Page 7 of 28
PE6.{4,7,12} | Adolescent Sexuality — SDL Guide (Part 3)
Applied Practice — The HEEADSSS Consultation Technique for Sexuality and Drugs
Integrating the sexuality (S) and drugs (D) domains into a real clinical consultation requires both knowledge and technique. The HEEADSSS framework provides the structure; the following worked example illustrates how the most sensitive domains are introduced after rapport is established through the less sensitive earlier domains.
Setting the scene: the adolescent should be seen alone for at least part of the consultation (parent may be in the room for the general health assessment but asked to wait outside for the HEEADSSS portion). The clinician introduces the process: "I see all my teenage patients on their own for part of our visit — it's completely routine. What we talk about is private unless I'm worried about your safety."
After Home, Education, Eating, Activities are covered — moving to Drugs (D):
"I ask all my patients about alcohol and other substances — not to judge, just to understand your health. Do you or your friends ever drink alcohol or smoke?" → If yes: "How often? Does it ever get in the way of school or things you want to do?" → Administer CRAFFT if disclosure occurs.
Moving to Sexuality (S):
"The next topic is relationships — I ask everyone because it's part of looking after your health. Are you dating or in a relationship? Have you been sexually active?" → If yes: "I want to make sure you're protected — are you using any contraception? Have you had any concerns about discharge, pain, or other symptoms?" → If STI risk identified: proceed to syndromic assessment and treatment.
If abuse is suspected (disclosure, or concerning behavioural/physical signs):
"I want to check — has anyone ever done anything sexual to you that you didn't want or that felt wrong?" → If abuse disclosed: remain calm, reassure the adolescent they are not at fault, explain the mandatory reporting duty clearly but sensitively: "What you've told me is very important. I'm glad you told me. The law requires me to report this to the police so you can be protected. I will be with you through this process." → Proceed to POCSO mandatory reporting within 24 hours.
Closing the consultation: summarise what was discussed, what actions are being taken, and arrange follow-up. Never let a disclosure about abuse, suicidal ideation, or high-risk substance use end without a safety plan and follow-up appointment.
Self-Assessment — Adolescent Sexuality
Test your understanding with these scenario-based questions before reviewing the answers.
Provided image
Question 1: Under the POCSO Act 2012, at what age does a child have legal capacity to consent to sexual activity? What are your reporting obligations if a 17-year-old discloses consensual sexual activity with a 20-year-old partner?
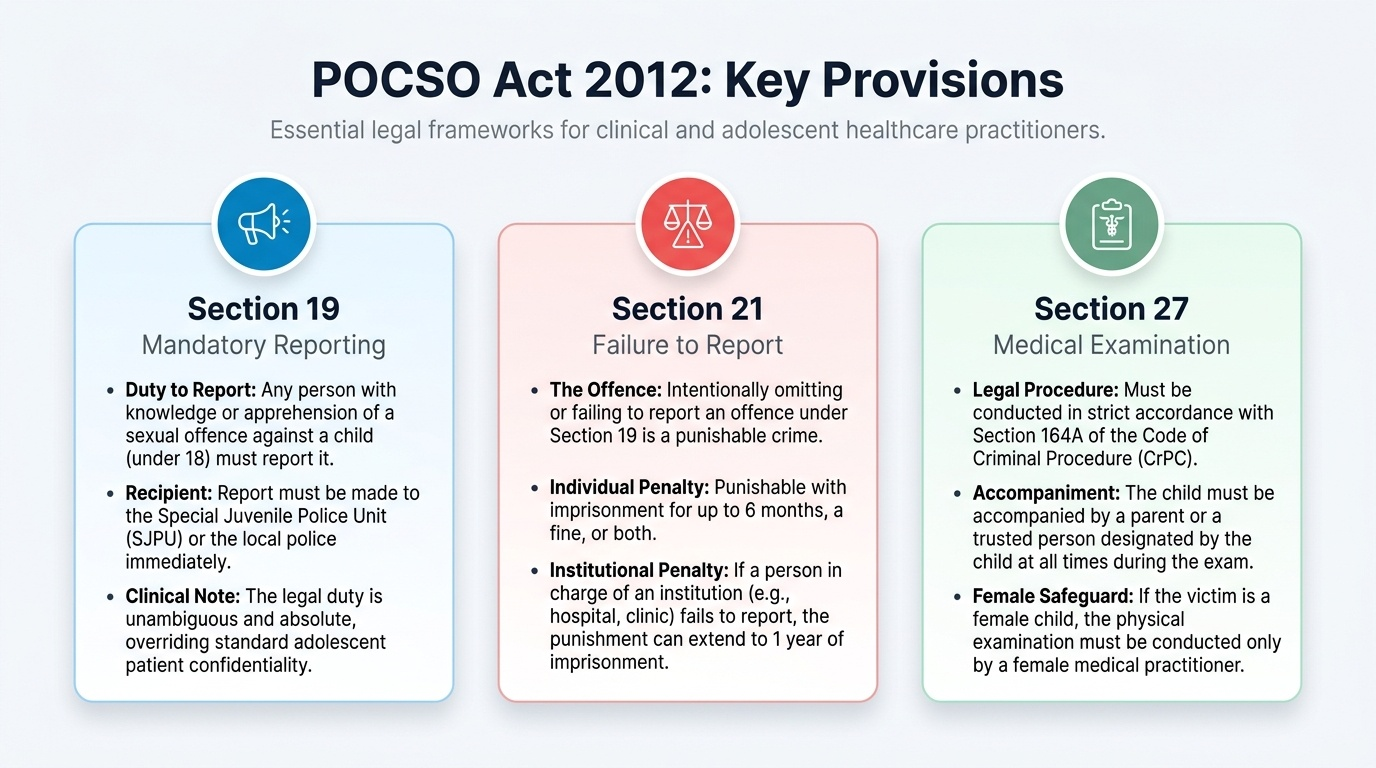
Answer: Under the POCSO Act 2012, there is NO age of sexual consent below 18 years — any sexual activity involving a person under 18 is an offence regardless of apparent consent. A 17-year-old does not have the legal capacity to consent to sexual activity. If a 17-year-old discloses sexual activity with a 20-year-old, this technically constitutes an offence under POCSO 2012, and Section 19 mandates mandatory reporting. However, in clinical practice, the clinician must weigh the adolescent's safety and trust — but the legal duty is unambiguous.
Question 2: A CRAFFT score of 3 in a 16-year-old indicates which of the following: (a) no action needed; (b) positive screen requiring brief intervention; (c) formal substance use disorder diagnosis; or (d) inpatient detoxification required?
Answer: (b) CRAFFT ≥2 = positive screen → brief motivational intervention at minimum, referral if indicated. It does not diagnose a disorder or mandate inpatient treatment.
Question 3: List three behavioural indicators that should raise clinical suspicion of sexual abuse in an adolescent.
Answer: Any three from: unexplained school absenteeism or performance decline; withdrawal or depression; age-inappropriate sexual knowledge; avoidance of a specific person; substance use as coping; running away; vague somatic complaints without organic cause; self-harm or suicidal ideation.
SELF-CHECK
Which of the following is a mandatory provision of the POCSO Act 2012?
A. A doctor must obtain the parent's written consent before reporting suspected child sexual abuse
B. Only police officers are obligated to report suspected child sexual abuse — healthcare providers are exempt
C. Any person, including a healthcare provider, who suspects sexual abuse of a person under 18 years MUST report it to the SJPU or police within 24 hours, with criminal liability for failure to report
D. Mandatory reporting applies only when the child presents with physical evidence of sexual assault
Reveal Answer
Answer: C. Any person, including a healthcare provider, who suspects sexual abuse of a person under 18 years MUST report it to the SJPU or police within 24 hours, with criminal liability for failure to report
Section 19 of the POCSO Act 2012 imposes a mandatory reporting duty on ANY PERSON — not just law enforcement — who suspects that a child (under 18 years) has been or is being sexually abused. This includes doctors, nurses, teachers, and any other person. The report must be made within 24 hours to the Special Juvenile Police Unit (SJPU) or the local police. No consent from the parent, guardian, or child is required — the duty is absolute. Section 21 creates criminal liability (up to 6 months imprisonment and/or fine) for failure to report. The absence of physical evidence does not exempt anyone from the reporting duty — suspicion based on behavioural or disclosure evidence is sufficient.