Page 2 of 25
PE9.{1,3} | Normal Nutritional Needs — SDL Guide (Part 2)
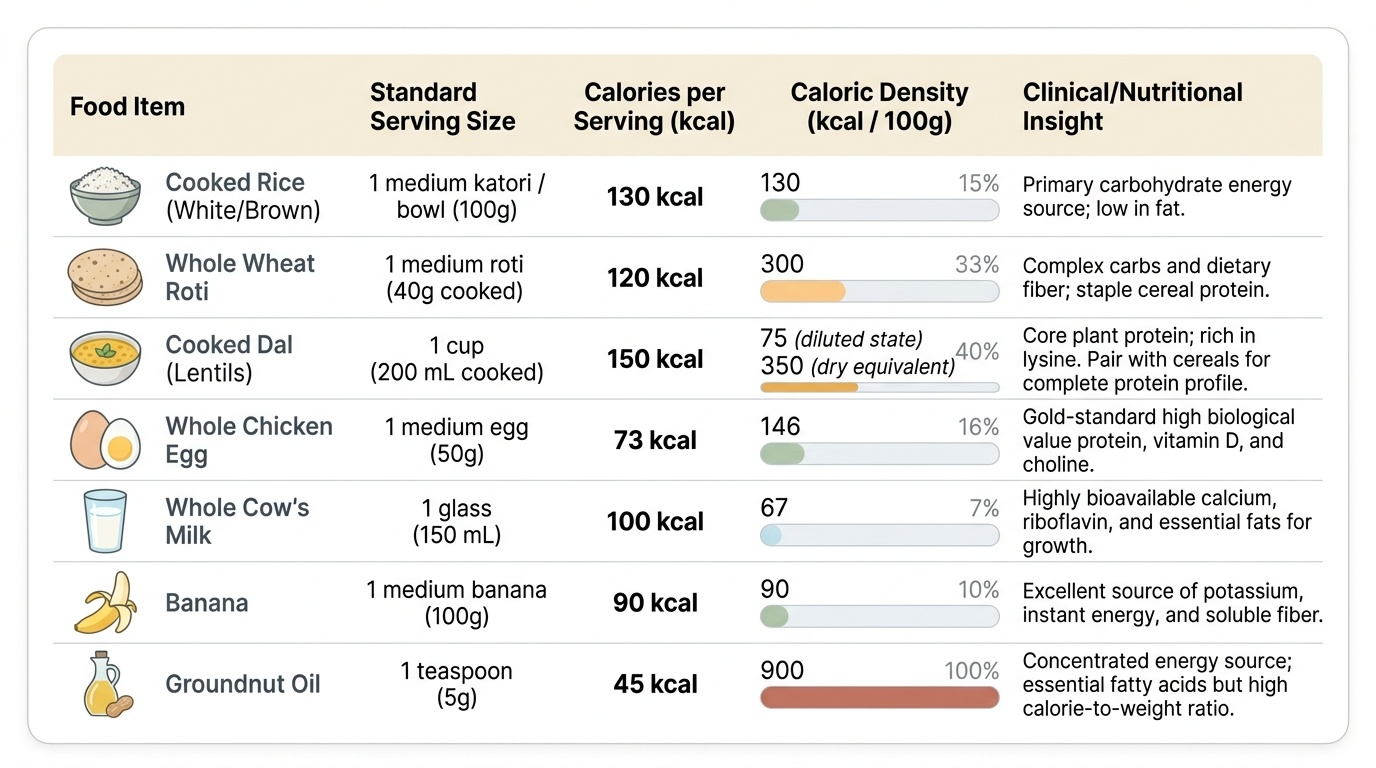
Caloric Value of Common Indian Foods
Nutritional counselling in the Indian context is only effective when expressed in terms of locally available, affordable foods. Prescribing 'high-protein foods' without naming them in the patient's dietary vocabulary has little practical impact. The ICMR-NIN publishes caloric and nutrient composition data for Indian foods (Nutritive Value of Indian Foods, revised regularly); familiarity with this data is part of the clinical toolkit.
Provided image
Cereals are the caloric backbone of most Indian meals. Cooked rice provides approximately 130-145 kcal per 100 g (raw rice ≈ 345-360 kcal/100g, which yields about 3× its weight when cooked with water). A single medium roti (40 g) from whole wheat provides approximately 120-130 kcal. Cereals are predominantly carbohydrate-rich but contribute a significant portion of daily protein intake when consumed in large quantities, albeit of moderate biological value.
Pulses and legumes (dal, chana, rajma, lentils) are the primary protein source in vegetarian Indian households. Dry lentils or dal provide approximately 340-360 kcal/100g with 20-26 g protein/100g dry weight. When cooked, the caloric density falls substantially: a standard serving of dal (200 mL cooked) provides approximately 150-180 kcal and 10-12 g protein. The combination of a cereal and a pulse — 'dal-chawal' or 'roti-dal' — provides a nearly complete amino-acid profile.
Dairy is a calorie and calcium-dense food. Whole cow's milk provides approximately 65-70 kcal/100 mL with 3.3 g protein. Buffalo milk is richer: ≈ 100-117 kcal/100 mL. Curd (dahi) from whole milk ≈ 60-65 kcal/100 g. These foods are major sources of high-quality protein, calcium, and riboflavin. For young children, dairy should not be replaced with low-fat versions before 2 years of age, as fat is essential for brain myelination in this period.
Eggs are among the most nutrient-dense foods available: one whole egg (50 g) provides approximately 73 kcal, 6 g protein, and 5 g fat, along with vitamins D, B12, and choline. In India, the ICDS midday-meal programme provides eggs in some states as the single most cost-effective intervention for child protein-energy nutrition.
Fats and oils are calorically concentrated at 900 kcal/100 g; a teaspoon of any cooking oil (5 g) contributes 45 kcal. While not usually a limiting factor in Indian diets, the type of fat matters: groundnut, mustard, and sesame oils are commonly used and provide monounsaturated and polyunsaturated fatty acids; coconut oil is saturated-fat-rich. Refined vanaspati or partially hydrogenated oils contain trans-fatty acids and should be avoided in children's diets.
Fruits and vegetables are relatively low in caloric density (50-100 kcal/100g) but provide essential micronutrients, dietary fibre, and phytochemicals. Banana is calorie-denser than most fruits (≈ 90-100 kcal per medium fruit); green leafy vegetables (spinach, methi) are iron-, folate-, and carotene-rich despite low caloric density — valuable micronutrient vehicles.
CLINICAL PEARL
In practice, the simplest way to estimate whether an Indian child's diet is adequate is the 'handful rule' for toddlers: each meal should contain one small handful of cereal + half a handful of pulses + a thumb-size portion of fat (oil/ghee/milk) + vegetables. The energy density of cereal-pulse mixtures is approximately 100-120 kcal per 100g when freshly cooked, but drops to 70-80 kcal/100g when diluted with water to soft porridge consistency — a common error in complementary feeding where over-diluted foods fail to meet energy requirements despite adequate volume. When counselling families, explicitly advise against excessive dilution of weaning foods. Similarly, iron absorption from plant sources (non-haem iron) is 5-10× lower than from animal sources; advising concurrent vitamin C (lemon juice on dal, amla) can increase non-haem iron absorption by 2-4-fold — a simple, cost-free improvement for vegetarian families.
Breastfeeding, Complementary Feeding, and Feeding Transitions
Human breast milk is the ideal nutritional and immunological food for infants in the first 6 months of life. Its composition is dynamic: colostrum (secreted in the first 3-5 days) is lower in fat and calories but rich in secretory immunoglobulin A (sIgA), lactoferrin, leukocytes, growth factors, and zinc — precisely the components that protect a neonate whose gut is colonising and whose immune system is immature. Transitional milk (days 5-14) and then mature breast milk (after 2 weeks) provide approximately 65-70 kcal/100 mL, 1.0-1.1 g protein/100 mL, and 3.5-4.5 g fat/100 mL, with lactose as the dominant carbohydrate.
WHO and IAP both recommend exclusive breastfeeding for the first 6 months of life, meaning no water, juice, or supplementary foods. Beyond 6 months, continued breastfeeding is recommended alongside complementary foods until at least 2 years of age. This recommendation is evidence-based: exclusive breastfeeding reduces all-cause infant mortality, protects against diarrhoea and pneumonia, promotes neurodevelopment, and reduces later risk of obesity and type-2 diabetes.
Complementary foods should be introduced at exactly 6 months — not before (immature gut and immune system increase infection risk) and not after (nutrient needs, especially for energy and iron, can no longer be met by breast milk alone). The first complementary foods should be semi-solid, energy-dense, iron-rich, and prepared with good hygiene. Key principles: (1) start with single-ingredient soft foods (well-cooked mashed rice, vegetable purée); (2) increase texture progressively as the child's motor skills develop (lumpy at 9 months, family foods by 12 months); (3) achieve 5-6 meals per day by 12 months in a breastfed infant; (4) include protein sources (dal, egg, meat) by 8-9 months.
The transition to family foods by 12-18 months is guided by the child's developmental readiness — pincer grasp, chewing movements, eruption of first molars (typically 12-16 months). By 2 years, most children should be eating three balanced family meals with two nutritious snacks, and breastfeeding can be gently phased out, though the WHO recommends continuation beyond 2 years if the mother and child desire it.
Some important feeding practices to counsel against: offering bottle feeding as a substitute for breastfeeding (increases infection risk, promotes dental caries), giving cow's milk as the main drink before 12 months (low iron content, high renal solute load), and introducing ultra-processed snacks (high sugar/salt, low micronutrient density) before 2 years. These behaviours are common in urban India and represent modifiable risk factors for malnutrition and later obesity.
SELF-CHECK
A 7-month-old exclusively breastfed infant is being started on complementary foods. Which of the following is MOST important to include as an early priority?
A. High-sugar fruit juices to increase caloric density
B. Iron-rich foods such as mashed dal or minced meat
C. Cow's milk as the main liquid feed
D. Highly spiced family foods to develop taste preferences
Reveal Answer
Answer: B. Iron-rich foods such as mashed dal or minced meat
Iron is the nutrient most likely to become limiting after 6 months of age, because fetal iron stores are depleted by 4-6 months and breast milk provides insufficient iron to meet the rapidly growing infant's needs. Iron-rich first foods (legumes, organ meats, iron-fortified cereals) are therefore a high priority. Fruit juices add sugar without adequate nutrient density and displace more nutritious foods. Cow's milk as main liquid before 12 months provides low bioavailable iron and an excessive renal solute load. Heavily spiced foods are inappropriate for immature gut and taste preferences at this age.
Clinical Significance: Consequences of Nutritional Adequacy vs Deficiency
Understanding normal requirements allows the clinician to predict and recognise the clinical consequences of their absence. The paediatric deficiency syndromes are among the most clinically distinctive presentations in medicine, and their early recognition can be life-saving or growth-saving.
Energy-protein deficiency on a background of adequate micronutrients presents as the wasted and/or stunted child: weight-for-height reduced (wasting = acute deficiency), height-for-age reduced (stunting = chronic deficiency). Severe energy-protein deficiency produces Severe Acute Malnutrition (SAM) — characterised by weight-for-height <−3 SD, MUAC <11.5 cm (in 6-59 month children), or bilateral pedal oedema (kwashiorkor pattern) — which carries a mortality risk of 20-30% without treatment. This is covered in detail in the SAM module (PE10).
Iron-deficiency anaemia is the world's most common nutritional deficiency. In young children it presents as pallor, irritability, reduced activity, anorexia, and — critically — impaired cognitive development and neurodevelopment (iron is required for myelination and neurotransmitter synthesis). The cognitive effects are partially irreversible even with late iron supplementation, emphasising the importance of prevention.
Vitamin A deficiency presents in a stepwise manner: earliest is night blindness (nyctalopia), then Bitot's spots (white foamy plaques on the bulbar conjunctiva — pathognomonic), then xerophthalmia (corneal dryness, keratomalacia, and ultimately corneal perforation with permanent blindness). Vitamin A deficiency also increases susceptibility to and severity of measles and diarrhoeal diseases.
Rickets from vitamin D deficiency is clinical in the infant and toddler: craniotabes (ping-pong-ball skull softening), rachitic rosary (costochondral junction swelling), Harrison's sulcus (rib cage indentation from diaphragm pull), frontal bossing, and the classic bow-legs (genu varum) of the walking toddler. Vitamin D deficiency in older children causes osteomalacia (generalised bone pain) rather than classic rickets.
Iodine deficiency during pregnancy and early infancy causes cretinism — irreversible intellectual disability, deafness, neuromotor impairment, and short stature. In school-age children, moderate iodine deficiency reduces IQ by an estimated 10-15 points, a population-level cognitive cost that is fully preventable by universal iodised salt.
Zinc deficiency classically presents as growth failure, delayed sexual maturation, poor wound healing, acrodermatitis enteropathica (perioral and acral rash), and impaired immunity with recurrent infections. Zinc supplementation (10-20 mg/day for 10-14 days) is a WHO/UNICEF-recommended adjunct to ORS in children with acute diarrhoea.
Conversely, the emergence of over-nutrition — excessive caloric intake leading to childhood obesity — now represents the other end of the spectrum in urban India. Obesity in childhood is associated with metabolic syndrome, type-2 diabetes, polycystic ovarian syndrome, and orthopedic complications. The same framework of energy requirements must be applied to identify excessive caloric intake, not merely deficiency.
Self-Assessment
Review your understanding of the key factual anchors from this module before moving to nutritional assessment and therapeutic feeding. These figures form the quantitative basis for every dietary prescription you will write in clinical practice and for every dietary gap you will identify during a nutritional history. Clinicians who cannot recall the reference values cannot recognise when a child's intake is inadequate. Can you recall: (1) the WHO energy requirement per kg for infants 0-6 months? (2) the ICMR-NIN 2020 daily energy requirement for a 5-year-old child? (3) the iron requirement at 6-12 months and why it is higher than in the first 6 months? (4) the caloric value per 100g of rice, dal, and egg? (5) the duration of recommended exclusive breastfeeding? (6) the key clinical signs of vitamin A, vitamin D, and iron deficiency?
These figures are not arbitrary — they define the boundary between adequacy and deficiency, and they are the quantitative basis for every dietary prescription you will write.