Page 6 of 20
PE16.{2,5} | IMNCI Young Infant Assessment — SDL Guide (Part 2)
Classifying the Young Infant: PSBI, Local Infection, Jaundice, Feeding Problems
After completing the eleven-step young-infant assessment, each domain of findings is translated into a classification using the IMNCI colour-coded triage system: pink for urgent referral, yellow for facility-level treatment, and green for home management with counselling. The classification is not a summary of all findings — it is a decision rule that takes the MOST SEVERE finding and drives the action. This is the override rule: if ANY single pink classification is found at any point during the assessment, the child is managed as pink regardless of how many yellow or green findings were also recorded. Understanding the criteria for each classification — and why they are set at specific thresholds — is essential for applying the algorithm correctly under clinical pressure. The following classification system covers all the major conditions assessed in the young-infant algorithm, with emphasis on the pink conditions that require immediate pre-referral treatment before transfer.
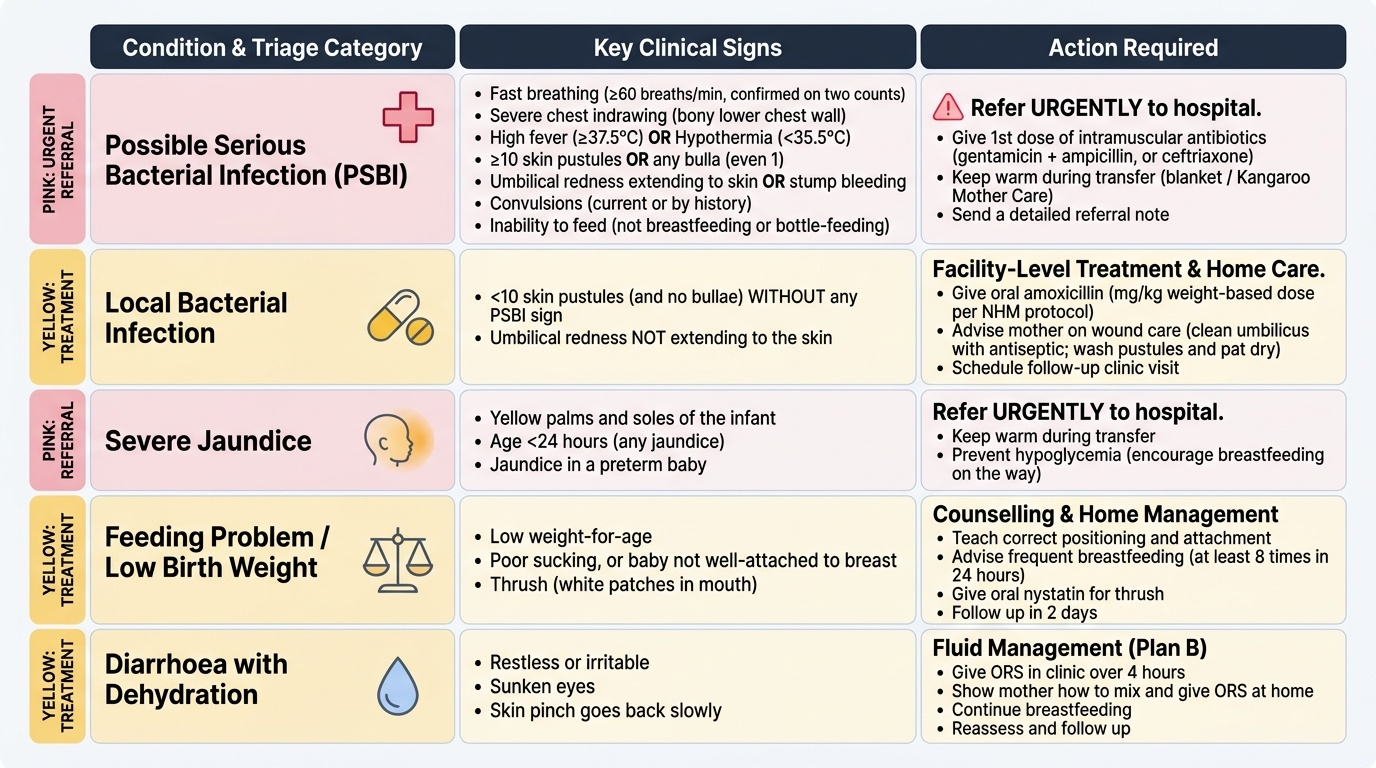
Provided image
1. Possible Serious Bacterial Infection (PSBI) — PINK:
Presence of ANY ONE of the following:
• Fast breathing (≥60/min, confirmed on two counts)
• Severe chest indrawing (bony thorax — lower chest wall)
• Temperature ≥37.5°C (fever) OR <35.5°C (hypothermia)
• ≥10 skin pustules OR any bulla (even 1)
• Umbilical redness extending to skin
• Bleeding from stump (bleeding from umbilical cord stump is a PSBI sign)
• Convulsions (current or by history in this illness)
• Cannot feed at all (not breastfeeding or bottle-feeding)
Action: Refer URGENTLY to hospital. Give pre-referral treatment: first dose of IM antibiotic (gentamicin + ampicillin per current NHM protocol, OR ceftriaxone if a single-antibiotic protocol is used at your facility); if baby cannot be transferred, initiate IV fluids. Keep warm during transfer (wrap in blanket; kangaroo care if possible). Give a referral note with all findings and the pre-referral treatment given.
2. Local Bacterial Infection — YELLOW:
Skin pustules <10 (and no bulla) WITHOUT any other PSBI sign, OR umbilical redness NOT extending to skin.
Action: Give oral amoxicillin (specific mg/kg weight-based dosing per current NHM protocol — do NOT give adult doses). Advise mother on wound care (umbilicus: clean with antiseptic; pustules: gently wash and pat dry). Return for follow-up in 2 days. Advise on danger signs requiring immediate return.
3. Severe Jaundice — PINK:
Jaundice visible on palms OR soles (regardless of age), OR jaundice appearing within 24 hours of birth.
Action: Refer URGENTLY. Severe jaundice in the first 24 hours is haemolytic (Rh/ABO incompatibility) until proven otherwise — bilirubin rises rapidly and untreated hyperbilirubinaemia causes kernicterus (permanent brain damage). Pre-referral: keep baby warm and feeding; do NOT delay transfer.
4. Jaundice (moderate) — YELLOW:
Jaundice present but NOT on palms/soles and NOT within 24 hours.
Action: Advise increased breastfeeding (every 2–3 hours). Follow up in 1 day. If jaundice extending or no improvement, refer.
5. Feeding Problem or Low Birth Weight — YELLOW (or PINK if severe):
Unable to feed adequately, or low birth weight <2500 g without PSBI signs.
Action for feeding problem: advise on breastfeeding technique; supplement expressed breastmilk by cup/spoon if latch fails; if baby takes <3/4 of expected feeds, refer.
Action for LBW: if weight ≥1800 g and feeding well and no other problem → advise skin-to-skin (kangaroo care) and frequent breastfeeding, follow up in 2 days; if weight <1800 g or LBW + any PSBI sign → refer URGENTLY (PINK).
6. Diarrhoea — classify dehydration separately:
In young infants, diarrhoea dehydration is classified as no dehydration, some dehydration, or severe dehydration (same signs as older children but the threshold for referral is lower). Severe dehydration in a young infant = PINK (refer). Some dehydration = give ORS, advise on feeding, follow up.
| Classification | Colour | Key signs | Action |
|---|---|---|---|
| PSBI | Pink | Any 1 of 8 signs | Urgent referral + IM antibiotic |
| Local bacterial infection | Yellow | Pustules <10 or local umbilical redness | Oral amoxicillin + follow-up |
| Severe jaundice | Pink | Palms/soles or <24h onset | Urgent referral |
| Moderate jaundice | Yellow | Present but not severe | Increased breastfeeding, follow-up |
| LBW <1800 g | Pink | Weight + feeding difficulties | Urgent referral |
| LBW 1800-2499 g | Yellow | Weight only, feeding ok | Kangaroo care, follow-up |
Risk Stratification in the Sick Neonate
Risk stratification in the IMNCI context means using the classification output to determine the level of urgency and the level of care the sick neonate requires. The IMNCI algorithm performs this stratification through its colour-coded system, but understanding the underlying risk logic helps practitioners apply the algorithm correctly when findings are ambiguous or borderline. Neonates are biologically unique in that their compensatory reserve is small — a young infant with neonatal sepsis may maintain a near-normal blood pressure until cardiovascular collapse is imminent, so vital-sign thresholds that signal moderate risk in an older child represent high risk in a neonate. This asymmetry — where a finding that looks mild is actually serious — is the reason IMNCI calibrates its pink-classification criteria conservatively (low threshold for referral) in the young infant. A practitioner who understands the underlying physiology will naturally err toward referral when signs are ambiguous, rather than waiting for full-blown septic shock to develop. The following risk tiers describe the clinical reasoning behind the triage categories.
High-risk features that mandate urgent referral (Pink) regardless of other findings:
• Any PSBI sign — because PSBI in a young infant has case fatality rates of 10–30% even with optimal facility care; delays of even 2–4 hours increase mortality substantially.
• Severe jaundice — because bilirubin in the kernicteric range can cause permanent brain damage within hours; there is no safe observation period at primary care level.
• LBW <1800 g — because these infants have insufficient glycogen reserves, immature temperature control, and limited respiratory reserve to sustain themselves without intensive nursing support.
• Any PSBI sign + diarrhoea — compound risk; the combination of sepsis and dehydration causes rapid cardiovascular compromise.
Moderate-risk features requiring facility-level management (Yellow):
• Local bacterial infection without systemic spread — responds to oral antibiotics but requires verification of compliance at 48-hour follow-up.
• Moderate jaundice — has a defined safe observation window with breastfeeding support, but requires next-day reassessment.
• LBW 1800–2499 g without other problems — can be managed with kangaroo mother care (KMC) and exclusive breastfeeding support at PHC level, with twice-weekly weight monitoring.
Perinatal risk factors that elevate the prior probability of PSBI (elicit in history):
• Maternal fever ≥38°C before or during delivery
• Prolonged rupture of membranes (PROM) >18 hours
• Foul-smelling liquor
• Maternal Group B Streptococcus (GBS) colonisation (if known)
• Birth asphyxia or resuscitation at birth
• Preterm birth (<37 weeks)
When ANY perinatal risk factor is present, the threshold for classification as PSBI and referral should be lower — a neonate with maternal fever + fast breathing (even borderline 58–62/min on repeated count) should be classified PSBI and referred.
Important rule: do not discharge a sick-looking neonate with only one negative finding. The algorithm is designed so that any ONE positive sign triggers PSBI. However, when a neonate looks sick (lethargic, pale, poor tone) but the specific signs are just below threshold, use clinical judgment to classify upward — the algorithm is a minimum standard, not a ceiling.
CLINICAL PEARL
Jaundice on palms and soles = Pink, no exceptions. A common mistake is to reassure a mother whose 8-day-old baby has mild jaundice with the phrase 'it's still physiological — come back in 2 days'. This is correct ONLY if the jaundice does not extend to palms or soles. If the palms or soles are yellow on blanching, the baby MUST be referred regardless of day of life, feeding status, or absence of other symptoms. Bilirubin at the palms/soles level corresponds to serum bilirubin typically above 15–17 mg/dL in term neonates — within the range of neurotoxicity. The visual zone-of-spread (Kramer's zones) is a practical bedside tool: Zone 1 = face, Zone 2 = chest, Zone 3 = below umbilicus, Zone 4 = below knees/elbows, Zone 5 = palms/soles. Zone 5 = refer.
SELF-CHECK
A 10-day-old baby has 7 skin pustules on the trunk, no other signs, temperature 37.2°C, respiratory rate 54/min on two counts, feeding adequately, no jaundice. What is the IMNCI classification and action?
A. Pink — refer urgently with pre-referral IM antibiotic because pustules are present
B. Yellow — local bacterial infection; give oral amoxicillin and advise follow-up in 2 days
C. Green — fewer than 10 pustules with normal vitals means no action required; reassure and discharge
D. Yellow — give topical antibiotic only; systemic antibiotics are not needed for pustules
Reveal Answer
Answer: B. Yellow — local bacterial infection; give oral amoxicillin and advise follow-up in 2 days
This baby has 7 pustules (<10), no bulla, temperature 37.2°C (no fever), respiratory rate 54/min (<60/min — not fast breathing), and no other PSBI signs. This meets the criteria for LOCAL BACTERIAL INFECTION — classified YELLOW. The action is oral amoxicillin (weight-based dose per NHM protocol) plus wound care counselling, with follow-up in 2 days. PSBI requires ≥10 pustules or at least one other PSBI sign — this baby has neither. Green is wrong because local bacterial infection requires treatment. Topical antibiotic alone is insufficient — oral antibiotics are mandated by IMNCI for local bacterial infection.
Applied Practice: Supervised Assessment Scenarios
Applied practice in IMNCI young-infant assessment involves working through structured clinical scenarios and, ideally, supervised assessment in a neonatal ward or PHC outpatient setting. The following worked scenarios consolidate the assessment and classification steps.
Scenario A — 5-day-old male, home delivery:
History: mother says baby has not fed since morning (approximately 12 hours). Grandmother says baby has been 'sleeping too much'. No convulsions reported.
Observation: baby lies still, minimal spontaneous movement. Chest: respiratory rate 66/min (confirmed on second count). Severe chest indrawing present. Axillary temperature: 38.4°C. Umbilicus: slight redness confined to umbilical area. No skin pustules. Jaundice: visible on face and chest but not palms/soles. Weight: 2.7 kg (birthweight was 2.8 kg — has lost 100 g, acceptable if feeding resumes).
Classification: PSBI (PINK) — three PSBI signs present: fast breathing ≥60/min, fever ≥37.5°C, cannot feed (approximately). Plus: severe chest indrawing confirms PSBI independently.
Pre-referral action: give first dose IM antibiotic (gentamicin + ampicillin); keep warm; counsel mother on urgency; write referral note with all findings. Do NOT attempt oral antibiotics.
Scenario B — 18-day-old female, institutional delivery:
History: mother says baby is feeding well, 8–10 times per day. No fever noticed. Reason for visit: child welfare check at sub-centre.
Observation: baby active, crying appropriately. Respiratory rate 48/min (two counts). No chest indrawing. Axillary temperature: 36.8°C. Umbilicus: clean, no redness. Skin: 2 small pustules on left axilla, no bulla. Jaundice: slight yellow tinge on face; blanching shows no yellow on chest or below. Palms/soles: not yellow. Weight: 3.2 kg (birthweight was 2.9 kg — good weight gain). BCG scar visible; immunisation card shows Hep-B and OPV-0 given at birth.
Classification: Local bacterial infection (YELLOW) — 2 pustules without other PSBI signs. Jaundice is mild face-only (Zone 1) — classify as physiological, advise frequent breastfeeding, review tomorrow.
Action: oral amoxicillin; advise pustule wound care; advise on jaundice monitoring (return if jaundice spreads or baby feeds less); follow-up in 2 days.
Scenario C — 3-day-old female born at home:
History: mother says baby is 'yellow since yesterday morning' (approximately 24–36 hours old). Feeding 4–5 times per day, adequate latch.
Observation: significant yellow colouration of face, chest, abdomen, and palms. Palms clearly yellow on blanching. Respiratory rate 52/min. Axillary temperature 36.9°C. No skin lesions. Umbilicus clean.
Classification: Severe jaundice (PINK) — palms are yellow regardless of other findings.
Action: Urgent referral. Pre-referral: continue breastfeeding during transport; keep warm; referral note states onset at day 1–2, palms/soles yellow, vitals documented.
Counselling key points for all yellow cases: educate mothers on (1) danger signs requiring immediate return (baby stops feeding, breathing becomes difficult, temperature rises/falls, jaundice spreads to palms/soles, baby has a fit); (2) how to give oral medication correctly; (3) importance of follow-up appointment.
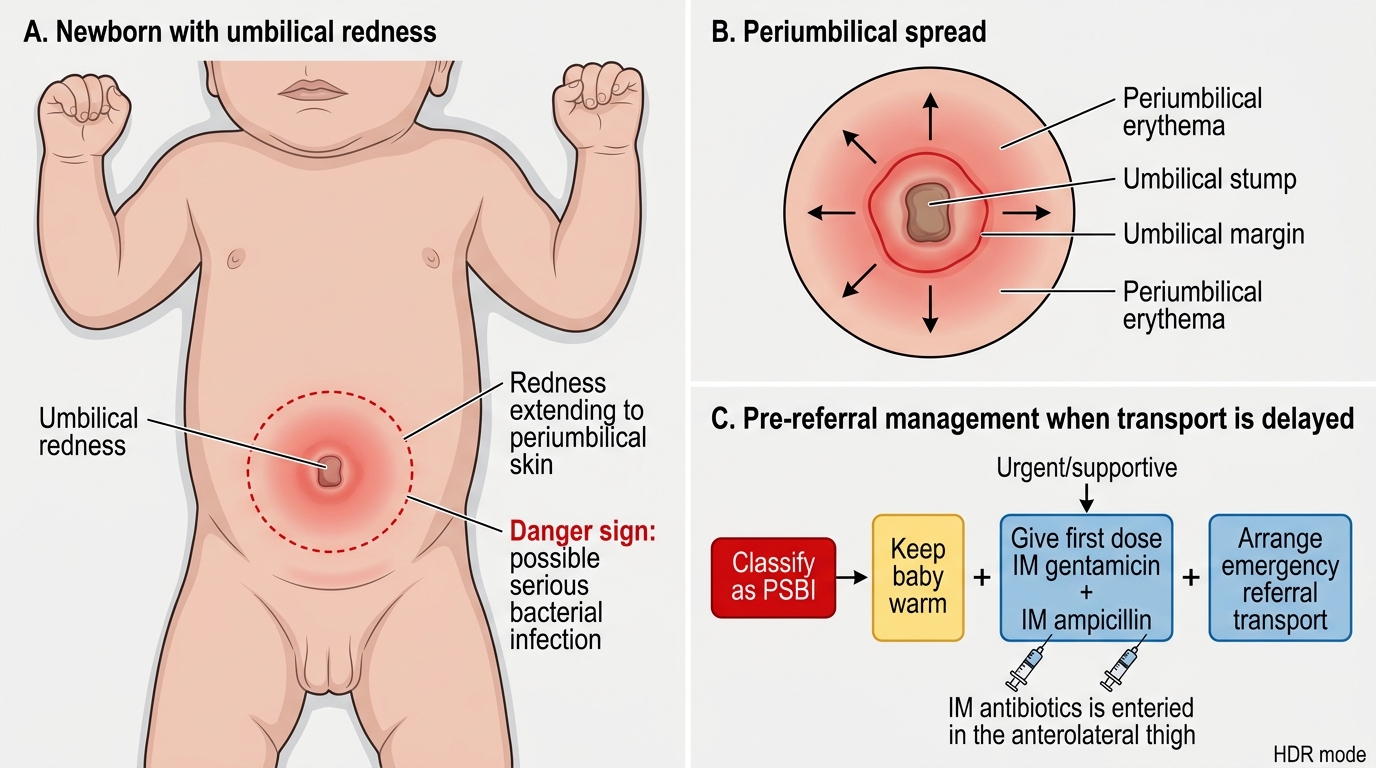
Umbilical Redness in Newborn: PSBI Danger Sign and Pre-referral Care
SELF-CHECK
A 25-day-old neonate classified as PSBI at a sub-centre does not have transport available for referral. You have gentamicin and ampicillin available. What is the most appropriate pre-referral management while arranging transport?
A. Give oral amoxicillin and wait for transport — IV/IM antibiotics are not appropriate without a hospital
B. Give first dose of IM gentamicin and IM ampicillin immediately; keep warm; arrange emergency transport as soon as possible
C. Give IM gentamicin only — ampicillin is not part of the IMNCI protocol
D. Delay antibiotic until the baby reaches the referral hospital to avoid interfering with blood culture
Reveal Answer
Answer: B. Give first dose of IM gentamicin and IM ampicillin immediately; keep warm; arrange emergency transport as soon as possible
IMNCI explicitly mandates PRE-REFERRAL administration of the first dose of IM antibiotics in PSBI — the rationale is that the mortality benefit of early antibiotics outweighs the risk of an imperfect setting for administration. The recommended regimen for PSBI pre-referral in India is gentamicin + ampicillin IM (single doses). Delaying antibiotics until arrival at the referral hospital substantially worsens outcome. Oral amoxicillin alone is not sufficient for PSBI. Gentamicin alone lacks coverage for Group B Streptococcus and Listeria (covered by ampicillin). Blood culture logistics never override time-sensitive antibiotic initiation in neonatal sepsis.
Self-Assessment
The following questions are designed to consolidate your application of the IMNCI young-infant assessment skill. For each vignette question, work through the full assessment sequence mentally — do not skip directly to the classification. Practising the sequence even on paper builds the procedural memory that will serve you in a real clinical encounter where time pressure and caregiver anxiety compete for your attention. These questions are structured at the NMC exit OSPE level — the standard you will be tested to before you practice independently. Competency PE16.2 requires you to assess children under 2 months using IMNCI guidelines, and PE16.5 requires you to identify and stratify risk in a sick neonate — both are demonstrated skills (domain S, level SH), meaning written knowledge alone is insufficient. Use these questions to test whether you can apply the algorithm fluidly, not just recall its components in isolation. Where possible, discuss your answers with a peer or faculty before reviewing the model responses, as the discussion process itself deepens procedural retention more effectively than passive re-reading.
- A 14-day-old infant has a respiratory rate of 62/min on a single 30-second count. Before classifying, what additional step does IMNCI mandate, and why is this important in young infants specifically?
- A mother brings her 20-day-old for a routine HBNC visit. The ASHA finds the baby feeding less than usual but no other signs. What IMNCI classification does this receive and what action is taken?
- List ALL eight PSBI signs in the IMNCI young-infant algorithm. Identify which two are temperature-based and which one relates to umbilical examination.
- A 7-day-old neonate has mild jaundice on the face only, first noticed by parents at day 4. No other abnormalities. What is the IMNCI classification, and what feeding advice is given?
- Compare the pre-referral management of a PSBI neonate versus a severe-jaundice neonate — what is the same and what differs?