatigue) may dominate the picture. Recall from the HEEADSSS framework (pe5-adolescent-development SDL) that the 'S' for Suicide/depression is one of the most sensitive domains — always probe it directly in an adolescent clinical encounter. Recall the Mental Healthcare Act 2017: a suicide attempt is no longer a criminal offence in India, and persons who attempt suicide are to be rehabilitated, not punished.
Clinical Presentation of Common Adolescent Mental Health Disorders
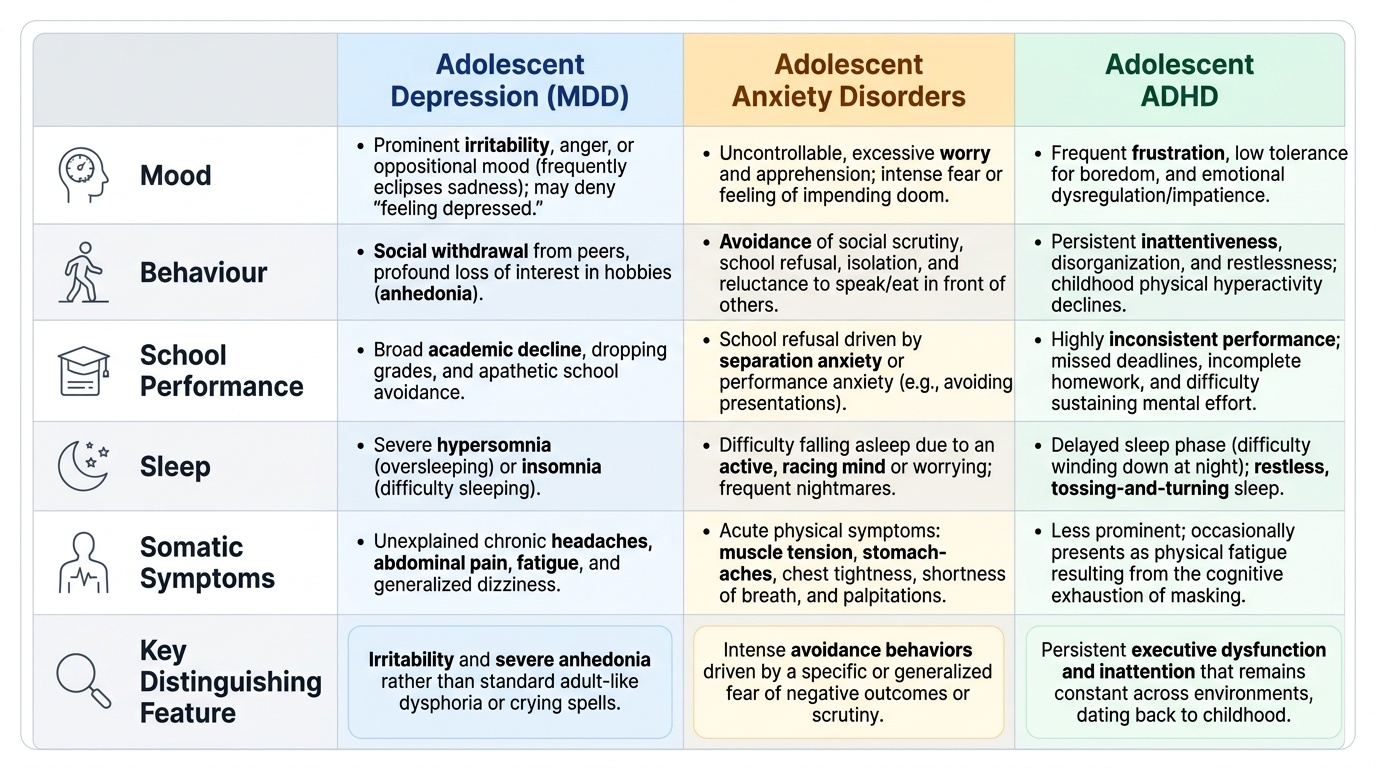
Adolescent mental health disorders frequently present with clinical features that differ substantially from the textbook adult picture, creating diagnostic challenges for clinicians trained on adult psychiatry presentations. Understanding these adolescent-specific presentations is the first step towards reliable clinical recognition.
Provided image
Major Depressive Disorder (MDD) in adolescents: unlike adults who classically present with sadness, low mood, and tearfulness, depressed adolescents often present with irritability as the dominant mood feature — they appear angry, oppositional, or difficult rather than sad. Academic decline (dropping grades, school avoidance), social withdrawal from peer activities, loss of interest in previously enjoyed hobbies, hypersomnia (sleeping excessively) or insomnia, and unexplained somatic complaints (headache, abdominal pain, fatigue, dizziness) are common presenting features. The adolescent may deny 'feeling depressed' entirely — probing for anhedonia (loss of interest and pleasure) is often more revealing than asking about mood.
Anxiety disorders are the most prevalent category of mental health disorders in adolescence. Common presentations include:
- Generalised Anxiety Disorder (GAD): excessive, uncontrollable worry across multiple domains (academic performance, social situations, family matters, health, future) that the adolescent cannot turn off, associated with physical symptoms (headache, muscle tension, fatigue, difficulty sleeping, stomach-aches).
- Social anxiety disorder: intense fear of social situations and scrutiny by others, leading to school refusal, avoidance of presentations, inability to eat in front of others, isolation from peers.
- Separation anxiety: persistent fear of separation from attachment figures (parents), most common in early adolescence; causes school refusal with multiple somatic complaints on school mornings.
- Panic disorder: recurrent unexpected panic attacks (intense fear + physical symptoms: palpitations, shortness of breath, chest tightness, dizziness, feeling of impending doom), often misdiagnosed as cardiac or respiratory disease.
ADHD in adolescence: the hyperactive features of childhood ADHD (running, climbing, excessive talking) often diminish by adolescence, while inattentive features persist (difficulty sustaining attention, forgetfulness, disorganisation, losing things, distractibility). Adolescents with ADHD characteristically have academic underperformance inconsistent with their tested intelligence, difficulty completing tasks, and impulsivity that contributes to risk-taking behaviour. ADHD is frequently comorbid with depression and anxiety.
Suicidal ideation and self-harm: any adolescent presenting with unexplained school decline, social withdrawal, irritability, or somatic complaints should be directly and calmly asked about self-harm and suicidal ideation. Non-suicidal self-injury (NSSI) — superficial cutting or burning, usually on the forearms, as an emotional regulation strategy — must be distinguished from suicidal self-harm by intent.
SELF-CHECK
A 14-year-old girl is brought to the OPD. Her mother says she has become 'moody and irritable' over the past 3 weeks, is sleeping 10–11 hours, has stopped attending her dance classes, has no appetite, and appears socially withdrawn. The girl says she doesn't feel 'sad.' Which DSM-5 modification allows you to consider a diagnosis of major depressive disorder in this adolescent?
A. The 2-week duration criterion is reduced to 1 week for adolescents
B. In children and adolescents, irritability can substitute for depressed mood as the core mood criterion for MDD
C. Anhedonia is not required for MDD in children — only 4 of 9 symptoms are needed
D. MDD cannot be diagnosed in adolescents who deny feeling sad — they must be referred to psychiatry first
Reveal Answer
Answer: B. In children and adolescents, irritability can substitute for depressed mood as the core mood criterion for MDD
DSM-5 includes an adolescent-specific modification for major depressive disorder: in children and adolescents, IRRITABILITY may substitute for DEPRESSED MOOD as one of the two required core symptoms (the other being anhedonia). This recognises the well-established observation that depressed adolescents often present with irritability, oppositional behaviour, or anger rather than subjective sadness. This girl has: irritability (core mood criterion, DSM-5 adolescent modification) + hypersomnia + anhedonia (stopped dance classes) + reduced appetite + social withdrawal — that is ≥5 symptoms for ≥3 weeks, meeting MDD criteria. The 2-week duration criterion applies to both adults and adolescents. Anhedonia remains a core criterion in all ages.
Pathophysiology and Aetiology of Adolescent Mental Health Disorders
Adolescent mental health disorders arise from the interaction of neurobiological vulnerabilities with psychological and sociocultural stressors — a biopsychosocial model that is both scientifically supported and clinically useful for explaining the illness to families.
Neurobiological factors: the adolescent brain is in a state of active remodelling. The prefrontal cortex — responsible for impulse control, emotional regulation, and executive function — is the last brain region to mature, with full myelination and synaptic pruning not complete until the mid-20s. In contrast, the limbic system (including the amygdala, the emotional centre) matures earlier. This developmental imbalance creates a biological substrate for emotional dysregulation and risk-taking. The hypothalamic-pituitary-adrenal (HPA) axis dysregulation — characterised by elevated cortisol and blunted stress reactivity — is consistently found in adolescent depression. Monoamine neurotransmitter systems (serotonin, dopamine, norepinephrine) also show developmental changes that interact with the pathophysiology of depression and anxiety.
Genetic factors: the heritability of depression is approximately 37% in adolescents (lower than in adults, where environmental factors become less dominant relatively). First-degree relatives of individuals with depression have 2–3 times the risk. The genetic risk is largely non-specific — variants associated with depression also confer risk for anxiety, substance use, and neurodevelopmental disorders.
Psychological factors: negative cognitive schemas — the tendency to interpret events as reflecting one's own inadequacy, to catastrophise outcomes, and to discount positive evidence — are the psychological core of depressive vulnerability (Beck's cognitive model). Adverse childhood experiences (ACEs) — abuse, neglect, domestic violence, household substance use — are the strongest environmental predictors of adolescent depression and suicide risk. Perfectionism and low self-esteem amplify vulnerability, especially in the context of academic pressure.
Sociocultural factors unique to adolescence: academic performance pressure (high-stakes examinations, parental expectations), peer comparison and peer rejection, bullying (including cyberbullying), and social media exposure (association with depression from social comparison, disrupted sleep from late-night use, and cyberbullying) are all established risk factors. In India, additional factors include family socioeconomic stress, migration-related family disruption, and gender-based discrimination.
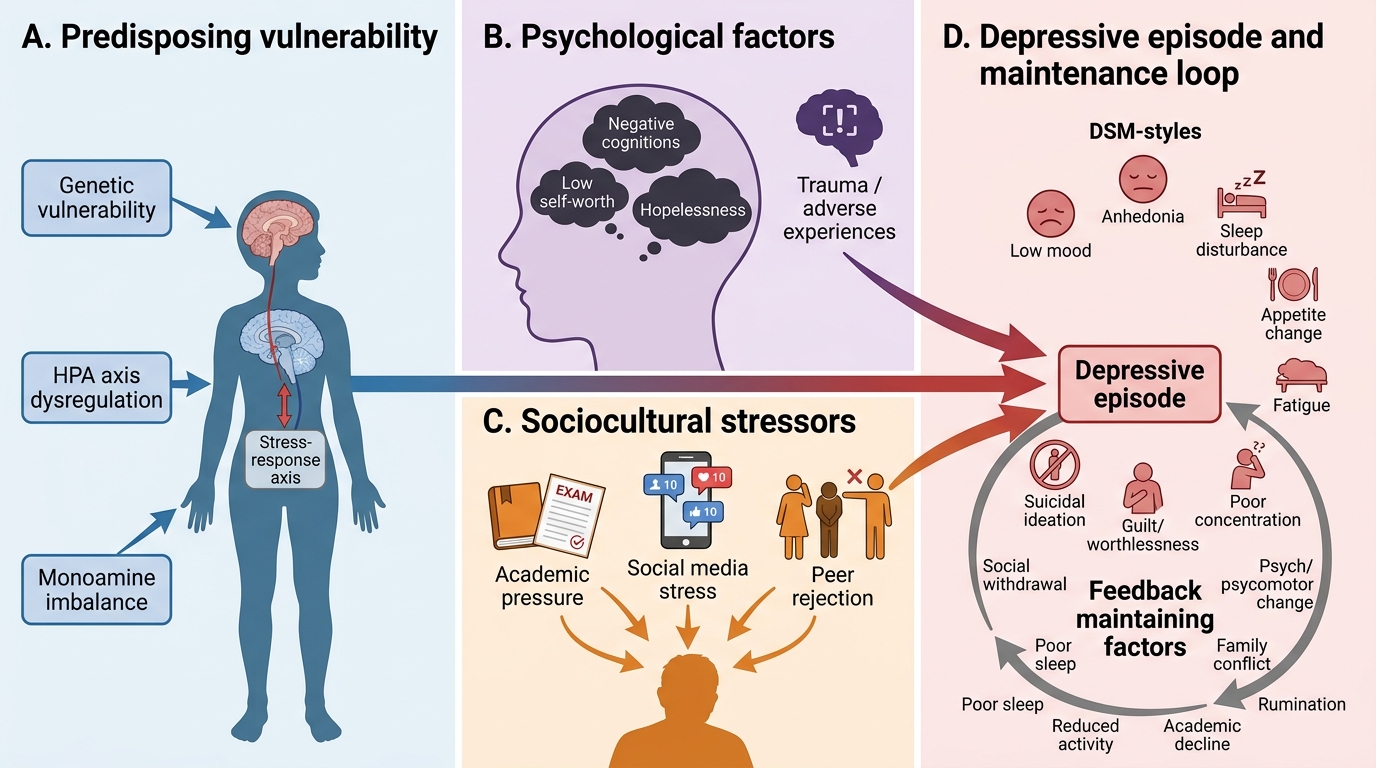
Biopsychosocial Model of Adolescent Depression
Diagnosis — DSM-5 Criteria and Screening Tools
Reliable diagnosis of adolescent mental health disorders requires both a systematic application of the DSM-5 diagnostic criteria and the judicious use of validated screening tools that are appropriate for the developmental level and the clinical setting. In the time-pressured primary-care adolescent encounter, the clinician needs a structured framework — not an informal impression — to move from clinical suspicion to a provisional diagnosis and a treatment plan. The two highest-priority conditions to diagnose in this setting are depression and anxiety, both of which are highly prevalent, both of which present atypically in adolescents, and both of which respond well to early treatment. ADHD is the next priority when academic underperformance and attentional concerns dominate the presenting picture. The PHQ-A provides a quick, validated, quantitative screen for depression severity that can be administered in the waiting room before the consultation.
DSM-5 Criteria for Major Depressive Disorder (MDD):
A diagnosis of MDD requires ALL of the following:
1. ≥5 of the following 9 symptoms present during the SAME 2-week period, representing a change from previous functioning:
- (a) Depressed mood most of the day, nearly every day (in children/adolescents: may be irritable mood)
- (b) Markedly diminished interest or pleasure in all/almost all activities (anhedonia)
- (c) Significant weight loss/gain, or decrease/increase in appetite
- (d) Insomnia or hypersomnia
- (e) Psychomotor agitation or retardation
- (f) Fatigue or loss of energy
- (g) Feelings of worthlessness or excessive/inappropriate guilt
- (h) Diminished ability to concentrate or make decisions
- (i) Recurrent thoughts of death, suicidal ideation, or a suicide attempt
2. AT LEAST ONE of the ≥5 symptoms must be either (a) depressed/irritable mood OR (b) anhedonia
3. Symptoms cause clinically significant distress or functional impairment
4. Not attributable to a substance or medical condition
5. Not better explained by a psychotic disorder
DSM-5 Criteria for Generalised Anxiety Disorder (GAD):
- Excessive anxiety and worry about multiple events or activities
- Difficulty controlling the worry
- Present for ≥6 months
- Associated with ≥3 of: restlessness/feeling keyed up, fatigue, difficulty concentrating, irritability, muscle tension, sleep disturbance (in children, only 1 symptom is required, not ≥3)
- Causes significant distress or impairment
The PHQ-A (Patient Health Questionnaire — Adolescent) is a validated 9-item self-report screening tool for adolescent depression (adapted from the PHQ-9). Each of the 9 MDD symptom domains is rated 0–3 (not at all / several days / more than half the days / nearly every day), yielding a total score of 0–27:
| PHQ-A Score | Severity | Clinical Action |
|---|---|---|
| 1–4 | Minimal | Monitor; psychoeducation |
| 5–9 | Mild | Watchful waiting; consider counselling |
| 10–14 | Moderate | Active treatment recommended (CBT ± medication) |
| 15–19 | Moderately severe | Pharmacotherapy + therapy; consider referral |
| 20–27 | Severe | Urgent psychiatric referral |
A score ≥10 on the PHQ-A is the positive screening threshold — it indicates the need for further diagnostic assessment and active treatment planning. Item 9 ('thoughts that you would be better off dead, or of hurting yourself') should be reviewed independently of the total score — any positive response to item 9 mandates a direct suicide risk assessment regardless of the total score.