Page 10 of 33
PE12.5-6 | Vitamin K — SDL Guide
Learning Objectives
- State the RDA and dietary sources of Vitamin K (K1 and K2) for infants and children
- Explain the mechanism by which Vitamin K enables coagulation factor activation (gamma-carboxylation)
- List the Vitamin K-dependent coagulation factors and explain the significance for coagulation testing
- Classify Vitamin K Deficiency Bleeding (VKDB) into early, classic, and late forms with their timing, causes, and at-risk groups
- Describe the clinical features of each form of VKDB, emphasising the danger of late VKDB intracranial haemorrhage
- Interpret the coagulation profile in VKDB and distinguish it from other bleeding disorders
- Describe the treatment of VKDB and the prophylaxis protocol at birth
INSTRUCTIONS
Vitamin K Deficiency Bleeding (VKDB) — formerly called Haemorrhagic Disease of the Newborn — is entirely preventable with a single intramuscular injection of Vitamin K at birth. Yet it continues to cause preventable deaths and permanent neurological disability from intracranial haemorrhage when prophylaxis is missed. This module covers the biological role of Vitamin K in coagulation, the three clinical forms of VKDB, and the critical national guideline on prophylaxis. Understanding why exclusively breastfed infants are at highest risk, and why late VKDB is so dangerous, will equip you to advocate for routine prophylaxis and to diagnose VKDB rapidly when it does occur.
References
- Ghai Essential Pediatrics, 9th ed., Ch 9 (Vitamins and Minerals — Vitamin K) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 65 (Vitamin K Deficiency) (textbook)
- IAP Guideline on Vitamin K Prophylaxis in Newborns (2014) (guideline)
- Cloherty and Stark's Manual of Neonatal Care, 8th ed. (Neonatal Coagulopathy) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 3-week-old exclusively breastfed infant is brought to the emergency department by her parents. She was born at home and weighed 3.2 kg at birth. No postnatal medications were given at home. For 2 days the parents have noticed the infant was increasingly lethargic and not feeding well. Today she had one episode of vomiting followed by a tense fontanelle. CT scan of the head is performed and reveals a large intracranial haemorrhage. Coagulation tests show: PT 45 seconds (normal <15), aPTT 98 seconds (normal <40), platelet count 280 × 10⁹/L (normal). What single injection given at birth could have completely prevented this catastrophe?
WHY THIS MATTERS
Vitamin K Deficiency Bleeding is the most important preventable cause of intracranial haemorrhage in neonates. Unlike most paediatric emergencies, it has a single, cheap, and universally applicable intervention: 1 mg of Vitamin K intramuscularly at birth. The tragedy of VKDB lies in its preventability — in countries with high rates of home delivery and inconsistent prophylaxis coverage, late VKDB causing intracranial haemorrhage continues to be seen. The mortality is 20% and permanent neurological disability occurs in 30–50% of survivors of intracranial VKDB. Beyond the newborn period, Vitamin K continues to play an essential role in maintaining haemostasis throughout life; understanding its mechanism illuminates the pharmacology of warfarin and the management of coagulopathy. This module also grounds your understanding of the coagulation cascade by identifying which factors depend on Vitamin K — knowledge that directly applies to interpretation of coagulation tests in clinical practice.
RECALL
Activate your knowledge of the coagulation cascade from Physiology. Recall that haemostasis involves both primary (platelet plug formation) and secondary (coagulation factor cascade) phases. The coagulation cascade has two initiation pathways converging on a common pathway: the extrinsic pathway (Tissue Factor + Factor VII → activates X) is measured by the prothrombin time (PT); the intrinsic pathway (Factors XII → XI → IX → VIII → X) is measured by the activated partial thromboplastin time (aPTT). The common pathway (Factors X → V → II [prothrombin → thrombin] → I [fibrinogen → fibrin]) is measured by both PT and aPTT. Critically, recall that platelet count and bleeding time (primary haemostasis) are normal in pure coagulation factor deficiency — a key point for distinguishing VKDB from thrombocytopenia. Vitamin K deficiency impairs secondary haemostasis (factor carboxylation), not platelet function.
Orientation: Vitamin K's Role in Haemostasis
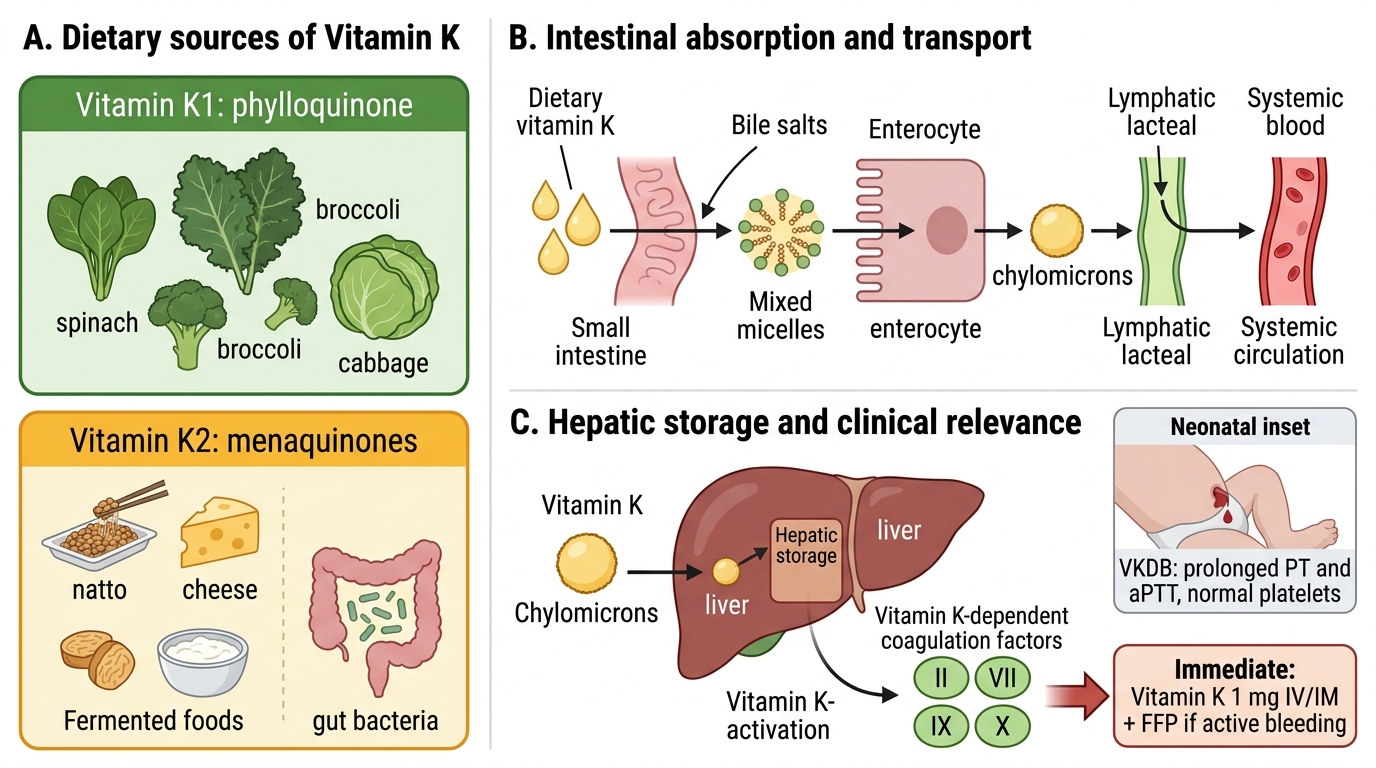
Vitamin K is a fat-soluble vitamin whose name derives from the German word Koagulationsvitamin — 'coagulation vitamin' — reflecting its essential role in blood clotting, which was its first discovered function. It exists in three naturally relevant forms: Vitamin K1 (phylloquinone), the principal dietary form found in green leafy vegetables; Vitamin K2 (menaquinones, MK-4 to MK-13), produced by intestinal bacteria and present in fermented foods (nattokinase, cheese); and Vitamin K3 (menadione), the synthetic water-soluble form used pharmaceutically. Of these, K1 and K2 are clinically significant for nutrition and supplementation.
Vitamin K's central role in paediatrics is the prevention of Vitamin K Deficiency Bleeding (VKDB) — a condition unique to the newborn period, and particularly dangerous in its late form, which causes intracranial haemorrhage in otherwise healthy breastfed infants. The reason newborns are specifically vulnerable is a combination of four factors: (1) placental transfer of Vitamin K is poor; (2) breast milk contains very little Vitamin K (1–3 mcg/L, compared to 4–25 mcg/100 kcal in formula); (3) the neonatal gut is initially sterile, providing no bacterial K2 synthesis; (4) hepatic stores at birth are minimal. This makes every newborn physiologically Vitamin K-deficient at birth, with exclusively breastfed infants at greatest risk if prophylaxis is not given.
Beyond the neonatal period, Vitamin K is required throughout life for maintaining adequate coagulation factor activity, and its antagonism by warfarin is the basis of anticoagulant therapy.
RDA, Dietary Sources and Metabolism of Vitamin K
The recommended dietary intake of Vitamin K is relatively modest compared to other fat-soluble vitamins, reflecting the contribution of bacterial synthesis to the body's Vitamin K economy. The ICMR-recommended intake is approximately 10–20 mcg/day for infants (0–12 months) and 30–55 mcg/day for children aged 1–10 years; adults require 55–65 mcg/day. These values represent the dietary K1 requirement, recognising that gut bacterial K2 provides an additional but variable contribution depending on the intestinal microbiome. Two nutritional facts about Vitamin K are clinically pivotal: first, dark-green leafy vegetables are so rich in K1 that a single serving can satisfy the daily requirement many times over — so dietary deficiency in older children eating a balanced diet is essentially non-existent; second, breast milk is strikingly low in Vitamin K (~1–3 mcg/L), which is the biological basis for neonatal VKDB risk and explains why infant formula is routinely supplemented.
Dietary sources of Vitamin K:
• K1 (phylloquinone) — highest in: dark-green leafy vegetables (spinach, kale, methi, palak, coriander, broccoli); also in vegetable oils (soybean, canola), Brussels sprouts. Green leafy vegetables can contain 100–900 mcg/100 g — far exceeding daily requirements with a single serving.
• K2 (menaquinones) — found in: fermented soy (natto — the richest K2 source at 900+ mcg/100 g), some cheeses, eggs, meat; and synthesised by Bacteroides, Fusobacterium and other gut anaerobes.
• Breast milk: very low in Vitamin K (~1–3 mcg/L); this is the key nutritional fact underlying neonatal VKDB risk. Formula milk is supplemented to ~4–25 mcg/100 kcal.
Absorption and metabolism follow the fat-soluble vitamin route: Vitamin K requires bile salts for micellar solubilisation, is absorbed via enterocytes, packaged into chylomicrons (K1 predominantly) or via portal circulation (K2), and stored in the liver. Hepatic stores are limited (1–2 weeks' supply in adults), which means Vitamin K deficiency can develop quickly with malabsorption or antibiotic-related suppression of gut flora.
Vitamin K Sources, Absorption, and Hepatic Role
SELF-CHECK
A 4-day-old exclusively breastfed term infant (3.3 kg, born at a government hospital) presents with oozing from the umbilical stump and a large cephalhaematoma. Investigation: PT 52 s (elevated), aPTT 105 s (elevated), platelet count 240 × 10⁹/L (normal), bleeding time 3 min (normal). Which intervention should be administered immediately?
A. Intravenous Vitamin K 1 mg and fresh frozen plasma for active bleeding
B. Platelet transfusion for thrombocytopenia
C. Fresh frozen plasma alone without Vitamin K
D. IM Vitamin K 10 mg as a single high-dose treatment
Reveal Answer
Answer: A. Intravenous Vitamin K 1 mg and fresh frozen plasma for active bleeding
Prolonged PT and aPTT with normal platelets and normal bleeding time is the hallmark of Vitamin K deficiency bleeding (classic VKDB, day 2-7). The pattern reflects deficiency of K-dependent coagulation factors (II, VII, IX, X) with intact primary haemostasis. Immediate management is IV or IM Vitamin K 1 mg, which restores coagulation factor carboxylation. Fresh frozen plasma (FFP) is added when there is active, significant bleeding requiring rapid factor replacement because Vitamin K takes several hours to work. Platelet transfusion is incorrect — platelets are normal. A 10 mg dose is excessive and not recommended.
Mechanism: Vitamin K-Dependent Coagulation Factor Carboxylation
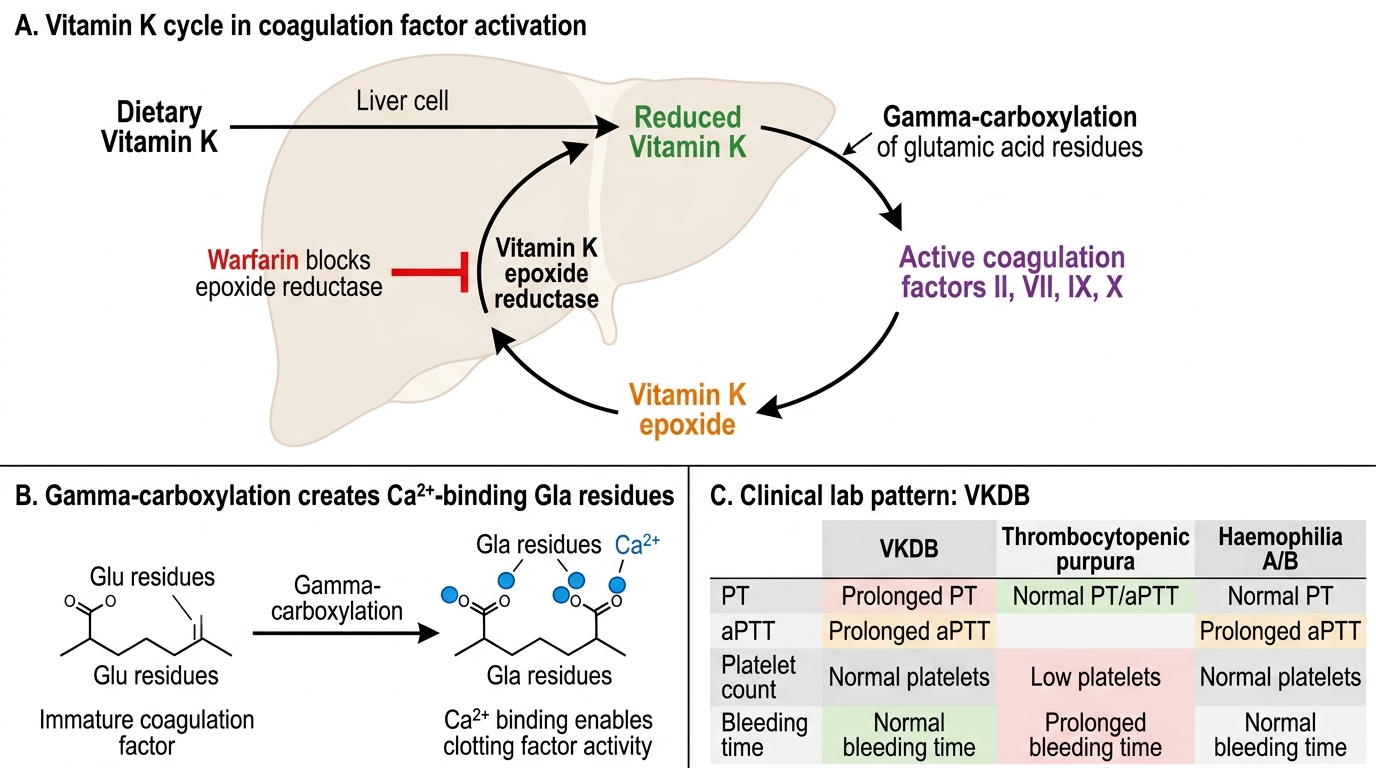
Vitamin K serves as an essential cofactor for the enzyme gamma-glutamyl carboxylase in hepatocytes. This enzyme adds a carboxyl group (COO⁻) to specific glutamic acid (Glu) residues on the precursor forms of coagulation proteins, converting them to gamma-carboxyglutamic acid (Gla) residues. This carboxylation step is not optional — it is biochemically essential for the protein to function, because the Gla residues provide negatively charged binding sites that chelate calcium ions (Ca²⁺), enabling the coagulation protein to anchor to phospholipid membrane surfaces and participate in the coagulation cascade. Without gamma-carboxylation, the coagulation factors are produced but remain biologically inert (called PIVKAs — Proteins Induced by Vitamin K Absence).
The Vitamin K cycle: During each carboxylation reaction, Vitamin K is oxidised to Vitamin K epoxide (the inactive form). The enzyme Vitamin K epoxide reductase (VKOR) then reduces Vitamin K epoxide back to active Vitamin K (the reduced quinol form), recycling it for the next carboxylation round. This cycle is the target of warfarin — warfarin inhibits VKOR, trapping Vitamin K in the epoxide form and preventing its recycling, thereby depleting active Vitamin K and impairing coagulation factor carboxylation.
Vitamin K-dependent coagulation factors:
• Procoagulant factors: Factor II (prothrombin), Factor VII, Factor IX, Factor X
• Anticoagulant proteins: Protein C, Protein S
Note: all four procoagulant factors are in the common or extrinsic/intrinsic pathways, explaining why Vitamin K deficiency prolongs BOTH the PT (extrinsic: Factor VII + X + II) AND the aPTT (intrinsic: Factor IX + X + II). In contrast, primary haemostasis (platelet count, bleeding time) is entirely normal.
- Vitamin K also carboxylates osteocalcin (bone matrix protein) and matrix Gla protein — roles in bone mineralisation and arterial calcification prevention.
Vitamin K Cycle and VKDB Lab Pattern
CLINICAL PEARL
The coagulation profile of VKDB is pathognomonic: prolonged PT AND prolonged aPTT WITH normal platelet count and normal bleeding time. This pattern is distinct from thrombocytopenic purpura (low platelets + prolonged bleeding time + normal PT/aPTT) and from haemophilia A/B (only aPTT prolonged, not PT). When a newborn presents with unexplained bleeding and this laboratory pattern, VKDB must be the first diagnosis considered, and Vitamin K should be given immediately without waiting for further test results.