Page 8 of 25
PE10.1-5 | Severe Acute Malnutrition — SDL Guide
Learning Objectives
- Define Severe Acute Malnutrition (SAM) and Moderate Acute Malnutrition (MAM) using WHO diagnostic criteria including weight-for-height z-score, MUAC, and oedema
- Describe the clinical features, pathophysiology, and WHO classification of marasmus, kwashiorkor, and marasmic-kwashiorkor
- Outline the clinical approach and WHO 10-step management protocol for SAM including stabilisation (F-75) and rehabilitation (F-100/RUTF) phases
- Describe the management of life-threatening SAM complications: hypoglycaemia, hypothermia, dehydration with ReSoMal, and infection
- Counsel parents of children with SAM and MAM regarding cause, home feeding, danger signs, and community rehabilitation
- Enumerate the role of F-75, F-100, RUTF, and locally prepared therapeutic foods in SAM management
INSTRUCTIONS
Severe Acute Malnutrition is the most dangerous and immediately life-threatening form of childhood malnutrition. Without treatment, SAM carries a case fatality rate of 20-30%. With appropriate WHO-protocol management in a Nutrition Rehabilitation Centre (NRC), this drops to under 5%. Understanding the 10-step WHO management protocol, the precise diagnostic criteria, the specific therapeutic diets, and the life-threatening metabolic complications is essential for every clinician working with children in India.
References
- Ghai Essential Pediatrics, 9th ed, Ch 7 (Severe Acute Malnutrition) (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch on Malnutrition (textbook)
- WHO Guidelines for the Inpatient Treatment of Severely Malnourished Children, 2003 (guideline)
- NHM Operational Guidelines on Facility-Based Management of SAM, Government of India, 2011 (updated) (guideline)
- IAP Guidelines on Management of Severe Acute Malnutrition, 2013 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 14-month-old boy is brought to the emergency department by his grandmother. He is limp, barely responsive, and has not fed for two days. On examination: temperature 35.1°C, blood glucose 38 mg/dL (2.1 mmol/L), visible rib cage with loose hanging skin folds, weight 5.8 kg (expected ~10 kg at 14 months). MUAC is 10.2 cm. There is no oedema. He is in severe marasmus with hypoglycaemia and hypothermia. He will die within hours without immediate correction of his glucose and temperature — and within days without the right therapeutic feeding sequence. This module teaches you the protocol that will save him.
WHY THIS MATTERS
India bears the highest burden of SAM in the world. NFHS-5 (2019-21) estimated that 7.7% of Indian children under 5 years — approximately 3.8 million children — have severe wasting (weight-for-height < −3 SD). The case fatality rate for untreated SAM is 20-30%; with optimal inpatient management under the WHO protocol, it falls below 5%. India's National Health Mission operates a network of Nutrition Rehabilitation Centres (NRCs) that provide inpatient SAM care using the WHO 10-step protocol and F-75/F-100/RUTF feeding. As a final-year student and future intern, you will identify SAM cases, initiate emergency stabilisation, refer appropriately to NRC, and counsel families post-discharge. Each of these roles requires precise knowledge of criteria, protocol, and therapeutic foods.
RECALL
From the Nutritional Assessment module, recall the WHO SAM diagnostic criteria: weight-for-height < −3 SD, MUAC <11.5 cm (6-59 months), or bilateral pedal oedema — any ONE criterion is sufficient for SAM. From physiology, recall the metabolic consequences of prolonged starvation: glycogen depletion within 12-16 hours, followed by gluconeogenesis from amino acids and glycerol, followed by ketone body production from fatty-acid oxidation. From biochemistry, recall that albumin is synthesised in the liver; its serum half-life is approximately 20 days, so hypoalbuminaemia in kwashiorkor reflects weeks-to-months of protein deficit. From pharmacology, recall that 50% dextrose (D50W) is the hypertonic glucose used for hypoglycaemia in adults — in children, the correct concentration is 10% dextrose (D10W) to avoid osmotic injury; this distinction is clinically critical.
Clinical Presentation of SAM and MAM
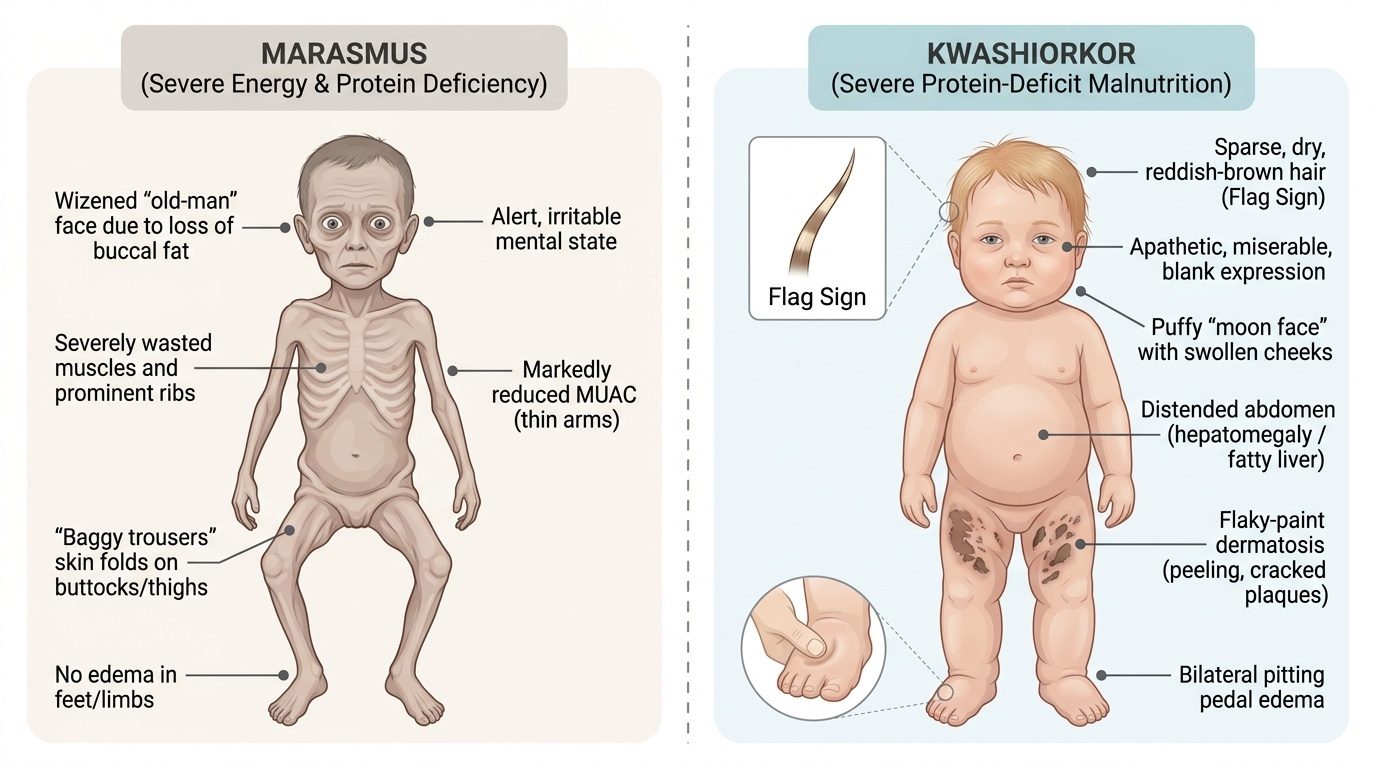
The clinical presentation of SAM depends on whether the predominant deficit is energy (marasmus) or protein (kwashiorkor), or both. Recognising the clinical pattern is essential for correct classification and for anticipating specific complications.
Provided image
Marasmus (from Greek 'marasmos' — wasting) is caused by severe, sustained deficiency of both energy and protein. The body mounts a catabolic adaptation — catabolising its own muscle and fat stores to provide energy for vital organs. The result is severe wasting: the child has a dramatically low weight-for-height, prominent ribs and scapulae, loss of the buccal fat pad (producing the characteristic 'old-man face' or 'wizened face'), loose skin folds hanging at the inner thighs and buttocks ('baggy trousers' sign), and markedly reduced MUAC. Despite the profound wasting, there is no oedema in uncomplicated marasmus. The child is typically alert (sometimes irritable) and may have a voracious appetite — this preserved or increased appetite is characteristic and prognostically important (it distinguishes marasmus from kwashiorkor, where anorexia is the rule). Skin and hair are usually normal in pure marasmus.
Kwashiorkor (derived from the Ga language of Ghana: 'displaced child' — the child displaced from the breast by a younger sibling) presents differently. The cardinal feature is bilateral pitting pedal oedema, which is the defining diagnostic feature. The oedema is dependent — beginning in the feet/ankles and extending upward to the face (moon face) in severe cases. Other features: flaky-paint dermatosis (superficial skin cracking with hyperpigmented, peeling plaques — most prominent in skin folds and pressure areas); hair changes (thin, sparse, reddish-brown or whitish discolouration from melanin depletion; straight or silky texture in a previously curly-haired child; easy pluckability — the 'flag sign' describes bands of depigmented hair alternating with normal hair, corresponding to periods of kwashiorkor and recovery); hepatomegaly from fatty infiltration of the liver; apathy and misery (the child does not cry or protest, stares blankly — contrasting with the irritability of marasmus); and anorexia (makes feeding extremely difficult).
Marasmic-kwashiorkor is the combination: severe wasting (weight-for-height < −3 SD) with bilateral oedema. This is the most severe form and carries the highest mortality risk. Both the energetic and protein compartments are severely depleted, and the oedema may mask the degree of wasting — the child may appear 'heavier' than the underlying lean mass would suggest.
MAM (Moderate Acute Malnutrition) presents with weight-for-height between −2 and −3 SD or MUAC between 11.5 and 12.5 cm, without oedema. The child may look thin but does not have the dramatic clinical features of SAM. MAM is managed at the community level and does not require NRC admission.
Pathophysiology and Aetiology of SAM
The pathophysiology of SAM differs fundamentally between marasmus and kwashiorkor, though both ultimately reflect an imbalance between nutrient intake and the body's metabolic requirements during a period of rapid growth.
Aetiology of SAM in the Indian context is multifactorial. The immediate cause is inadequate dietary intake relative to requirements — but this is always embedded in intermediate causes (poor complementary feeding, maternal illness affecting breastfeeding, food insecurity, recurrent infections increasing catabolism) and underlying causes (household food insecurity, inadequate care practices, poor water/sanitation and hygiene — the UNICEF 'Triple A' framework: Availability, Access, Absorption). Recurrent diarrhoeal and respiratory infections are both a consequence of malnutrition (immune suppression) and a cause (anorexia, increased catabolism) — creating a vicious cycle that accelerates nutritional decline.
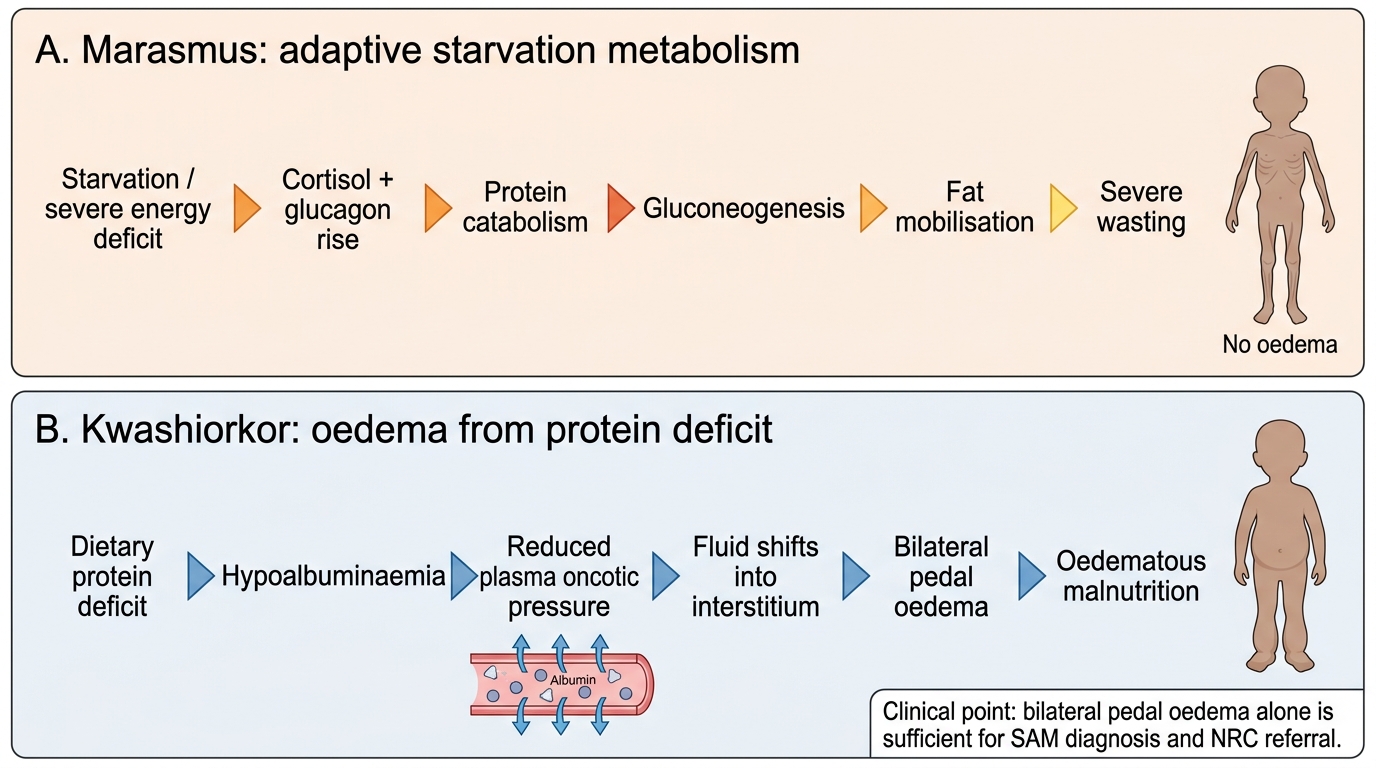
Pathophysiology of marasmus is a glucocorticoid/glucagon-driven catabolic state:
• Prolonged energy deficit → blood glucose falls → glucagon rises, insulin falls, cortisol rises
• Glycogen stores depleted within 12-16 hours → gluconeogenesis activated using amino acids from muscle proteolysis
• Fat stores mobilised (lipolysis) → fatty acid oxidation → ketone body production (provides brain fuel)
• Progressive loss of subcutaneous fat → wasting of temporal muscles, buccal fat pad, interosseous muscles
• The child is effectively 'auto-cannibalising' muscle and fat to survive
• Metabolic rate per kilogram is maintained or reduced — this is an adaptive, not maladaptive, response
Pathophysiology of kwashiorkor involves protein deficit with relatively preserved caloric intake (typically a cereal-based diet with very low protein). The exact mechanism remains debated, but the central event is hypoalbuminaemia:
• Protein deficit → reduced hepatic albumin synthesis → serum albumin falls (below 2.5 g/dL in severe kwashiorkor)
• Reduced oncotic pressure → fluid shifts from intravascular to interstitial compartment → oedema
• Concurrent electrolyte imbalance: hypokalaemia (potassium deficit from poor intake and renal/diarrhoeal losses), hypomagnesaemia, and hyponatraemia (dilutional)
• Fatty liver: excess carbohydrate intake + insufficient apolipoprotein synthesis (protein-limited) → triglyceride accumulation in hepatocytes → hepatomegaly
• Immune suppression: reduced T-lymphocyte function, impaired complement activity, low secretory IgA → susceptibility to overwhelming infection
Metabolic Adaptation in Marasmus and Kwashiorkor
WHO Classification and Diagnostic Criteria
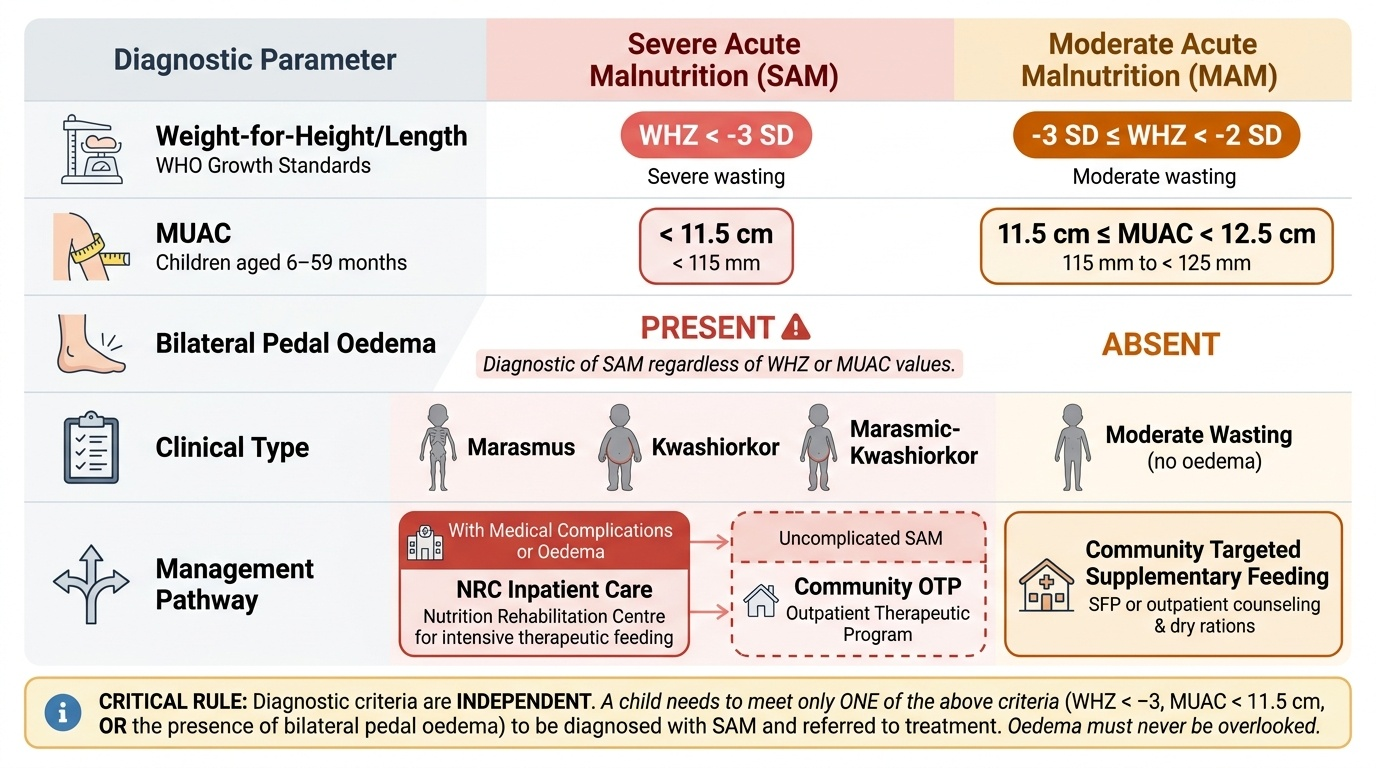
The WHO diagnostic criteria for SAM are precise, internationally validated, and operationally critical — they determine which children receive inpatient therapeutic feeding and which are managed in the community. Every clinician who sees children must be able to apply these criteria rapidly and accurately. These criteria are not interchangeable with Gomez or Waterlow classifications, which are older systems; the WHO z-score criteria and MUAC cut-offs are the operative thresholds for the NHM NRC admission protocol in India. Crucially, the three criteria are independent: a child need only meet ONE to be classified as SAM — they are not cumulative, nor does the absence of one exclude the diagnosis when another is present. The most commonly missed criterion in clinical practice is bilateral pedal oedema — practitioners sometimes overlook it because the child may not appear severely wasted, yet oedema alone is sufficient for the SAM diagnosis and NRC referral.
Provided image
The three WHO diagnostic criteria for SAM are:
1. Weight-for-height z-score (WHZ) < −3 SD (or <70% of the weight median for height using NCHS reference in older systems)
2. MUAC <11.5 cm for children aged 6-59 months
3. Bilateral pedal oedema of nutritional origin
Any ONE of the above three criteria, in a child aged 6-59 months, constitutes SAM and indicates need for therapeutic intervention. The presence of bilateral oedema alone — even if weight-for-height is normal — classifies the child as having oedematous malnutrition (kwashiorkor) and the child requires NRC-level management.
For the WHO classification by type:
• Marasmus: WHZ < −3 SD or MUAC <11.5 cm, no oedema
• Kwashiorkor: bilateral oedema present (oedema grade 1-3: 1 = feet/ankles only, 2 = feet + lower legs, 3 = generalised including face)
• Marasmic-kwashiorkor: WHZ < −3 SD + bilateral oedema
MAM is diagnosed when: WHZ is between −2 and −3 SD, or MUAC is 11.5-12.5 cm, without oedema.
Triage to inpatient vs community management is based not only on anthropometric severity but on the presence of medical complications:
• Inpatient NRC (hospital-based) for: SAM with any medical complication (pneumonia, severe diarrhoea, sepsis, severe anaemia, hypoglycaemia, hypothermia, altered consciousness, persistent vomiting, intractable diarrhoea) OR failed appetite test (child refuses RUTF) OR no carer at home
• Outpatient/Community-based management (CbM) via NHM for: uncomplicated SAM (no medical complication) + passes appetite test + alert child with a motivated carer
The appetite test is performed by offering the child approximately 1/4 sachet of RUTF. A child who eats it with interest, not just a few bites, passes the test — indicating the anorexia of severe kwashiorkor or infection is absent or mild. A failed appetite test indicates inpatient management is required regardless of other findings.
SELF-CHECK
An 18-month-old girl has weight-for-height z-score of −2.8 SD, MUAC of 11.3 cm, and bilateral pitting oedema to the ankles. How should she be classified?
A. MAM only — managed in community with RUTF
B. Marasmus — WHZ < −3 SD required for SAM
C. Kwashiorkor — bilateral oedema alone is sufficient for SAM diagnosis
D. Marasmic-kwashiorkor — WHZ < −3 SD + oedema
Reveal Answer
Answer: C. Kwashiorkor — bilateral oedema alone is sufficient for SAM diagnosis
Bilateral pedal oedema of nutritional origin alone is sufficient for a SAM diagnosis — this child has kwashiorkor, regardless of whether the WHZ meets the < −3 SD threshold. The WHZ of −2.8 SD would classify as MAM by anthropometry alone, but the presence of oedema overrides this and classifies the child as SAM (kwashiorkor). She requires NRC inpatient management, not community-level care. Option D (marasmic-kwashiorkor) would require WHZ < −3 SD plus oedema — this child's WHZ is −2.8, not below −3.