Page 1 of 33
PE12.1-2 | Vitamin A — SDL Guide
Learning Objectives
- State the recommended dietary allowance (RDA) and main dietary sources of Vitamin A for children
- Describe the absorption, transport and metabolism of Vitamin A (retinol and carotenoids)
- Explain the physiological functions of Vitamin A including vision, epithelial integrity and immune defence
- Classify Vitamin A deficiency using the WHO xerophthalmia grading (X0–XF, XN)
- Identify the clinical features at each stage of Vitamin A deficiency
- Describe the diagnosis, treatment schedule and preventive programme for Vitamin A deficiency
- Recognise the features of Vitamin A toxicity (acute and chronic)
INSTRUCTIONS
Vitamin A deficiency remains a major public health problem in India, responsible for the leading preventable cause of blindness in children under five. This module connects nutritional science to clinical practice: understanding how Vitamin A is absorbed, stored and utilised will equip you to recognise early deficiency (before corneal damage occurs), initiate the correct treatment schedule, and counsel families on prevention. India's National Prophylaxis Programme delivers supplementation at critical contact points with the health system, and every clinician must know the doses and timing. By the end of this module you will be able to stage xerophthalmia, prescribe the correct doses, and understand why Vitamin A supplementation reduces under-five mortality.
References
- Ghai Essential Pediatrics, 9th ed., Ch 9 (Vitamins and Minerals) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 62 (Vitamin A Deficiency) (textbook)
- WHO/UNICEF Vitamin A Supplementation: A Decade of Progress (2007) (guideline)
- Ministry of Health & Family Welfare, National Vitamin A Prophylaxis Programme Guidelines (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 2-year-old boy is brought by his mother to a rural health centre in Rajasthan. She has noticed that he bumps into objects in the evenings and refuses to walk outdoors after dusk. On examination he is thin, with dry skin. Inspection of his eyes reveals bilateral foamy, white triangular plaques on the temporal bulbar conjunctiva that do not wash off with irrigation. He received only the birth vaccines and the 9-month MR vaccine; his mother says the health worker who visited last time did not offer any 'eye drops or syrup.' What is the most likely diagnosis, and what single intervention could have prevented his eye disease?
WHY THIS MATTERS
Vitamin A deficiency is the world's most common cause of preventable blindness in children and significantly increases the risk of death from infections such as measles and diarrhoea. India accounts for a disproportionate share of the global burden — surveys estimate that subclinical deficiency affects 60–70% of pre-school children in some states. Critically, the spectrum runs from asymptomatic biochemical depletion through progressive eye disease to potentially fatal keratomalacia. Because the early stages (night blindness, conjunctival xerosis, Bitot's spots) are entirely reversible with supplementation, clinical recognition matters enormously. India's National Vitamin A Prophylaxis Programme delivers megadose supplementation at standard immunisation contacts, and as a final-year student you will be a frontline provider of this programme. This module also covers Vitamin A excess, which is clinically important because accidental overdose (especially in the context of well-intentioned supplementation) produces a distinct and serious syndrome.
RECALL
Before proceeding, activate your prior knowledge. From Physiology (Year 1), recall how fat-soluble vitamins (A, D, E, K) are absorbed — they require bile salts for emulsification and are packaged into chylomicrons for lymphatic transport, unlike water-soluble vitamins that enter the portal circulation directly. Vitamin A is a 20-carbon polyene alcohol (retinol); in the eye, it is isomerised to 11-cis retinal and incorporated into rhodopsin in rod photoreceptors — this is the biochemical basis of dark adaptation. From Biochemistry, recall that the liver is the principal storage organ for Vitamin A, and that release to peripheral tissues requires retinol-binding protein (RBP) complexed with transthyretin. These metabolic facts will make the clinical consequences of deficiency and the dose selection for treatment logically coherent rather than memorised.
Orientation: Vitamin A's Role in Paediatric Health
Vitamin A belongs to the family of fat-soluble vitamins and encompasses a group of structurally related compounds — retinol, retinal, and retinoic acid — as well as the dietary provitamin A carotenoids (principally β-carotene) from plant sources. Its clinical importance in paediatrics cannot be overstated: globally, an estimated 250 million pre-school-aged children are subclinically deficient, and each year approximately 250,000–500,000 children become blind due to Vitamin A deficiency, with half of those dying within twelve months of losing their sight. In India, the National Family Health Survey has repeatedly documented that rural, economically deprived children in states such as Rajasthan, Uttar Pradesh, Madhya Pradesh, and Odisha carry the highest burden.
Vitamin A deficiency does not merely affect the eyes. It compromises epithelial integrity throughout the body — respiratory, gastrointestinal, and urogenital tracts — resulting in increased susceptibility to infections, and it impairs immune function by reducing the production and activity of T lymphocytes and natural killer cells. Supplementation trials (IVACG, DEVTA, Beaton 1993 meta-analysis) have demonstrated a 23–24% reduction in all-cause under-five mortality with Vitamin A supplementation in deficiency-endemic settings. The interaction between Vitamin A deficiency and measles is particularly important: measles dramatically depletes hepatic Vitamin A stores and precipitates acute fulminant blindness (keratomalacia) in already-marginal children; consequently, the WHO and India's NIS mandate Vitamin A supplementation at the time of measles vaccination.
- Epidemiology in India: high-burden states = MP, UP, Rajasthan, Odisha
- Mortality impact: 23–24% reduction in under-5 mortality with supplementation
- Co-morbidity with measles: measles precipitates acute keratomalacia; supplement at measles visit
Vitamin A Absorption, Transport, Storage and Tissue Delivery
RDA, Dietary Sources and Metabolism
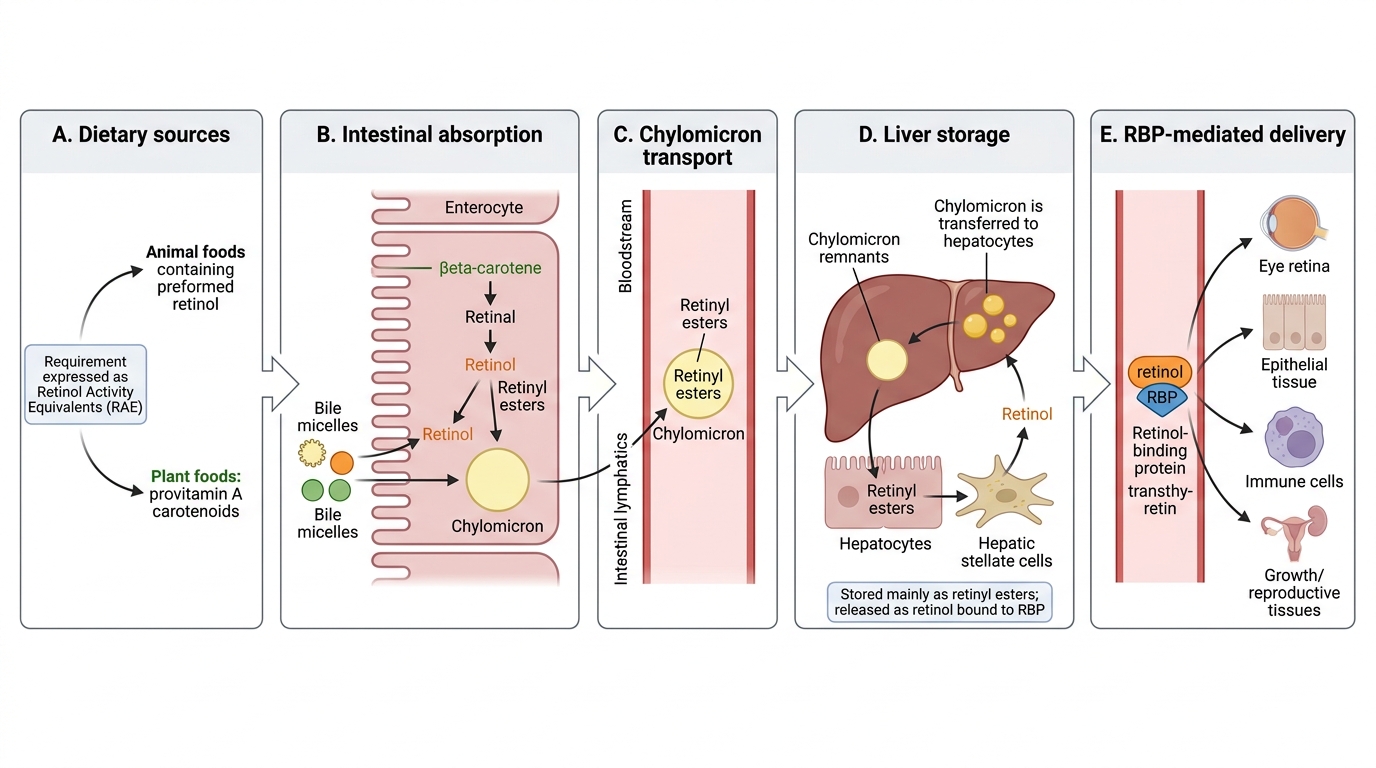
The dietary requirement for Vitamin A is expressed as Retinol Activity Equivalents (RAE) to account for the fact that provitamin A carotenoids are converted to retinol with lower efficiency than preformed retinol. The ICMR-recommended dietary allowance for children varies by age: approximately 400 mcg RAE/day for children aged 1–3 years, 600 mcg RAE/day for 4–6 years, and 600–700 mcg RAE/day for school-age children. Adult males require 600 mcg RAE/day and adult females 570 mcg RAE/day; requirements increase during pregnancy (800 mcg RAE/day) and lactation (950 mcg RAE/day).
Dietary sources are conventionally divided into two groups: preformed Vitamin A (retinol) in animal-origin foods — liver (the richest source, 10,000–15,000 mcg/100 g), egg yolk, dairy products (butter, ghee, whole milk), fish liver oils (cod-liver oil); and provitamin A carotenoids in plant foods — β-carotene (most efficiently converted) in dark-green leafy vegetables (spinach, drumstick leaves, methi), orange-yellow vegetables and fruits (carrots, sweet potato, mango, papaya), and red palm oil. Breast milk is an important source for infants when the mother is well-nourished; colostrum is particularly rich. In practice, Indian diets — especially in low-income and rural families — tend to be plant-based, making carotenoid conversion efficiency clinically significant.
Metabolism: dietary retinol esters and carotenoids are hydrolysed in the gut lumen; retinol is re-esterified as retinyl esters within enterocytes and packaged into chylomicrons for lymphatic absorption. In the liver, retinyl esters are stored in hepatic stellate cells (Ito cells), which hold 90% of the body's total Vitamin A (representing 6–12 months' reserve in a well-nourished individual). Mobilisation from the liver involves hydrolysis to retinol, binding to retinol-binding protein (RBP), and transport in complex with transthyretin (TTR) in the serum. Carotenoids are converted to retinal (and then retinol) in the intestinal mucosa; the conversion ratio for β-carotene to retinol is approximately 12:1 (dietary weight), hence 12 µg of β-carotene = 1 µg RAE.
| Source Category | Examples | RAE content (approx.) |
|---|---|---|
| Animal (preformed) | Liver | Very high (10,000+ mcg/100 g) |
| Animal (preformed) | Egg yolk, ghee, whole milk | Moderate |
| Plant (carotenoid) | Dark green leaves (palak, methi, drumstick) | High (as β-carotene) |
| Plant (carotenoid) | Orange-yellow fruits/vegetables (carrot, mango, papaya) | Moderate–high |
| Infant source | Breast milk (well-nourished mother) | Sufficient if maternal stores adequate |
Mechanism of Action and Functions of Vitamin A
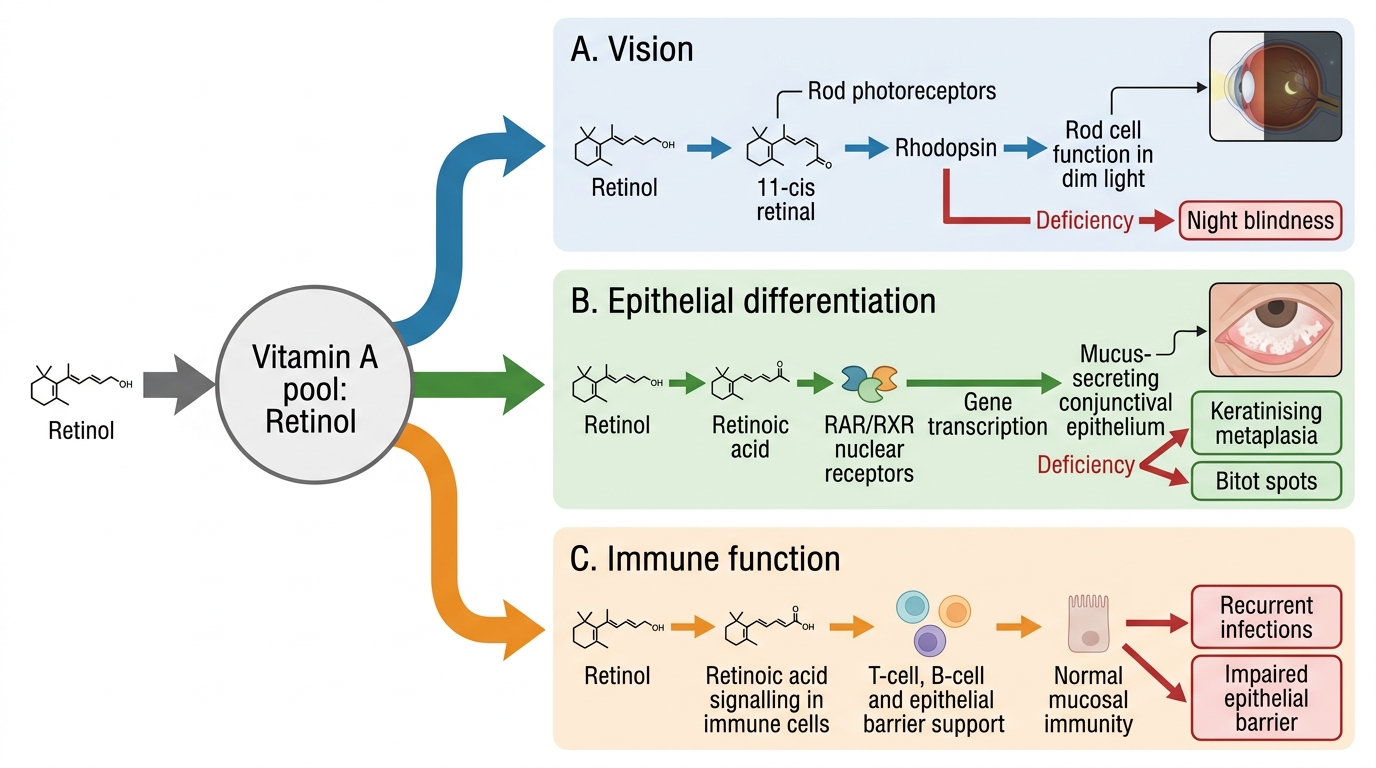
Vitamin A exerts its physiological effects through several mechanisms depending on the active form — retinal, retinol, or retinoic acid. Each form has a distinct role, and understanding these mechanistic linkages makes the clinical deficiency syndrome logically deducible rather than a list to be memorised.
Vision: In rod photoreceptors, retinol is transported to the retina and oxidised to 11-cis retinal, which combines with the protein opsin to form rhodopsin (visual purple). When light strikes the retina, rhodopsin is bleached (11-cis retinal → all-trans retinal + opsin), generating a nerve impulse that signals the brain. Dark adaptation (the ability to see in low-light conditions) requires the continuous regeneration of rhodopsin, which depends on an adequate supply of retinol from the circulation. Depletion of Vitamin A → insufficient 11-cis retinal → impaired rhodopsin regeneration → night blindness (nyctalopia), the earliest clinical sign.
Epithelial differentiation: Retinoic acid binds to nuclear retinoic acid receptors (RAR/RXR), which regulate the transcription of genes controlling cell differentiation. Vitamin A maintains mucus-secreting columnar epithelium throughout the body; deficiency leads to replacement of normal mucus-secreting epithelium by keratinising squamous epithelium (xerosis, metaplasia) — seen on the conjunctiva (conjunctival xerosis, Bitot's spots), cornea (corneal xerosis, keratomalacia), skin (phrynoderma), respiratory tract, and gut.
Immune function: Vitamin A supports both innate and adaptive immunity. It is required for the normal function of natural killer (NK) cells, T-lymphocyte differentiation (including T-regulatory cells), and production of secretory IgA at mucosal surfaces. Deficiency impairs the first-line mucosal defence and increases susceptibility to bacterial and viral infections, explaining the striking mortality reduction seen with supplementation in measles and diarrhoeal disease.
Summary of functions:
• Rhodopsin synthesis → dark adaptation
• Epithelial differentiation → mucosal barrier integrity (respiratory, GI, urogenital, conjunctival)
• Immune function → NK cell activity, T-cell differentiation, mucosal IgA
Vitamin A Functions and Deficiency Consequences
SELF-CHECK
A 3-year-old child cannot see well at dusk but has normal visual acuity in daylight. Slit-lamp examination shows bilateral foamy white plaques on the temporal bulbar conjunctiva. Which TWO Vitamin A metabolic steps are most directly disrupted in this child?
A. Conversion of 11-cis retinal to rhodopsin in rod cells, AND differentiation of mucus-secreting conjunctival epithelium
B. Conversion of retinol to retinoic acid in the liver, AND production of coagulation factors
C. Absorption of carotenoids by enterocytes, AND transport of retinol by chylomicrons only
D. Synthesis of retinol-binding protein by hepatic stellate cells, AND cholesterol metabolism
Reveal Answer
Answer: A. Conversion of 11-cis retinal to rhodopsin in rod cells, AND differentiation of mucus-secreting conjunctival epithelium
Night blindness reflects impaired rhodopsin regeneration (insufficient 11-cis retinal from retinol depletion). Bitot's spots represent keratinising metaplasia of conjunctival epithelium due to loss of retinoic acid's epithelial-differentiation function. These are the earliest visual (X0) and conjunctival (X1A) manifestations respectively. Coagulation factor synthesis relates to Vitamin K (not A). Chylomicron transport is needed but is not what is 'disrupted' clinically here.