Page 13 of 33
PE12.7 | B Complex Vitamins — SDL Guide
Learning Objectives
- List all eight B complex vitamins, their coenzyme forms, and principal metabolic roles
- Identify the main dietary sources of each B vitamin and the groups at risk of deficiency
- Describe the mechanisms by which deficiency of each B vitamin arises in paediatric patients
- Recognise and diagnose the key deficiency syndromes: beriberi (B1), pellagra (B3), megaloblastic anaemia (B9/B12), and pyridoxine-responsive seizures (B6)
- Outline the management of each B complex deficiency syndrome with correct doses and routes
INSTRUCTIONS
B complex vitamin deficiencies remain clinically relevant in India, particularly in children from food-insecure families, exclusively breastfed infants of nutritionally depleted mothers, and communities dependent on monotonous cereal-based diets. This module gives you a systematic understanding of all eight B vitamins — their biochemistry, dietary sources, mechanisms of deficiency, and the distinct clinical syndromes they produce — equipping you to diagnose and manage these conditions in your clinical rotations.
References
- Ghai Essential Pediatrics, 9th ed, Ch 8 — Nutrition (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch 63 — Vitamin Deficiencies (textbook)
- IAP Recommended Dietary Allowances and Upper Limits, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-month-old exclusively breastfed boy from a rural household is rushed to the emergency department with acute onset restlessness, refusal to feed, and a sudden high-pitched cry. His mother is a strict vegetarian who has not received any postnatal nutritional supplementation. On examination the infant is pale, tachycardic, and his liver is palpable 3 cm below the costal margin. The abdomen is distended. His peripheries are cool and he appears puffy around the face. What B vitamin deficiency could explain this constellation of cardiovascular collapse in an apparently well-fed infant whose mother's diet is nutritionally restricted?
WHY THIS MATTERS
B complex vitamins are essential cofactors in energy metabolism, DNA synthesis, neurological function, and red-cell production. Although each can be obtained from a balanced diet, paediatric patients are uniquely vulnerable: infants of vegan or malnourished mothers receive inadequate amounts through breast milk; children on monotonous maize-based diets are at risk of pellagra; adolescents on restricted diets may develop subacute B12 deficiency without obvious clinical features until neurological damage is irreversible. In Indian primary-care settings, recognition of beriberi, pellagra, and megaloblastic anaemia can be life-saving. As a final-year student, you must be able to distinguish B vitamin deficiency syndromes clinically — before laboratory confirmation is available.
RECALL
Before you proceed, recall from your Biochemistry and Physiology studies:
• Water-soluble vitamins are not stored in significant amounts; hence continuous dietary supply is critical and deficiency develops faster than for fat-soluble vitamins.
• Coenzymes are small organic molecules that partner with apoenzymes to carry out catalysis; without the coenzyme, the entire metabolic step is blocked.
• One-carbon transfer reactions (from folate/B12) are fundamental to nucleotide synthesis and hence to cell division.
• Energy metabolism: glucose → pyruvate → acetyl-CoA requires thiamine (B1) as a coenzyme; failure of this step accumulates lactate and pyruvate, leading to lactic acidosis.
• Neural tube closure occurs at 28 days post-conception, before a pregnancy is often confirmed — this is why periconceptional folate is critical.
Overview of B Complex Vitamins: Roles and Sources
The B complex is a family of eight chemically distinct, water-soluble vitamins that share the property of being essential coenzymes in intermediary metabolism. Although they are grouped together, their biochemical roles, deficiency syndromes, and clinical manifestations differ substantially. As a group they participate in energy extraction from macronutrients, red-blood-cell production, maintenance of neural integrity, and synthesis of genetic material. The family includes thiamine (B1), riboflavin (B2), niacin (B3), pantothenic acid (B5), pyridoxine (B6), biotin (B7), folate (B9), and cobalamin (B12). Their water-solubility means excess is excreted in urine, which limits toxicity but also means tissue stores are small — deficiency can develop within weeks to months on a deficient diet. In children, the consequences of deficiency are amplified because rapid growth increases demand; deficiency during critical developmental windows — especially the first two years of life — can cause irreversible neurological damage. Globally, the most clinically significant B vitamin deficiencies in paediatric practice are those of thiamine (beriberi), niacin (pellagra), folate and cobalamin (megaloblastic anaemia), and pyridoxine (B6-responsive seizures in neonates). India carries a significant burden of these conditions, especially in undernourished rural and tribal populations.
- Thiamine (B1): found in whole grains, legumes, pork, yeast; destroyed by prolonged cooking and polished-rice diets.
- Riboflavin (B2): dairy products, organ meats, eggs, leafy greens.
- Niacin (B3): meat, poultry, fish, groundnuts; can be synthesised from tryptophan (60 mg tryptophan = 1 mg niacin equivalent).
- Pantothenic acid (B5): widely distributed; deficiency is rare except in severe malnutrition.
- Pyridoxine (B6): meat, fish, poultry, bananas, legumes.
- Biotin (B7): eggs (yolk), liver, nuts; deficiency rare but occurs with raw egg-white consumption (avidin binds biotin) or prolonged parenteral nutrition.
- Folate (B9): green leafy vegetables, legumes, liver, fortified cereals; heat-labile.
- Cobalamin (B12): exclusively from animal products (meat, dairy, eggs, fish); vegans/strict vegetarians and their exclusively breastfed infants are at risk.
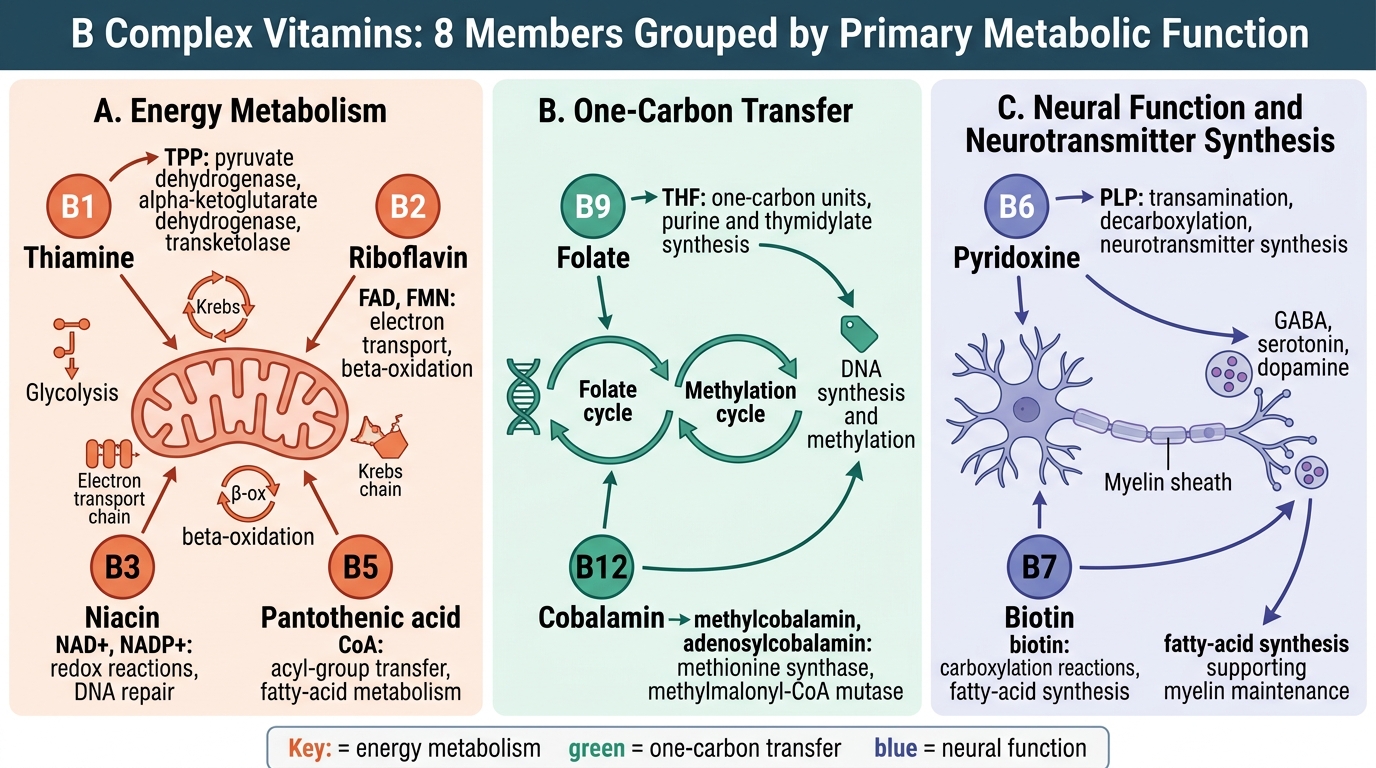
B Complex Vitamins by Primary Metabolic Function
Normal Functions: Coenzyme Roles and Dietary Sources
Each B vitamin is converted intracellularly into an active coenzyme form that acts as a cofactor for specific enzyme-catalysed reactions. Understanding the coenzyme role helps predict the metabolic consequence of deficiency and thus the clinical syndrome. Thiamine pyrophosphate (TPP), the active form of B1, is an obligate coenzyme for pyruvate dehydrogenase, alpha-ketoglutarate dehydrogenase, and transketolase in the pentose phosphate pathway. Blockade of pyruvate dehydrogenase prevents conversion of pyruvate to acetyl-CoA, causing pyruvate and lactate to accumulate; cells that rely heavily on glucose — neurones and cardiac myocytes — are the first to fail. Riboflavin (B2) is the precursor of FAD (flavin adenine dinucleotide) and FMN (flavin mononucleotide), electron carriers in the mitochondrial respiratory chain and in fatty-acid beta-oxidation; deficiency causes angular stomatitis, glossitis, and corneal vascularisation but is rarely life-threatening alone. Niacin (B3) is converted to NAD+ and NADP+, which participate in hundreds of redox reactions including glycolysis, Krebs cycle, and fatty-acid synthesis; NAD+ is also a substrate for ADP-ribosylation and PARP activity (DNA repair). Pyridoxal phosphate (PALP), the active form of B6, is a coenzyme for over 100 enzyme reactions, notably aminotransferases (transamination), decarboxylases (neurotransmitter synthesis — GABA, serotonin, dopamine), glycogen phosphorylase, and sphingolipid synthesis. Neonatal pyridoxine-dependent epilepsy results from a defect in the enzyme antiquitin, causing accumulation of pipecolic acid, or from inadequate dietary B6, and is treated with IV/oral pyridoxine. Folate (B9) is converted to tetrahydrofolate (THF), which carries one-carbon units critical for purine and thymidylate synthesis (DNA) and for methionine regeneration; deficiency impairs DNA synthesis, causing megaloblastic changes in all rapidly dividing cells — especially erythroid precursors and mucosa. Cobalamin (B12) is required for two reactions: methylcobalamin regenerates methionine from homocysteine (linked to folate cycle) and adenosylcobalamin allows methylmalonyl-CoA to be converted to succinyl-CoA (important in myelin synthesis); deficiency causes megaloblastic anaemia AND — uniquely — subacute combined degeneration (SCD) of the spinal cord, which folate deficiency does NOT cause.
Provided image
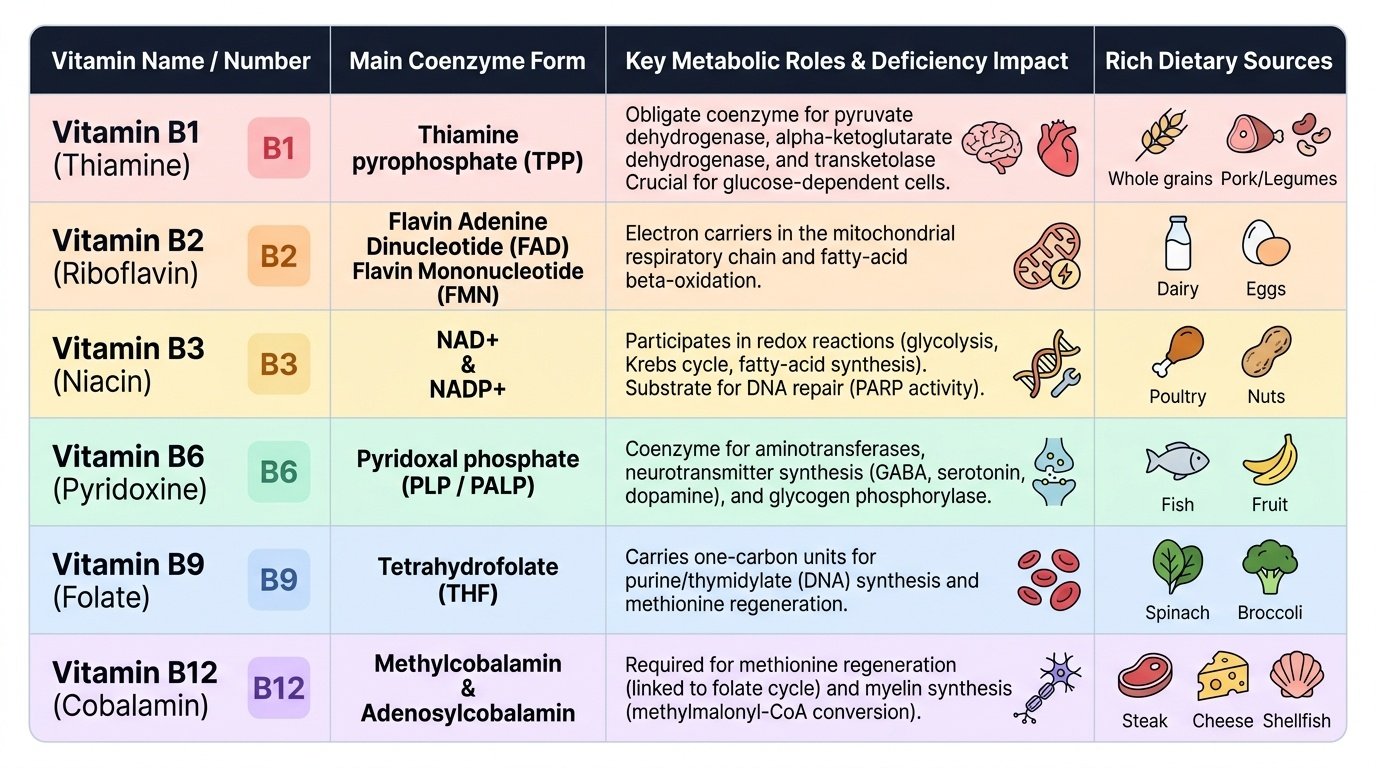
| Vitamin | Active coenzyme | Key role | Sources |
|---|---|---|---|
| B1 (thiamine) | TPP | Pyruvate dehydrogenase, TCA cycle | Whole grains, legumes, pork |
| B2 (riboflavin) | FAD, FMN | Electron transport, beta-oxidation | Dairy, eggs, organ meats |
| B3 (niacin) | NAD+, NADP+ | Redox reactions (glycolysis, TCA) | Meat, fish, groundnuts |
| B6 (pyridoxine) | PALP | Transamination, neurotransmitter synthesis | Meat, bananas, legumes |
| B9 (folate) | THF | One-carbon transfer, DNA synthesis | Green leafy vegetables, legumes |
| B12 (cobalamin) | Methylcobalamin, AdoCbl | Methionine synthesis, myelin maintenance | Animal products only |
SELF-CHECK
A 3-month-old breastfed infant presents with acute cardiac failure. His mother is a strict vegetarian on a rice-based diet without supplementation. Which vitamin deficiency is most likely responsible?
A. Riboflavin (B2) deficiency causing angular stomatitis
B. Thiamine (B1) deficiency causing infantile wet beriberi
C. Cobalamin (B12) deficiency causing megaloblastic anaemia
D. Niacin (B3) deficiency causing pellagra
Reveal Answer
Answer: B. Thiamine (B1) deficiency causing infantile wet beriberi
Infantile wet beriberi (thiamine/B1 deficiency) classically presents before 6 months in exclusively breastfed infants of thiamine-deficient mothers. It manifests as acute cardiac failure with oedema (wet = cardiovascular). Thiamine is critical for cardiac muscle energy metabolism via pyruvate dehydrogenase. Riboflavin deficiency causes mucocutaneous features, not cardiac failure. B12 deficiency causes megaloblastic anaemia and neurological regression, not cardiac failure. Pellagra is seen in older children on maize-based diets.
Mechanisms of Deficiency
B complex vitamin deficiency in paediatric patients arises through several distinct mechanisms, and recognising the mechanism helps identify the at-risk child before overt clinical illness develops. Dietary inadequacy is the most common pathway: exclusive reliance on polished white rice depletes thiamine (the bran is removed); corn/maize diets deplete niacin because bound niacytin in maize is bioavailable only when the grain is processed with alkali (nixtamalisation), and maize protein is also tryptophan-poor; strict plant-based diets eliminate all dietary sources of B12 since cobalamin is found exclusively in animal products. Maternal deficiency transmitted via breast milk is particularly important for thiamine, B12, and folate — an infant's only dietary source in the first months of life is breast milk, and if the mother's stores are depleted, the infant becomes deficient despite appearing clinically breastfed. This is the mechanism in the hook scenario. Malabsorption contributes to B12 deficiency when gastric intrinsic factor production fails (juvenile pernicious anaemia, a rare autoimmune condition) or when the terminal ileum — the sole absorption site for the B12–intrinsic-factor complex — is inflamed or resected. Crohn's disease and post-surgical short bowel syndrome are important causes in older children. Drug-induced deficiency is underappreciated: isoniazid (INH, used in TB prophylaxis/treatment) competitively inhibits pyridoxine phosphokinase, precipitating B6 deficiency and peripheral neuropathy — this is why pyridoxine is co-prescribed with INH in children; metformin (used in adolescents with T2DM or PCOS) reduces B12 absorption by an ileal mechanism and requires B12 monitoring. Increased demand from rapid growth in infancy and adolescence, or from haemolytic disorders (increased folate use for erythropoiesis), can expose marginal dietary intake. Cooking practices destroy heat-labile folate and thiamine; food fortification gaps in rural areas compound the problem.
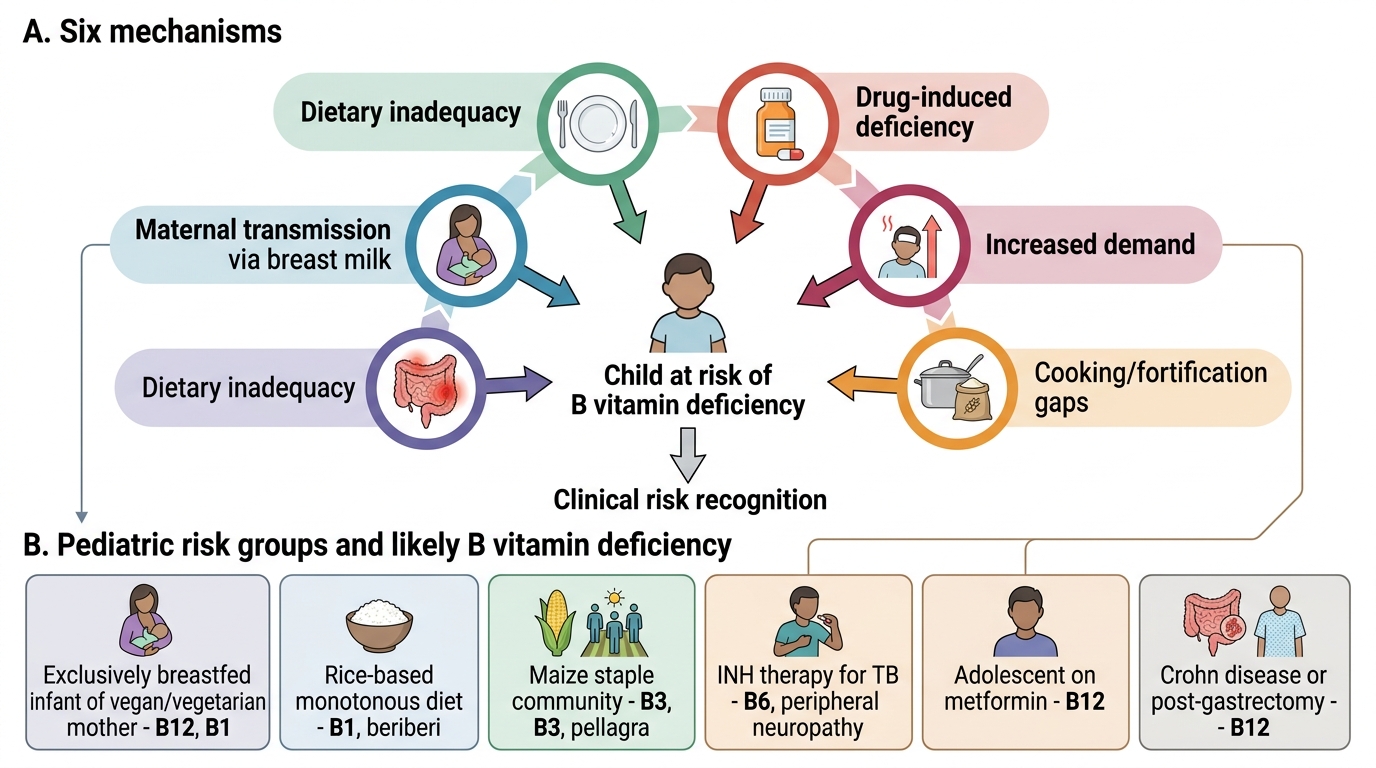
Mechanisms of B Vitamin Deficiency in Children
- Key at-risk groups in paediatric practice:
- Exclusively breastfed infants of vegan/vegetarian mothers → B12, B1
- Infants/children on rice-based monotonous diets → B1 (beriberi)
- Children in communities eating maize as the staple → B3 (pellagra)
- Children on INH therapy for TB → B6 (peripheral neuropathy)
- Adolescents on metformin → B12
- Children with Crohn's disease or post-gastrectomy → B12