Page 20 of 33
PE13.1-2 | Iron Nutrition — SDL Guide (Part 2)
Clinical Features, Diagnosis, and Treatment of IDA
The clinical presentation of iron deficiency anaemia in children spans a wide spectrum, from entirely asymptomatic states detectable only on screening, to severe symptomatic anaemia with cardiac decompensation requiring urgent intervention. The signs and symptoms vary with the severity of deficiency, the rapidity of its onset, and the age of the child. An important clinical point is that mild-to-moderate IDA is frequently missed in routine outpatient encounters because children compensate physiologically: heart rate rises, 2,3-DPG increases in red cells (shifting the oxygen dissociation curve rightward), and cardiac output increases — so the child may appear deceptively well until anaemia is severe. Additionally, the neurobehavioural manifestations of iron deficiency — irritability, reduced attention span, and pica — may precede haematological anaemia by weeks to months and are often attributed to behavioural or social causes. Applying the correct Hb cut-off for the child's age is essential, because adult thresholds would miss significant anaemia in young children.
Clinical features:
• General: pallor of skin, conjunctivae, tongue, nail beds, and palmar creases; the most sensitive site for pallor examination in children is the conjunctivae.
• Neurobehavioural: irritability, reduced attention span, developmental delay or regression, pica (craving for non-food substances — clay, paper, ice, chalk), fatigue and exercise intolerance.
• Cardiovascular: tachycardia, flow murmur, and in severe anaemia, cardiac failure (high-output).
• Other: glossitis, angular stomatitis, koilonychia (spoon-shaped nails, seen in chronic iron deficiency), hepatosplenomegaly (mild, from extramedullary haematopoiesis in severe chronic cases).
• Growth: failure to thrive is common in chronic severe IDA.
Diagnostic criteria — WHO Hb cut-offs for anaemia:
• 6 months to 5 years: Hb <11 g/dL
• 5 to 11 years: Hb <11.5 g/dL
• 12 to 14 years: Hb <12 g/dL
Laboratory profile of IDA:
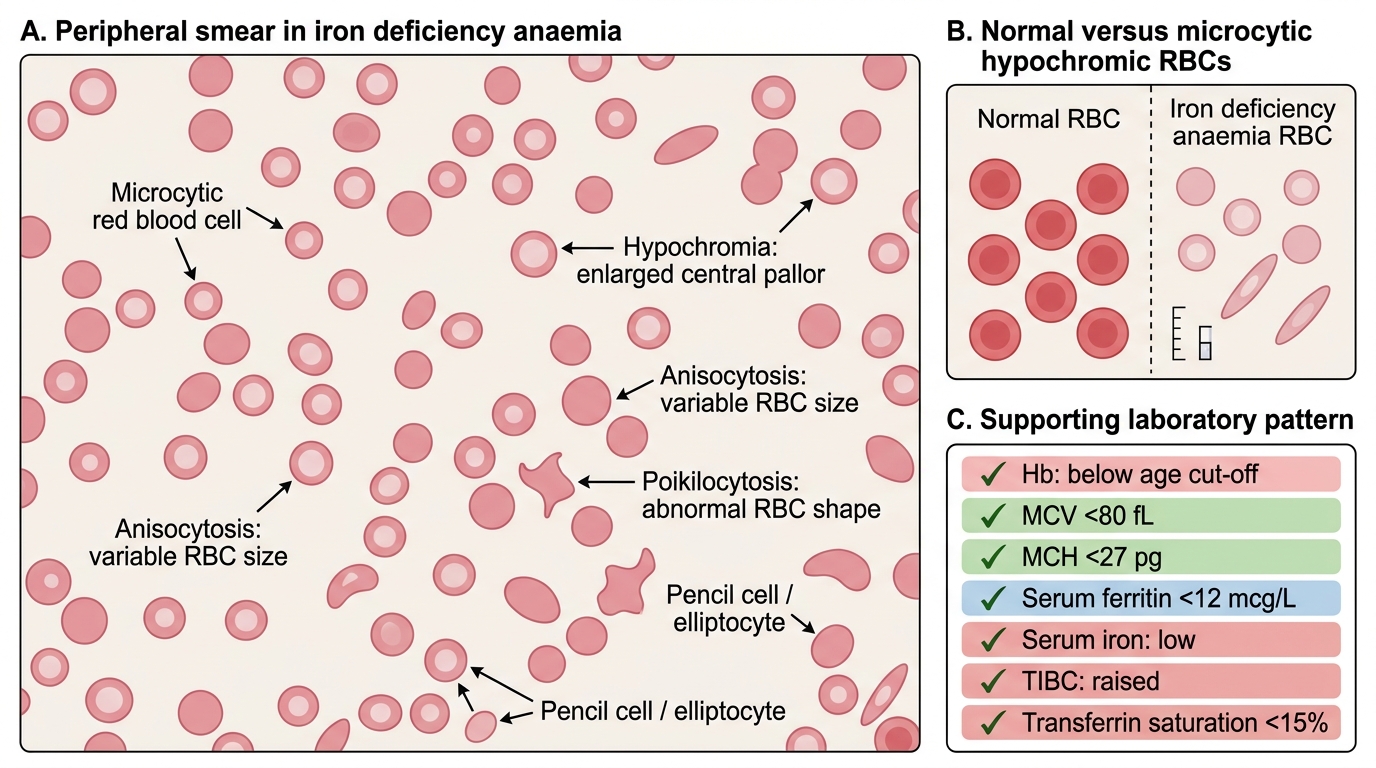
Peripheral Smear in Iron Deficiency Anaemia
| Parameter | Iron deficiency anaemia | Normal |
|---|---|---|
| Haemoglobin | Below cut-off for age | Age-appropriate |
| MCV | <80 fL (microcytic) | 80–100 fL |
| MCH | <27 pg (hypochromic) | 27–33 pg |
| Serum ferritin | <12 mcg/L | 15–200 mcg/L |
| Serum iron | Low | Normal |
| TIBC | Raised | 250–370 mcg/dL |
| Transferrin saturation | <15% | 20–45% |
| Peripheral smear | Microcytic hypochromic, anisocytosis, poikilocytosis | Normocytic normochromic |
Treatment of IDA:
Oral elemental iron is the treatment of choice. The therapeutic dose is 3–6 mg/kg/day of elemental iron in 2–3 divided doses, given between meals (not with milk or tea) to maximise absorption. Giving with vitamin C (orange juice, guava) enhances absorption. The preparation most commonly used in India is ferrous sulphate syrup or drops (containing 25 mg elemental iron per 5 mL) or ferrous ascorbate. Continue treatment for at least 3 months after normalisation of Hb to replenish body stores — stopping when the Hb normalises leads to rapid relapse. Response monitoring: reticulocyte count rises within 5–7 days; Hb should rise by ≥1 g/dL in 4 weeks; failure to respond suggests non-compliance, wrong diagnosis (thalassaemia trait, inflammation), or ongoing blood loss. Parenteral iron (iron sucrose, ferric carboxymaltose) is reserved for cases of malabsorption, severe non-compliance, or very severe anaemia requiring rapid repletion.
CLINICAL PEARL
Three iron-dosing traps in clinical practice:
1. The therapeutic dose of 3–6 mg/kg/day of elemental iron is NOT the same as the NIPI programme dose. The programme doses (IFA syrup 1 mL/day biweekly, pink tablet 45 mg weekly) are preventive/prophylactic doses for healthy children. A child with manifest IDA requires the full therapeutic dose — do not treat established anaemia with the programme dose.
2. Do not stop iron when the Hb normalises. It takes approximately 3 months after Hb normalisation to replenish depleted iron stores; stopping early causes rapid relapse and another episode of IDA.
3. Milk, tea, and antacids given with iron dramatically reduce absorption. Instruct parents to give the iron preparation between meals, not with milk or tea; a small amount of orange juice or citrus squash co-administered can double the absorbed dose from the same tablet.
National Anaemia Control Programme: NIPI and Anaemia Mukt Bharat
The National Iron Plus Initiative (NIPI), launched by the Ministry of Health and Family Welfare in 2013 and subsequently integrated into the Anaemia Mukt Bharat (AMB) strategy in 2018 under the POSHAN Abhiyaan umbrella, is India's comprehensive programme to reduce the burden of anaemia through universal iron and folic acid (IFA) supplementation, dietary diversification, deworming, and behaviour change communication. The programme targets all major at-risk groups across the lifecycle, with specific formulations and delivery platforms for each age group. The goal of AMB is to reduce the prevalence of anaemia by 3 percentage points per year, prioritising children under 5, school-age children, adolescents, and women of reproductive age.
Provided image
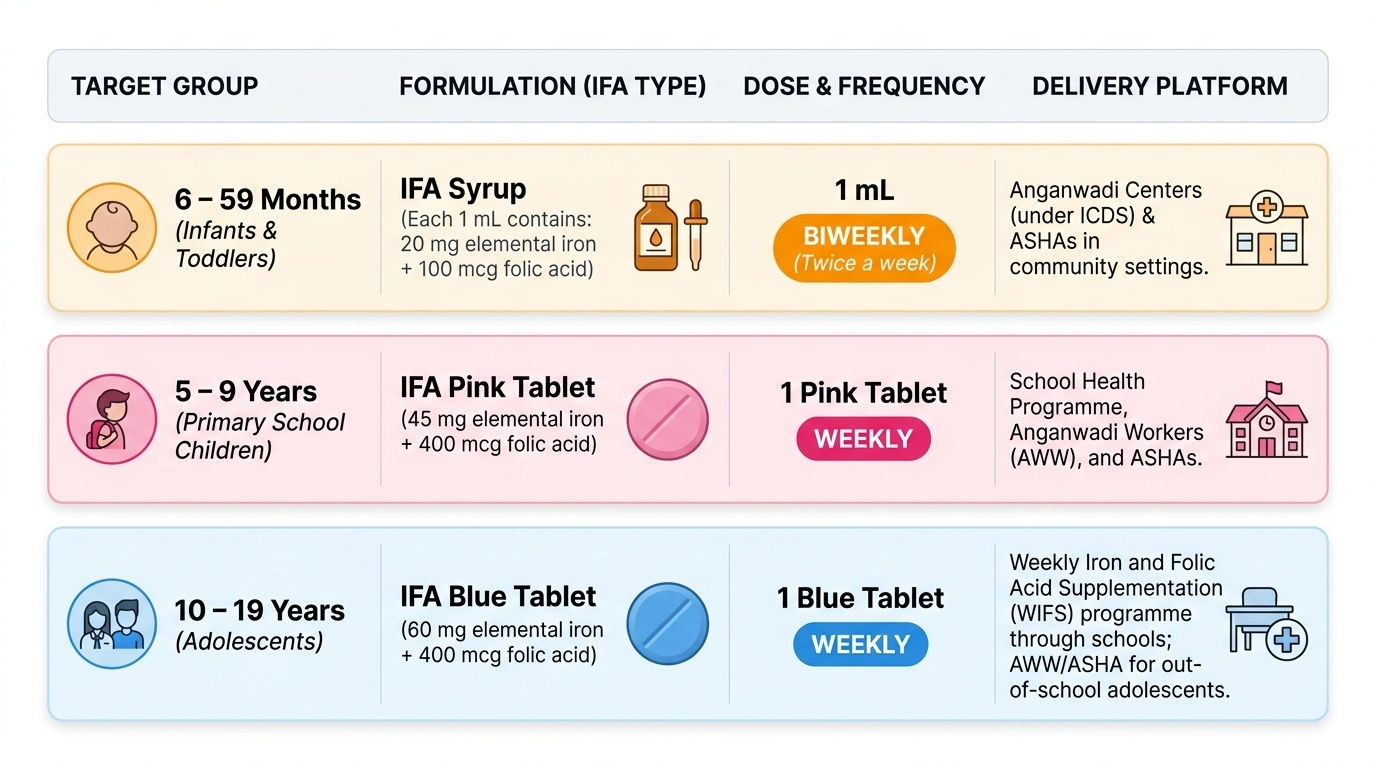
IFA supplementation schedule under NIPI/Anaemia Mukt Bharat:
Target group 1 — Children 6–59 months:
Formulation: IFA syrup — 1 mL contains 20 mg elemental iron + 100 mcg folic acid.
Dose and frequency: 1 mL given BIWEEKLY (twice a week, not daily — weekly dosing was found to have better compliance and lower gastrointestinal side effects than daily dosing in field conditions).
Delivery: Anganwadi workers under ICDS (Integrated Child Development Services), ASHAs, and AWW in community settings.
Target group 2 — Children 5–9 years:
Formulation: IFA pink tablet — contains 45 mg elemental iron + 400 mcg folic acid.
Dose and frequency: 1 pink tablet WEEKLY.
Delivery: School Health Programme, AWW, ASHA.
Target group 3 — Adolescents 10–19 years and reproductive-age women (non-pregnant):
Formulation: IFA blue tablet — contains 60 mg elemental iron + 400 mcg folic acid.
Dose and frequency: 1 blue tablet WEEKLY.
Delivery: Weekly Iron and Folic Acid Supplementation (WIFS) programme through schools (adolescents) and AWW/ASHA (out-of-school adolescents and women).
Target group 4 — Pregnant women:
Formulation: IFA large tablet — 100 mg elemental iron + 500 mcg folic acid.
Dose and frequency: 1 tablet daily for 180 days during pregnancy and 180 days postpartum.
Other AMB pillars (beyond IFA supplementation):
• Deworming (biannual albendazole under National Deworming Day — NDD) since helminthiasis causes chronic blood loss and reduces iron absorption.
• Fortification of staple foods (rice fortification under PDS, fortified supplementary nutrition in ICDS).
• Dietary diversification counselling through ASHAs, AWWs, and nutrition counsellors.
• Behaviour change communication (BCC) addressing IFA compliance, dietary practices, and early introduction of iron-rich complementary foods.
SELF-CHECK
Under the Anaemia Mukt Bharat programme, what is the correct dose and frequency of IFA syrup for a 2-year-old child?
A. 1 mL (20 mg elemental iron) daily for 100 days
B. 2 mL (40 mg elemental iron) daily for 6 months
C. 1 mL (20 mg elemental iron) twice a week (biweekly)
D. 5 mL (100 mg elemental iron) once a week
Reveal Answer
Answer: C. 1 mL (20 mg elemental iron) twice a week (biweekly)
The NIPI/Anaemia Mukt Bharat schedule for children aged 6–59 months is IFA syrup 1 mL (containing 20 mg elemental iron + 100 mcg folic acid) given BIWEEKLY (twice per week). This is a preventive/prophylactic dose — not a therapeutic dose. The biweekly schedule was adopted because weekly/biweekly dosing has equivalent efficacy to daily dosing for prevention but significantly better adherence and fewer gastrointestinal side effects in field conditions. Daily dosing for 100 or 180 days is the schedule for pregnant women (a different formulation), not for children 6–59 months.
Self-Assessment
Iron deficiency anaemia requires you to integrate clinical reasoning (which stage of IDA is this child at?), laboratory interpretation (applying the correct Hb cut-off for age), and programme knowledge (what dose should this child have been receiving under NIPI?). These vignettes test all three dimensions. For each one, work through the diagnosis systematically before looking at the questions — state the Hb cut-off you are applying, what the blood picture tells you about the stage and mechanism, and then identify the correct programme response.
Vignette 1: A 4-year-old boy is brought to the OPD with pallor and tiredness of 3 months duration. He is exclusively vegetarian. His Hb is 8.5 g/dL, MCV 68 fL, serum ferritin 6 mcg/L, TIBC raised. He has pica (eats chalk).
• Is this child anaemic? State the age-appropriate Hb threshold.
• What is the laboratory stage of iron deficiency?
• What dose of elemental iron will you prescribe for treatment?
• What dietary advice will you give regarding iron absorption?
Vignette 2: An Anganwadi worker asks you to clarify the correct NIPI supplementation schedule for the children in her centre. She has a 3-year-old and a 7-year-old.
• What formulation, dose, and frequency should the 3-year-old receive?
• What formulation, dose, and frequency should the 7-year-old receive?
• Name one other AMB programme component beyond IFA supplementation.
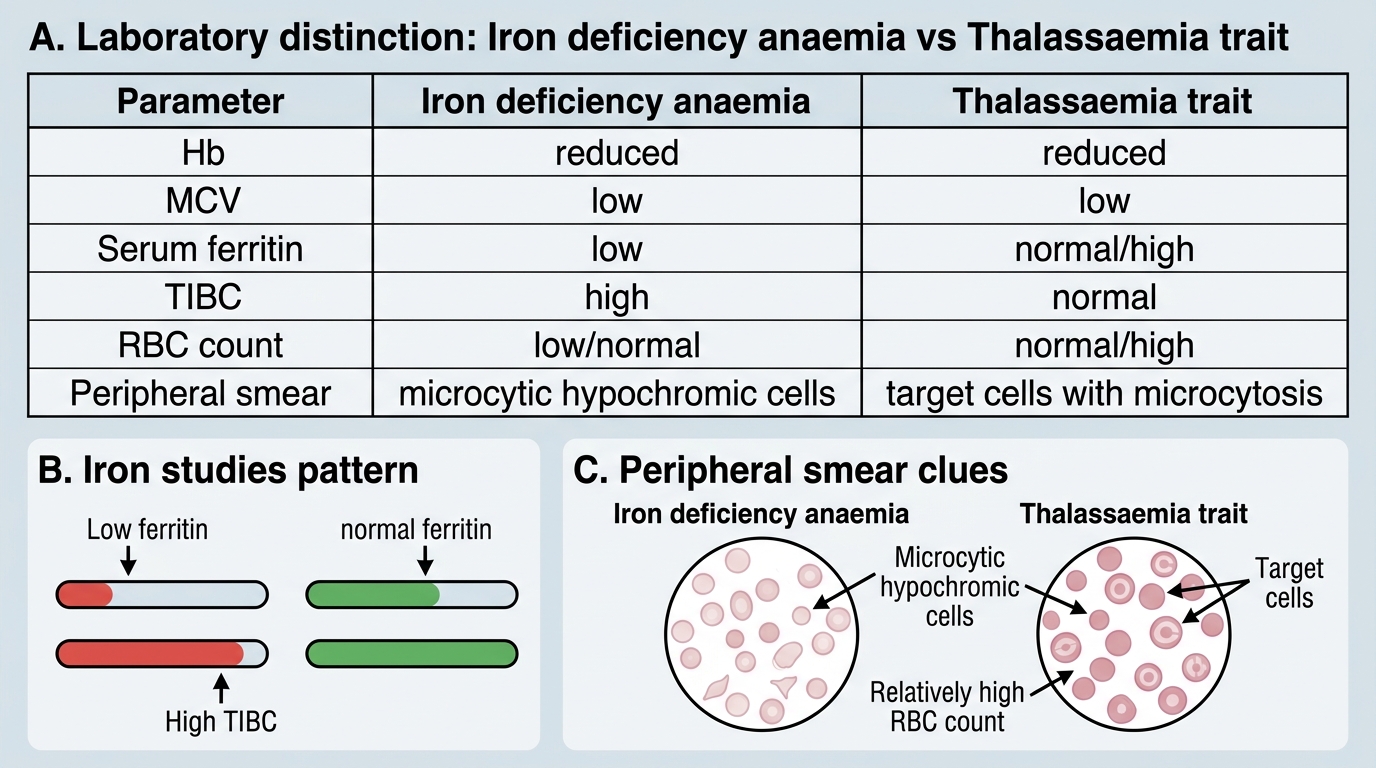
Iron Deficiency Anaemia vs Thalassaemia Trait