Page 5 of 25
PE9.{2,4-7} | Nutritional Assessment Workflow — SDL Guide (Part 2)
Caloric Gap Calculation and Classification
Once dietary intake is estimated from the 24-hour recall and anthropometric measurements are available, the clinician can calculate the caloric gap and classify nutritional status. This two-step process is the analytical core of nutritional assessment.
Provided image
Step 1 — Calculate expected caloric requirement. Use either (a) the ICMR-NIN 2020 age-group RDA values or (b) the Holliday-Segar formula for maintenance caloric needs: 100 kcal/kg/day for the first 10 kg of body weight, plus 50 kcal/kg/day for the next 10 kg (10-20 kg), plus 20 kcal/kg/day for each kilogram above 20 kg. For example, a 12 kg child requires (100 × 10) + (50 × 2) = 1100 kcal/day. In disease states (fever, infection, malnutrition recovery), add a stress factor: 10-30% extra above maintenance.
Step 2 — Estimate actual intake. Sum the caloric content of all food and beverages consumed in the 24-hour recall using standard food composition values. The gap = expected requirement − actual intake.
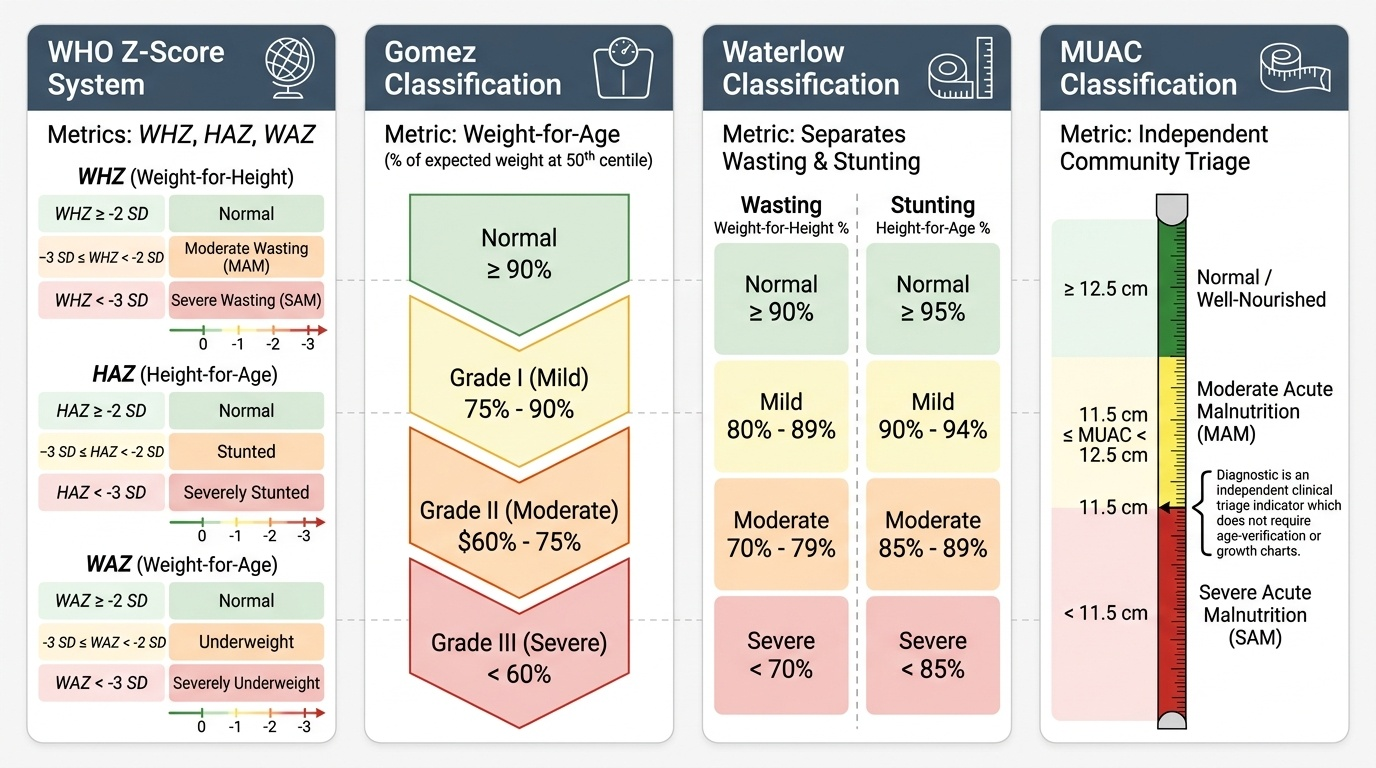
Step 3 — Classify nutritional status. Multiple systems are in use, each serving a different purpose:
The WHO z-score system is the international standard, using three indices:
• Weight-for-height (WHZ): measures wasting (acute malnutrition). WHZ < −2 SD = moderate wasting (MAM); WHZ < −3 SD = severe wasting (SAM).
• Height-for-age (HAZ): measures stunting (chronic malnutrition). HAZ < −2 SD = stunted; < −3 SD = severely stunted.
• Weight-for-age (WAZ): measures underweight (mixed/composite). WAZ < −2 SD = underweight; < −3 SD = severely underweight.
The Gomez classification uses weight-for-age as a percentage of the expected weight at the 50th centile for age:
• Grade I (mild): 75-90% of expected weight
• Grade II (moderate): 60-75% of expected weight
• Grade III (severe): <60% of expected weight
The Waterlow classification separately grades wasting and stunting:
• Wasting: weight as percentage of expected weight-for-height (normal ≥90%, mild 80-89%, moderate 70-79%, severe <70%)
• Stunting: height as percentage of expected height-for-age (normal ≥95%, mild 90-94%, moderate 85-89%, severe <85%)
MUAC classification provides an independent, rapid severity classification (see Anthropometry section) without requiring a chart or age verification — particularly useful in community screening and emergency triage.
CLINICAL PEARL
The single most common error in growth chart interpretation in Indian practice is using an inappropriate reference. The WHO 2006 Child Growth Standards are prescriptive — they describe how children from diverse countries should grow under optimal conditions. When Indian children are plotted against this chart, their median weight and height are slightly lower, so many healthy Indian children appear to be mildly below the 0th centile. This does not mean they are malnourished — it reflects the population difference. For clinical use in India, the IAP 2015 growth charts provide India-specific reference data and should be used where available. However, for classifying SAM (which requires WHO criteria for NRC admission and therapeutic feeding protocols), the WHO z-scores and MUAC cut-offs remain the standard. Know which chart you are using and what it means.
Interpretation of Assessment Findings and Deviation Recognition
Nutritional assessment findings must be integrated across all four domains — anthropometric, dietary, clinical, and biochemical — to arrive at a complete classification. Each domain contributes unique information, and relying on any single domain alone misses important diagnoses. A child may have a normal weight-for-height (no acute wasting) but profound stunting and iron-deficiency anaemia — the anthropometry alone would reassure, while the dietary history and clinical signs reveal a significant problem. Conversely, a child with severe wasting may have normal haemoglobin because the body has redistributed iron to compensate. Integration is not just desirable — it is the minimum standard of care. The clinician must synthesise across all domains before classifying, and must document each component of the assessment in the case record, as this drives the management plan and allows progress monitoring at follow-up visits.
Pattern recognition of nutritional deficits:
• Wasting alone (WHZ < −2, HAZ normal): suggests an acute nutritional insult — recent illness, acute food shortage, acute diarrhoea. The child's potential height is preserved; catching up in weight is relatively rapid with nutritional rehabilitation.
• Stunting alone (HAZ < −2, WHZ normal): suggests chronic, long-standing nutritional deficit — often originating in the first 1000 days. Weight may appear normal for the child's current height even though the child is shorter than expected. Stunting represents a more profound structural deficit and is far less reversible than wasting.
• Both wasting and stunting: the most severe combination — indicates both acute and chronic deprivation. This child is at the highest mortality risk.
• Oedematous malnutrition (kwashiorkor): bilateral pedal oedema in the presence of adequate or even excess carbohydrate intake but severe protein deficit. Weight may be deceptively normal due to fluid retention; the weight gain is oedema fluid, not lean mass. MUAC is a more reliable marker than weight here.
Clinical signs of specific micronutrient deficiency to recognise during physical examination:
• Iron deficiency: conjunctival pallor, koilonychia (spoon-shaped nails), glossitis, angular stomatitis
• Vitamin A deficiency: night blindness (history from caregiver), Bitot's spots (triangular pearlescent spots on temporal bulbar conjunctiva), xerophthalmia
• Vitamin D deficiency: craniotabes (0-6 months), rachitic rosary (6-18 months), bowing of legs in the walking toddler, hypotonia
• Zinc deficiency: acrodermatitis enteropathica (erythematous, vesicobullous, periorificial rash), poor wound healing, growth failure
• Vitamin C deficiency (scurvy): perifollicular haemorrhage, gingival swelling/bleeding, corkscrew hairs
Biochemical markers add specificity to the clinical assessment. Haemoglobin <11 g/dL in children under 5 years and <11.5 g/dL in 5-11 year olds indicates anaemia (WHO criteria); the haematological pattern (MCV, MCH, serum ferritin, RDW) differentiates iron-deficiency anaemia from other causes. Serum albumin <3.5 g/dL indicates protein deficit (though this is a late marker and is affected by inflammation via acute-phase response). Serum 25-OH vitamin D <20 ng/mL = deficiency; 20-30 ng/mL = insufficiency. Serum zinc levels are unreliable in isolation due to acute-phase reactant behaviour.
Diet Planning in Health and Disease
Diet planning translates the assessment findings into a practical prescription that the family can implement with locally available, culturally acceptable, affordable foods. An ideal diet plan for a child must address five domains: energy sufficiency, macronutrient distribution, micronutrient completeness, meal frequency and texture (age-appropriate), and hygiene of preparation. The plan is only as good as its feasibility in the family's real-world context — a prescription that requires expensive ingredients or complex preparation will not be followed. Good diet planning therefore combines knowledge of nutritional science with practical counselling that meets the family where they are. The clinician must first ask: what does this family already feed the child, what is affordable, what is culturally acceptable, and what barriers exist to change? Only then can a specific, actionable prescription be written. A generic 'high-protein, high-calorie diet' without naming foods, quantities, and meal timing is not a diet plan — it is an instruction without content.
The general framework for constructing a diet plan in health:
1. Calculate the daily energy requirement (ICMR-NIN RDA for age or Holliday-Segar formula).
2. Determine the macronutrient distribution: 50-60% from carbohydrates (cereals, root vegetables), 25-35% from fat (cooking oil, ghee, dairy), 10-15% from protein (pulses, eggs, dairy, meat).
3. Distribute across age-appropriate meal frequency: 2-3 meals + 2 snacks for toddlers; 3 meals + 1-2 snacks for school-age children.
4. Include high-iron foods in at least one meal (fortified cereals, dal, leafy vegetables + vitamin C source to improve absorption).
5. Include calcium-rich foods (dairy or alternatives) at every age.
6. Advise on food preparation (consistency matching developmental stage, avoiding over-dilution for weaning foods).
Disease-specific modifications:
• Acute diarrhoea: continue feeding throughout illness (WHO recommendation); do NOT withhold food; increase frequency to 5-6 smaller feeds per day; provide reduced-osmolarity ORS (245 mOsm/L) for rehydration alongside zinc supplementation (10-20 mg/day for 10-14 days); resume full diet as soon as tolerated.
• Fever/infection: metabolic demands increase by 10-12% per degree Celsius above 37°C; maintain or increase feeding frequency to compensate; ensure adequate fluids.
• SAM (in-hospital): use WHO F-75 formula (75 kcal/100 mL) in the stabilisation phase to avoid refeeding syndrome; progress to F-100 (100 kcal/100 mL) in rehabilitation phase; RUTF (Ready-to-Use Therapeutic Food) for uncomplicated SAM at home and in the transition phase.
• Anaemia: prescribe iron-rich diet (fortified cereals, dal, dark-green leafy vegetables, eggs) alongside pharmacological iron supplementation (3-6 mg/kg/day elemental iron); advise concurrent vitamin C foods; avoid tea/coffee with meals.
• Post-surgery or hospitalised children: catch-up feeding requires 150% of estimated average requirement per kg; high-energy-density feeds (oil/ghee enrichment of foods) are more practical than volume increase in small children.