Page 19 of 25
PE11.3-4 | Childhood Obesity Assessment — SDL Guide (Part 2)
Physical Examination: BMI, Waist-Hip Ratio, and External Markers
The physical examination of an obese child must be systematic and complete, covering anthropometric measurements, vital signs, and a structured head-to-toe clinical assessment. A common error is to record only the weight and BMI and stop there — this misses the blood pressure, the waist circumference, and the cutaneous markers that carry the most immediate clinical significance. Perform measurements first, before the clinical examination, because the anthropometric data contextualises everything you will observe clinically. Privacy and dignity must be preserved throughout: expose only the body part being examined, use a chaperone for adolescent girls, position the patient comfortably, and avoid any language — verbal or non-verbal — that stigmatises body weight. Obese children are already likely to have experienced weight-based stigma; the clinical encounter must be a safe, non-judgemental space if you are to establish the therapeutic relationship needed for effective counselling.
Anthropometric measurements (perform in this sequence):
1. Weight (light clothing, calibrated scale, nearest 0.1 kg)
2. Height (barefoot, stadiometer, Frankfurt plane, nearest 0.1 cm)
3. Calculate BMI = weight ÷ height² and plot on IAP age/sex chart → record percentile
4. Waist circumference (mid-axillary line, midpoint 12th rib–iliac crest, gentle expiration, nearest 0.1 cm)
5. Hip circumference (widest buttock point, horizontal tape, nearest 0.1 cm)
6. Waist-hip ratio = waist ÷ hip; waist-to-height ratio = waist ÷ height
7. Blood pressure (age-appropriate cuff, after 5 min seated rest, both arms if first reading elevated)
Head and neck:
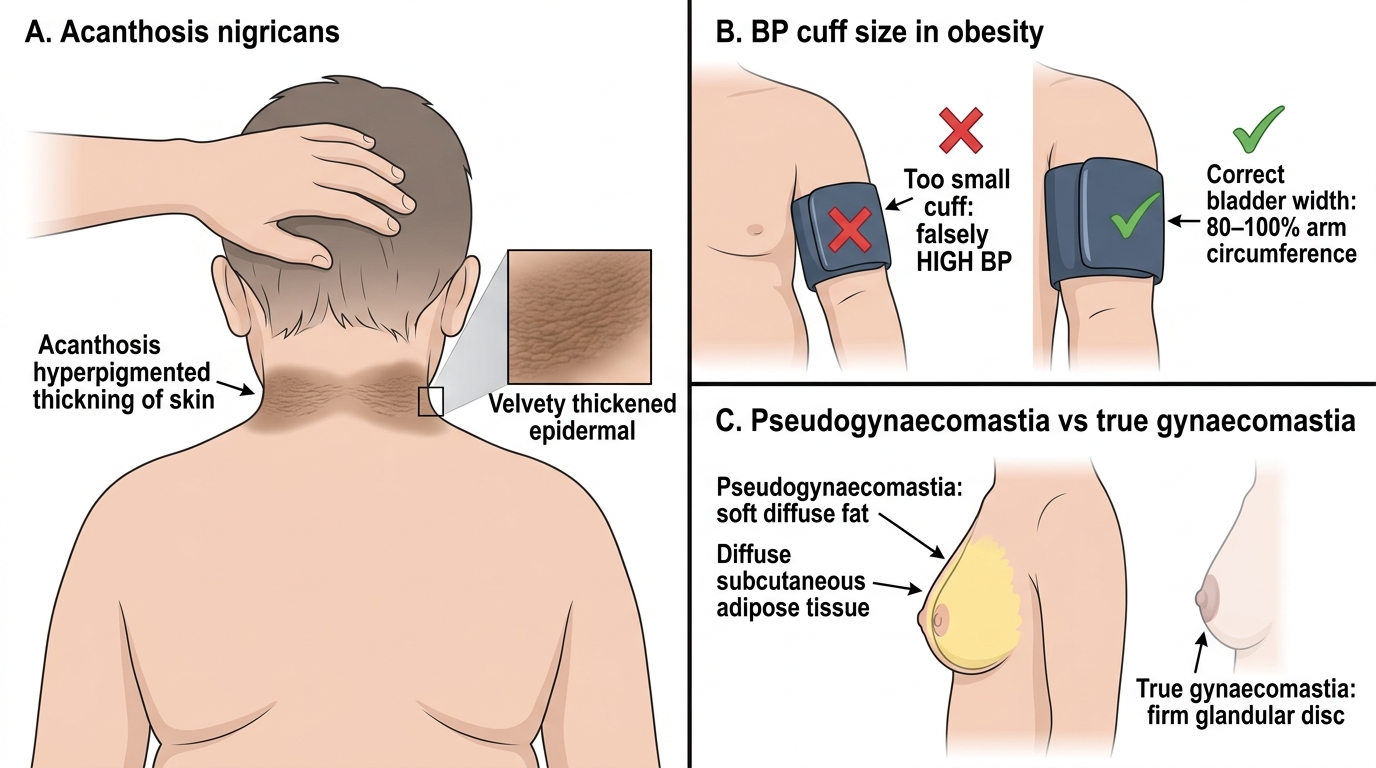
- Inspect neck for acanthosis nigricans: look at the nape (posterior neck crease), then axillae and groin. Grade severity: mild (barely visible), moderate (clearly visible brown velvety thickening), severe (warty, papillomatous). Document location and grade. Always examine the axillae and groin even if the neck is clear.
- Note round facies and moon face — the latter with central adiposity and hypertension raises Cushing syndrome
- Examine thyroid for goitre (hypothyroidism)
Skin:
- Striae distensae: inspect thighs, lower abdomen, upper arms, and breasts. In primary obesity, striae are typically silver-white to pale pink. Purple/violaceous striae suggest Cushing syndrome (due to elevated cortisol causing collagen fragility) and are a red flag for further investigation.
- Pseudogynaecomastia: in obese boys, palpate the breast tissue. Pseudogynaecomastia is soft, diffuse, and moves freely with the overlying skin — it is adipose tissue, not glandular. True gynaecomastia has a firm, palpable, sometimes tender disc of glandular tissue under the nipple-areolar complex. The distinction is important because true gynaecomastia implies hormonal imbalance (elevated oestrogens, reduced androgens — as in obesity-related aromatase excess, or secondary to medications).
- For adolescent girls: signs of PCOS — hirsutism (terminal hair on chin, upper lip, sideburns, linea alba), acne, and acanthosis nigricans together constitute a strong clinical triad.
Abdomen: hepatomegaly (NAFLD), tenderness.
Musculoskeletal: gait, knee alignment (genu varum in Blount's disease), hip range of motion (limited internal rotation + hip pain = SCFE until proven otherwise).
Respiratory and cardiovascular: auscultation for signs of cardiomegaly; look for signs of pulmonary hypertension in severe obesity.
Signs suggesting secondary causes:
- Short stature + obesity → thyroid/GH/Cushing
- Dysmorphic features + hypotonia → Prader-Willi
- Retinal dystrophy + polydactyly + obesity → Bardet-Biedl
- Purple striae + central distribution + hypertension → Cushing
Clinical Signs and Examination Pearls in Childhood Obesity
CLINICAL PEARL
The blood pressure cuff size is a non-negotiable technical detail that determines diagnostic accuracy. In obese children the upper arm circumference is substantially larger than average. Using a standard paediatric cuff (designed for normal-weight children) on a large arm will give a falsely HIGH blood pressure reading — leading to over-diagnosis of hypertension, unnecessary investigation, and parental anxiety. The correct cuff bladder should cover 80–100% of the arm circumference. Many paediatric clinics do not stock large-adult cuffs, so check and use the appropriate size before recording the blood pressure. If in doubt, use the next larger cuff — a cuff that is slightly too large gives a small underestimate, which is far less clinically harmful than the large overestimate from a small cuff.
SELF-CHECK
On examining a 13-year-old obese boy, you notice breast enlargement. On palpation you feel a soft, diffuse fatty mass that moves freely with the overlying skin, with no firm disc of tissue under the nipple. What is the MOST likely finding and what does it indicate?
A. True gynaecomastia due to hormonal imbalance requiring endocrine evaluation
B. Pseudogynaecomastia due to adipose deposition — a normal finding in obesity
C. Lipoma of the breast requiring biopsy
D. Breast abscess requiring antibiotic therapy
Reveal Answer
Answer: B. Pseudogynaecomastia due to adipose deposition — a normal finding in obesity
The description — soft, diffuse, freely mobile fatty mass without a firm sub-areolar glandular disc — is pseudogynaecomastia, which is adipose tissue deposition in the breast region and is a common and expected finding in obese boys. It does not indicate hormonal imbalance. True gynaecomastia, by contrast, has a firm, sometimes tender, disc of glandular tissue palpable directly beneath the nipple-areolar complex; it implies elevated oestrogen or reduced androgen activity and warrants endocrine evaluation. Distinguishing these two by palpation is an essential clinical skill.
Interpretation of Findings and Documentation
After completing the history and examination, the clinician must synthesise the findings into a structured clinical assessment that drives the next steps. A disorganised list of raw measurements is not a clinical assessment — interpretation and risk stratification are required. The key interpretive steps are as follows.
Provided image
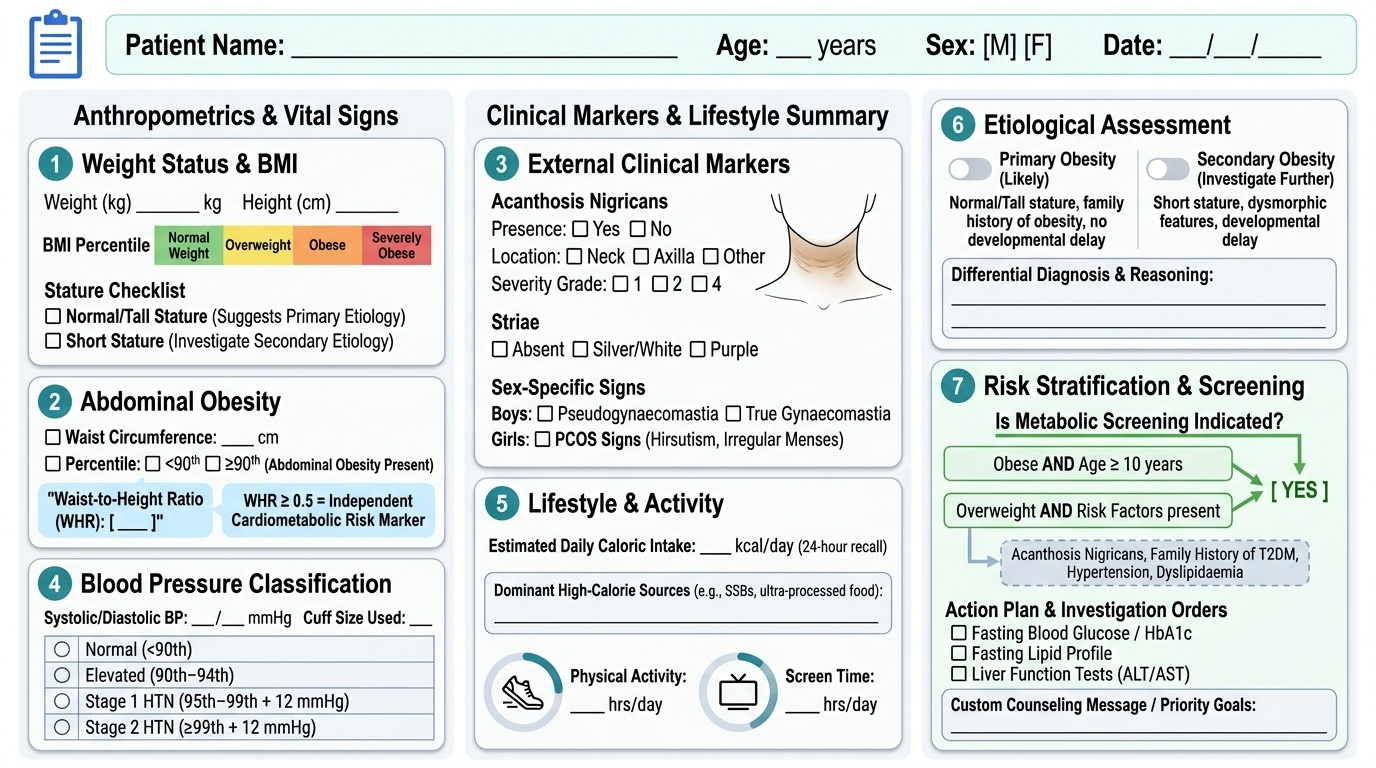
Step 1: Classify weight status. Plot the calculated BMI on the IAP age- and sex-specific growth chart. Document the percentile and the classification: normal weight (<85th), overweight (≥85th and <95th), obese (≥95th), or severely obese (≥99th). If the child is obese, note whether stature is normal or tall (suggesting primary) or short (suggesting secondary).
Step 2: Assess abdominal obesity. Plot waist circumference on the age/sex-specific waist circumference reference chart (IAP). Document whether it is >90th percentile (abdominal obesity present). Calculate waist-to-height ratio: >0.5 is an independent cardiometabolic risk marker applicable across ethnicities.
Step 3: Document external markers. Record presence/absence and severity of acanthosis nigricans (location, grade), striae (colour — silver/white vs purple), pseudogynaecomastia vs true gynaecomastia in boys, PCOS signs in girls.
Step 4: Blood pressure classification. Classify blood pressure using age/sex/height-specific paediatric percentile tables: normal (<90th), elevated (90th–94th), stage 1 hypertension (95th–99th +12 mmHg), stage 2 hypertension (>99th +12 mmHg). Note the cuff size used.
Step 5: Dietary and activity summary. Document the total estimated caloric intake from the 24-hour recall, identify the dominant high-calorie sources, and record hours of physical activity and screen time per day. This directs the counselling message.
Step 6: Aetiological assessment. Based on all findings, classify as primary (likely) or secondary (investigate further) and document the reasoning. If secondary features are present, list the differential and the investigation plan.
Step 7: Risk stratification and plan. Document whether metabolic screening is indicated (yes, if obese ≥10 years, or overweight with risk factors: acanthosis nigricans, family history T2DM, hypertension, dyslipidaemia). List the recommended investigations.
Applied and Supervised Practice
The following worked example simulates an OSCE-type clinical encounter. Read through the vignette, then verify that you would arrive at the same structured assessment. When you encounter a real obese child in clinic under supervision, use the same systematic framework.
Vignette: Priya is a 13-year-old girl brought by her mother for a school-health referral. The referral note says 'BMI above normal'. Her weight is 72 kg, height 158 cm. She watches 5 hours of screens daily, walks 5 minutes to the school bus, and does no structured exercise. Her 24-hour recall shows three cups of sweetened packaged juice, two packs of chips, and meals totalling approximately 3,200 kcal. She has irregular periods for the past 8 months, mild acne on the chin, and some facial hair. Previous growth chart shows a steady upward BMI trajectory from the 75th percentile at age 8 to today.
Worked assessment:
Anthropometry: BMI = 72 ÷ (1.58)² = 72 ÷ 2.4964 = 28.8 kg/m². Plot on IAP 13-year girls chart → this corresponds to approximately the 98th percentile → classification: obese. Stature: 158 cm for a 13-year-old girl is approximately at the 60th height percentile — she is NOT short, so primary obesity is more likely.
Waist circumference: measured at 95 cm → exceeds 90th percentile for a 13-year-old girl (approximately 80 cm) → abdominal obesity present. Waist-to-height ratio = 95 ÷ 158 = 0.60 (>0.5 = elevated cardiometabolic risk).
Blood pressure: 126/82 mmHg using a large-adult cuff → classify using age/sex/height percentile tables (at 60th height percentile for age 13 girls) → 90th percentile BP is approximately 119/76 → this reading exceeds the 90th percentile → classify as elevated blood pressure (pre-hypertension), re-check in 1 month.
External markers: On inspection of the neck — acanthosis nigricans present, moderate grade, at nape and both axillae. No purple striae (silver striae on thighs bilaterally). No goitre. Facial hair on chin and upper lip. Irregular periods + acne + hirsutism + acanthosis nigricans → PCOS screen indicated.
Dietary summary: estimated intake ~3,200 kcal/day (estimated requirement ~1,800–2,000 kcal/day for her age/sex); excess ~1,200 kcal/day; principal sources: sweetened beverages, chips, large meal portions.
Physical activity: 0 min structured exercise; >5 h screen time/day (recommended <2 h). Physical inactivity is a co-contributor.
Assessment and plan: Primary obesity (obese, normal stature, gradual trajectory), acanthosis nigricans (insulin resistance), possible PCOS. Investigations: fasting lipid profile, fasting glucose + 2-h OGTT, HbA1c, LFTs (NAFLD screen), TSH, LH, FSH, testosterone, pelvic USG. Management: family-based lifestyle modification (dietary reduction of sugar-sweetened beverages as first priority; target ≥60 min MVPA/day; screen time <2 h/day). Re-assess in 3 months.
SELF-CHECK
A 13-year-old obese girl has a waist circumference of 92 cm and a height of 155 cm. What is her waist-to-height ratio, and does it indicate elevated cardiometabolic risk?
A. 0.49 — below the risk threshold of 0.5, no increased risk
B. 0.59 — above the risk threshold of 0.5, elevated cardiometabolic risk
C. 0.92 — above the risk threshold of 0.5, elevated cardiometabolic risk
D. Cannot be determined without the hip circumference
Reveal Answer
Answer: B. 0.59 — above the risk threshold of 0.5, elevated cardiometabolic risk
Waist-to-height ratio = waist circumference ÷ height = 92 ÷ 155 = 0.593. This exceeds the threshold of 0.5, indicating elevated cardiometabolic risk. The waist-to-height ratio is calculated from waist circumference and height alone — the hip circumference is not needed (that is used for the waist-hip ratio, which is a different measure). A waist-to-height ratio >0.5 is a validated, ethnicity-independent paediatric cardiometabolic risk marker that captures central adiposity independent of absolute BMI.
Self-Assessment
Use these questions to verify that you have mastered the core procedural skills covered in this module. These represent the type of structured assessment questions you will encounter in OSCE examinations and in clinical supervisor sign-offs. Work through each question carefully before checking the answer, focusing not just on whether your answer is correct but on whether your reasoning process — the sequence of steps, the measurements, the landmarks — would withstand direct observation by a clinical examiner.
Q1. A 10-year-old boy weighs 48 kg and is 138 cm tall. Calculate his BMI. Given that his age-specific 85th percentile BMI is 19.5 kg/m² and 95th percentile is 22.0 kg/m², classify his weight status.
Answer: BMI = 48 ÷ (1.38)² = 48 ÷ 1.9044 = 25.2 kg/m². Since 25.2 > 22.0 (95th percentile threshold), he is classified as obese. Note: do not use the adult cut-off of 25 for 'overweight' — apply the paediatric percentile thresholds from the IAP chart.
Q2. List the five measurements you must perform when assessing an obese child for abdominal adiposity and cardiometabolic risk, stating the correct anatomical landmarks for each.
Answer: (1) Weight — calibrated scale, light clothing, nearest 0.1 kg; (2) Height — stadiometer, barefoot, Frankfurt plane, nearest 0.1 cm; (3) Waist circumference — midpoint between inferior 12th rib and iliac crest, mid-axillary line, gentle expiration; (4) Hip circumference — widest point of buttocks at level of greater trochanters; (5) Blood pressure — age-appropriate cuff (bladder width 40% of arm circumference), after 5 min seated rest. Derived indices: BMI from weight+height, WHR from waist+hip, waist-to-height ratio from waist+height.
Q3. You examine an obese 12-year-old boy and find velvety, dark thickening in both axillae and at the back of the neck. What is this sign called, what does it indicate, and what investigation should follow?
Answer: This is acanthosis nigricans, a cutaneous marker of insulin resistance caused by hyperinsulinaemia driving epidermal and dermal proliferation via IGF-1 receptors. It indicates that this child has significant insulin resistance and is at elevated risk for type 2 diabetes and metabolic syndrome. Investigations that should follow: fasting glucose and 2-hour OGTT, HbA1c, fasting lipid profile, and liver function tests (to screen for NAFLD). Refer to an endocrinologist or paediatric metabolic team if glucose intolerance is confirmed.