Page 12 of 25
PE10.6 | Adolescent Nutrition Problems — SDL Guide
Learning Objectives
- Explain the specific nutritional requirements of adolescents driven by the pubertal growth spurt, menarche, and cognitive demands, using ICMR-NIN 2020 reference values
- Describe the common nutritional problems of Indian adolescents: iron-deficiency anaemia, calcium deficiency, vitamin D insufficiency, and under-nutrition
- Explain the rising burden of adolescent overweight and obesity in urban India and the pathway to metabolic syndrome
- Describe the clinical features of anorexia nervosa and bulimia nervosa and their medical complications
- Outline practical screening, counselling, and programme-level approaches to adolescent nutrition including the WIFS programme
INSTRUCTIONS
Adolescence — spanning 10 to 19 years — is the second most rapid phase of growth after infancy. It is also the period during which lifelong dietary habits are formed. The nutritional decisions made during adolescence determine bone mineral density at age 30, cardiometabolic risk profile in middle age, and reproductive health in young women. India's adolescent population of approximately 253 million is nutritionally vulnerable in both directions: under-nutrition (particularly anaemia in girls) and over-nutrition (rapidly rising obesity in urban settings) affect the same generation, often in the same family.
References
- Ghai Essential Pediatrics, 9th ed, Ch 7 (Nutrition) and Ch 5 (Adolescent Health) (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Adolescent Nutrition (textbook)
- ICMR-NIN Recommended Dietary Allowances for Indians, 2020 (guideline)
- Government of India Weekly Iron and Folic Acid Supplementation (WIFS) Programme Guidelines, NHM (guideline)
- NFHS-5 (National Family Health Survey 2019-21): Adolescent Nutritional Status Data (reference)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In your school health posting, you are asked to screen 15-year-old girls in a government school. You check haemoglobin levels: 60% are below 12 g/dL. One girl, visibly thin, says she skips lunch because 'eating makes me fat.' Another is clearly overweight and brings chips and a cold drink for every break. These three problems — anaemia, an eating disorder, and obesity — exist in the same classroom, in the same age group, sometimes in the same girl. Adolescent nutrition is not one problem. It is a spectrum, and each end is dangerous.
WHY THIS MATTERS
The NFHS-5 (2019-21) found that 59.1% of adolescent girls aged 15-19 years in India are anaemic — a figure that has barely improved over the past decade. This is not a statistic without consequences: anaemic adolescent girls who become pregnant carry their anaemia into pregnancy, dramatically increasing the risk of maternal mortality, preterm birth, and low-birth-weight babies. At the other end, the prevalence of overweight among Indian adolescents has risen from 5-7% in 2000 to over 14% in urban areas by 2020. The metabolic programming that occurs during adolescent obesity — insulin resistance, dyslipidaemia, early hypertension — drives India's epidemic of type-2 diabetes and cardiovascular disease. As a clinician, you will encounter adolescent nutrition at well-child visits, school health programmes, OPD consultations for anaemia, and as a background factor in teenage pregnancies and eating disorders.
RECALL
From the Normal Nutritional Needs module, recall that adolescents have the highest absolute energy requirements of any paediatric age group — adolescent boys can require up to 2640 kcal/day and girls up to 2060 kcal/day (ICMR-NIN 2020). Recall that iron requirements rise sharply with menarche: adolescent girls need approximately 21 mg/day of iron, more than twice the 7-9 mg/day requirement of younger children, reflecting menstrual losses superimposed on the growth demand. From the Nutritional Assessment module, recall that BMI-for-age (not adult BMI) is the correct adiposity index for children and adolescents; a single BMI value does not classify nutritional status without an age-specific reference. From physiology, recall the hormonal drivers of the adolescent growth spurt: GH surge → IGF-1 → longitudinal bone growth; oestrogen/testosterone → muscle mass accretion; oestrogen → breast and pelvic development in girls; both sex hormones → accelerated bone mineralisation, making adequate calcium and vitamin D intake during adolescence critical for peak bone mass attainment.
Orientation: Why Adolescent Nutrition Is a Distinct Clinical Priority
Adolescent nutrition is clinically distinct from both childhood and adult nutrition for several intersecting reasons that are unique to this developmental stage. First, the pubertal growth spurt creates a window of dramatically increased nutrient demand — in girls, the peak height velocity of approximately 8-9 cm/year occurs around ages 11-12 years, accompanied by a 45% increase in lean body mass and a 120% increase in bone mineral accretion; in boys, the equivalent spurt at ages 13-14 years is steeper (approximately 9-10 cm/year). These biological demands create nutritional vulnerabilities that are not present in the pre-pubertal child.
Second, menarche in girls — occurring on average at 12.5 years in India — adds a monthly iron deficit of approximately 15-25 mg per menstrual period that must be compensated by dietary intake or supplementation. This is the primary driver of the extraordinarily high prevalence of iron-deficiency anaemia among Indian adolescent girls.
Third, adolescence is the final window for peak bone mass attainment. Approximately 40-60% of peak adult bone mass is accumulated during the adolescent decade; inadequate calcium and vitamin D during this period permanently reduces peak bone density, predisposing to adult osteoporosis decades later. This fact makes adolescent calcium and vitamin D intake a public health issue with long-term impact.
Fourth, adolescent eating behaviour is uniquely shaped by psychosocial factors that do not operate in young children: peer pressure, body image concerns, media influence, food advertising, and food environments (school canteens, fast-food outlets) all influence dietary choices in ways that can entrench unhealthy patterns. The formation of lifelong dietary habits during adolescence means that nutritional education and counselling in this age group has disproportionate long-term impact.
Finally, the double burden of malnutrition — co-existing under-nutrition and over-nutrition in the same population — makes adolescent nutritional assessment more complex: a BMI-based screen may identify obesity while missing concurrent micronutrient deficiencies in the same adolescent.
Normal Adolescent Nutritional Requirements and the Pubertal Growth Spurt
Adolescent nutritional requirements are the highest of any paediatric subgroup in absolute terms, and they are sex-differentiated after puberty — a distinction not relevant in pre-pubertal children. Understanding these requirements is the prerequisite for recognising dietary deficits.
Provided image
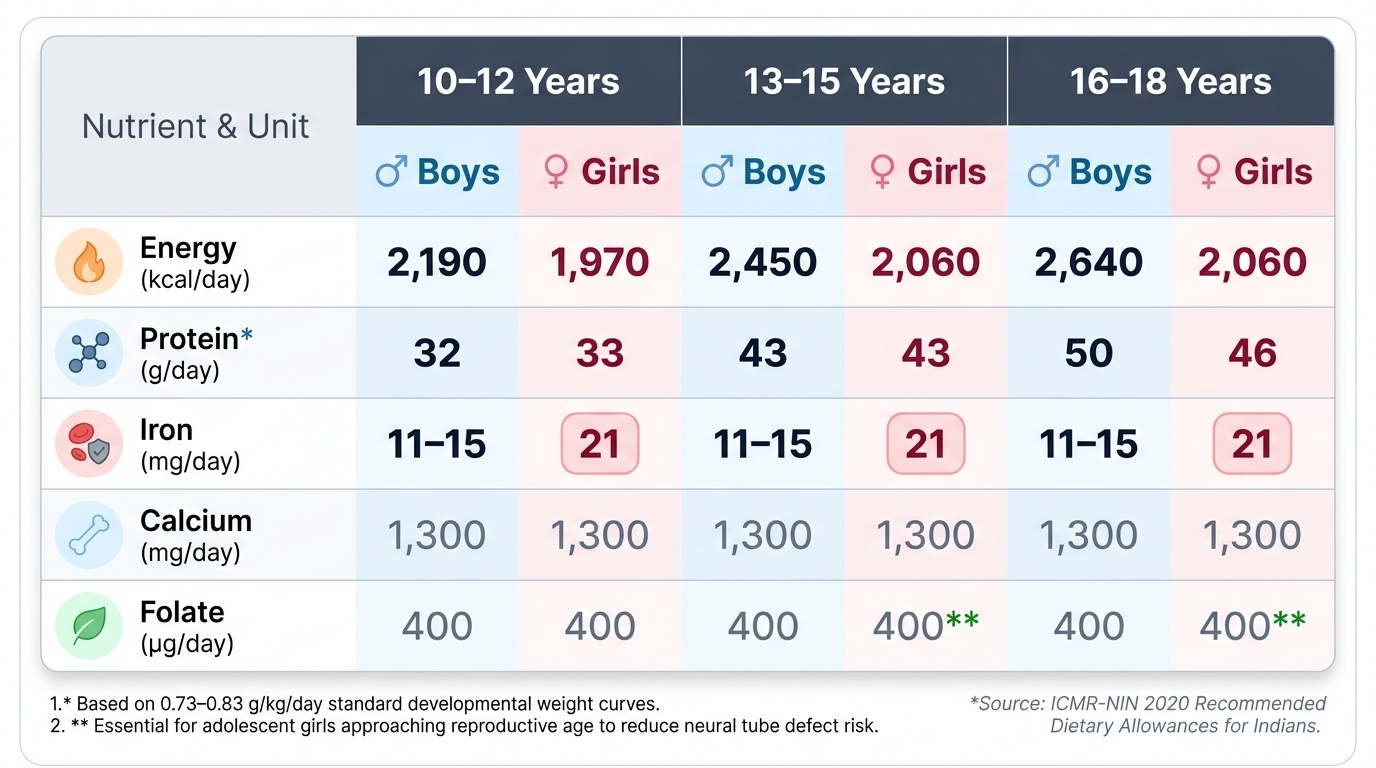
Energy requirements peak during the years of maximum growth velocity. The ICMR-NIN 2020 recommends: 10-12 years (boys) ≈ 2190 kcal/day, (girls) ≈ 1970 kcal/day; 13-15 years (boys) ≈ 2450 kcal/day, (girls) ≈ 2060 kcal/day; 16-18 years (boys) ≈ 2640 kcal/day, (girls) ≈ 2060 kcal/day. The sex difference widens after puberty because boys accumulate greater lean body mass (muscle) than girls.
Protein requirements increase in parallel with growth velocity: ICMR-NIN recommends 0.73-0.83 g/kg/day for adolescents. In practice, for a 50 kg adolescent boy, this translates to approximately 37-42 g/day. Protein quality — the amino-acid profile — remains important; adolescents on purely plant-based diets require careful food pairing to achieve adequate essential amino-acid intake.
Iron is the most clinically critical micronutrient during adolescence, particularly for girls. Boys require approximately 11-15 mg/day during the growth spurt (ICMR 2020); girls require 21 mg/day after menarche. This high requirement is difficult to meet from plant-based Indian diets alone (non-haem iron with low bioavailability ~5-10%). The result is the endemic iron-deficiency anaemia that NFHS-5 documents.
Calcium requirement peaks during the adolescent growth spurt: 1300 mg/day for ages 9-18 years (ICMR 2020), reflecting the rapid bone mineralisation of this period. Dairy products are the most bioavailable source; adolescents who avoid milk (lactose intolerance, dairy avoidance for various reasons, economic constraints) are at high risk of suboptimal peak bone mass.
Folate requirement (400 μg/day for adolescents) is of particular relevance for adolescent girls approaching reproductive age. Periconceptional folate adequacy reduces neural tube defect risk by ~70%; ensuring adequate folate intake during adolescence is a pre-conception health priority, since approximately 50% of pregnancies in India are unplanned.
Anaemia and Micronutrient Deficiencies in Adolescents
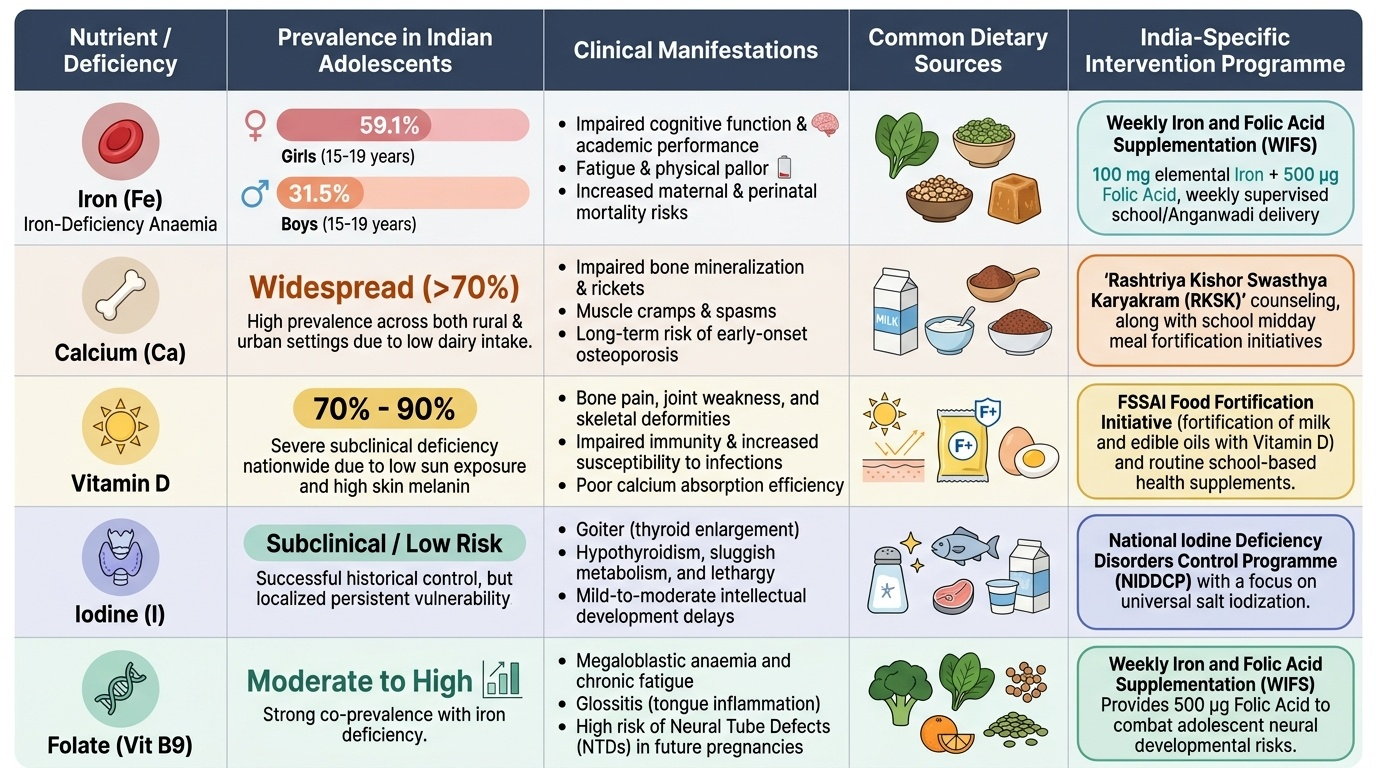
Iron-deficiency anaemia is the single most prevalent nutritional disorder among Indian adolescents, particularly girls. NFHS-5 data (2019-21) documents that 59.1% of girls aged 15-19 years and 31.5% of boys aged 15-19 years in India are anaemic (haemoglobin <12 g/dL and <13 g/dL respectively). The pathogenesis in girls involves three concurrent factors: (1) inadequate dietary iron intake (predominantly plant-based diet, low bioavailability), (2) menstrual iron losses (15-25 mg per cycle), and (3) increased haematopoietic demand during rapid growth. The clinical consequences extend beyond pallor and fatigue — iron-deficiency anaemia impairs cognitive function, reduces academic performance, reduces work capacity, and — when carried into pregnancy — dramatically increases maternal and perinatal mortality.
Provided image
The WHO anaemia thresholds for adolescents are: haemoglobin <12 g/dL for girls aged 12-18 years; <13 g/dL for boys ≥14 years. Severity grading: mild = 10-11.9 g/dL, moderate = 7-9.9 g/dL, severe = <7 g/dL.
India's Weekly Iron and Folic Acid Supplementation (WIFS) programme is the primary national intervention for adolescent anaemia. Under this NHM scheme, all adolescents (both in school and out-of-school) receive a weekly supervised dose of 100 mg elemental iron + 500 μg folic acid, delivered through schools and Anganwadi Centres on a fixed weekly day. Studies show WIFS reduces the prevalence of anaemia by 25-35% when coverage and compliance are adequate. Counsellors must reinforce weekly, not daily, dosing — weekly IFA is as effective as daily but with significantly better gastrointestinal tolerability and higher compliance.
Calcium deficiency is widespread among Indian adolescents due to the low dairy intake in many households. The consequence is suboptimal peak bone mass — a deficit that is permanent and predisposes to osteoporosis and fragility fractures in later life. India does not have a national calcium supplementation programme for adolescents; dietary counselling (milk, curd, fortified foods, ragi/finger millet which is naturally calcium-rich at ~344 mg/100g) is the primary approach.
Vitamin D insufficiency (serum 25-OH vitamin D <20 ng/mL) is almost universal in Indian adolescents despite India's tropical latitude, because of indoor schooling, dark clothing, and reduced outdoor play time in urban areas. Vitamin D is required for intestinal calcium absorption; vitamin D deficiency therefore compounds the calcium deficit.
Iodine deficiency in adolescents causes goitre, hypothyroidism, and subtle cognitive impairment. Universal iodised salt remains the primary prevention strategy.
Folate deficiency — from low consumption of green leafy vegetables and legumes — is particularly concerning in adolescent girls, given its periconceptional significance.
SELF-CHECK
Under the Government of India's WIFS programme, what is the correct dose and frequency of iron-folic acid supplementation for adolescent girls?
A. 30 mg elemental iron + 250 μg folic acid daily
B. 100 mg elemental iron + 500 μg folic acid weekly
C. 200 mg elemental iron + 5 mg folic acid daily
D. 60 mg elemental iron + 500 μg folic acid every 2 weeks
Reveal Answer
Answer: B. 100 mg elemental iron + 500 μg folic acid weekly
The WIFS programme prescribes 100 mg elemental iron + 500 μg folic acid once weekly for all adolescents. Weekly dosing is as effective as daily dosing for iron replenishment but has significantly better gastrointestinal tolerability and compliance, particularly in school-based programmes where supervised administration is feasible. Daily iron (60 mg) is used for treatment of established anaemia in pregnancy, not for adolescent supplementation under WIFS. The higher daily dose (200 mg) in option C would cause significant gastrointestinal side effects.