Page 12 of 20
PE17.1 | National Health Mission Programs — SDL Guide
Learning Objectives
- Describe the vision and structure of the National Health Mission (NHM) and its relationship to NRHM and NUHM
- Outline the goals, strategies and plan of action of RMNCH+A as the overarching maternal and child health framework
- Describe the objectives, target populations, and key features of RBSK, RKSK, and JSSK
- Explain the goals and phases of Mission Indradhanush and the role of ICDS in child nutrition and development
- Discuss the achievements of NHM in reducing MMR, IMR, and U5MR and identify current programme gaps
INSTRUCTIONS
India's remarkable reduction in maternal and child mortality over the past two decades — from an MMR of over 300 per 100,000 live births in 2001 to approximately 97 in 2018-20, and an IMR from 66 per 1,000 live births in 2000 to 28 in 2020 — did not happen spontaneously. It was the result of systematic, funded, government-led programmes under the National Health Mission. As a final-year MBBS graduate destined to serve in the public health system — at a PHC, district hospital, or community health centre — you are an NHM implementer. You will deploy JSSK entitlements for your patients, use IMNCI as the clinical tool of RMNCH+A's child health component, refer children detected by RBSK to DEIC, and complete immunisation under Mission Indradhanush targets. Understanding these programmes is not an optional policy module — it is the architecture within which your clinical practice will operate.
References
- MoHFW India — NHM Framework for Implementation 2012-17 (extended) (guideline)
- MoHFW India — RMNCH+A Strategy Document, 2013 (guideline)
- MoHFW India — RBSK Programme Guidelines, 2013 (guideline)
- MoHFW India — Mission Indradhanush Operational Guidelines, 2014 (and subsequent phases) (guideline)
- Ghai Essential Pediatrics, 9th edition, Ch 5 (Child Survival) and Appendix (National Programmes) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 23-year-old woman from a tribal district in Odisha is 28 weeks pregnant and has never had an antenatal visit. She arrives at the PHC for the first time because her feet are swollen. She has anaemia (Hb 8.2 g/dL) and elevated blood pressure (148/96 mmHg). Her two previous children — both delivered at home — died in the neonatal period. Under JSSK, she is entitled to free ANC consultations, free iron-folic acid tablets, free emergency transport for delivery, and free in-facility delivery care. Under RMNCH+A, her care pathway is documented on a Mother and Child Protection (MCP) card, and the ASHA is supposed to have made four HBNC-equivalent antenatal home visits. None of this happened. This case — multiplied across millions of women in India's high-focus states — is exactly the gap that the National Health Mission was designed to close. Understanding NHM's programmes is inseparable from understanding why so many preventable deaths still occur, and what the health system is doing to stop them.
WHY THIS MATTERS
The National Health Mission is the largest public health programme India has ever implemented, covering over a billion people with a mandate to reduce mortality, improve nutrition, expand immunisation, and make essential services free at the point of care. For the MBBS graduate in India, NHM is the organisational context of clinical practice: PHCs are NHM facilities, ASHAs are NHM workers, the drugs on your dispensary shelf are procured under NHM, and the patients who reach you do so via NHM-designed referral pathways. Competency PE17.1 is explicitly knowledge-level (KH) — you must be able to describe the vision, goals, strategies and plan of action of NHM and the specific programmes within it. This knowledge is tested in NMC exit examinations and is the foundation for applying the clinical skills covered in the IMNCI SDLs in this cluster.
RECALL
Before engaging with the NHM programme descriptions, activate the following prior knowledge:
- India's health indicators: India's MMR declined from ~300/100,000 LB (2001) to ~97/100,000 LB (2018-20, SRS); IMR from ~66/1,000 LB (2000) to ~28/1,000 LB (2020); U5MR from ~91/1,000 LB (2000) to ~32/1,000 LB (2020). NHM contributed significantly to these trends.
- IMNCI and HBNC (from earlier SDLs in this cluster): IMNCI is the clinical tool for RMNCH+A's child-health component; HBNC visits are the community-delivery arm of neonatal care under JSSK and RMNCH+A.
- National Immunization Schedule (NIS): understand the current schedule — Mission Indradhanush targets children who missed vaccines in this schedule.
- Community health workers: ASHA (Accredited Social Health Activist) — demand-side mobiliser, trained in IMNCI, paid by performance; ANM (Auxiliary Nurse Midwife) — facility-linked, supervisory role; AWW (Anganwadi Worker) — ICDS nutrition and early childhood development.
- Malnutrition criteria (from IMNCI cluster SDLs): SAM MUAC <11.5 cm, MAM 11.5–12.4 cm — detected through ICDS and RBSK screening, referred through NRC under NHM.
Introduction: What Is the National Health Mission and Why Does It Matter?
The National Health Mission (NHM) was launched in April 2013 as an umbrella programme integrating two earlier initiatives: the National Rural Health Mission (NRHM) (launched 2005, focusing on rural areas and 18 high-focus 'EAG' states) and the National Urban Health Mission (NUHM) (launched 2013, extending the same framework to urban underserved populations). The NHM is implemented by the Ministry of Health and Family Welfare (MoHFW) through state governments, with central funding supplemented by state contributions.
The NHM's overarching vision is to attain the highest possible level of health and wellbeing for all Indians — specifically by reducing maternal and child mortality, addressing communicable and non-communicable diseases, and universalising access to comprehensive primary health care. The mission operates through four strategic approaches: (1) Strengthening primary health infrastructure — building and upgrading sub-centres, PHCs, and CHCs to Indian Public Health Standards; (2) Flexible programme architecture — allowing states to adapt national frameworks to local needs through Programme Implementation Plans (PIPs); (3) Community health worker deployment — ASHAs and AWWs as the interface between communities and the health system; and (4) Free essential services at government facilities — particularly under the JSSK, RBSK, and RMNCH+A entitlements.
For the MBBS graduate, NHM is not an abstract policy framework — it is the system within which your clinical work will be embedded. Your PHC post is an NHM posting. Your daily practice of IMNCI, use of JSSK entitlements, participation in Mission Indradhanush immunisation rounds, and referral of malnourished children to NRCs are all NHM activities. Understanding the programme structure is prerequisite to implementing it correctly.
India's MCH Burden: The Magnitude That Drove NHM
The National Health Mission was created in direct response to India's stark maternal and child health (MCH) burden — a burden that persisted despite two decades of economic growth and was concentrated geographically and socially in ways that made targeted programmatic action essential.
Pre-NHM India (2000–2005) carried a mortality burden that stood in sharp contrast to international comparisons: India's Maternal Mortality Rate (MMR) of approximately 300 per 100,000 live births in 2001 was four times higher than the WHO-recommended threshold for high-performing systems (<75 per 100,000 LB). The Infant Mortality Rate (IMR) of 66 per 1,000 live births in 2000 was among the highest in Asia. And the Neonatal Mortality Rate (NMR) of approximately 44 per 1,000 live births reflected a health system that was losing the most critical battle — keeping newborns alive in their first month.
Critically, these national averages concealed profound inter-state disparities. The Empowered Action Group (EAG) states — Rajasthan, Uttar Pradesh, Bihar, Madhya Pradesh, Uttarakhand, Jharkhand, Chhattisgarh, Odisha, Jammu & Kashmir, Assam, and Himachal Pradesh — had far worse indicators than the national average. Uttar Pradesh's NMR in 2000 was over 50 per 1,000 live births; Kerala's was below 10. This 5-fold difference within a single country demanded a targeted, additional allocation of NHM resources to these high-focus states.
The causes of this mortality were known and largely preventable: haemorrhage, hypertensive disorders, sepsis, and unsafe abortion accounted for most maternal deaths; pneumonia, diarrhoea, sepsis, birth asphyxia, and malnutrition for most child deaths. The gap between what was known and what was being delivered — a 'knowledge-to-action' gap — was the NHM's primary target.
- MMR (India): 2001 ~300 → 2011-13 ~167 → 2018-20 ~97 per 100,000 live births
- IMR (India): 2000 66 → 2010 47 → 2020 28 per 1,000 live births
- U5MR (India): 2000 91 → 2010 59 → 2020 32 per 1,000 live births
- Full immunisation coverage: 2005 ~44% → 2021 ~76% (NFHS-5)
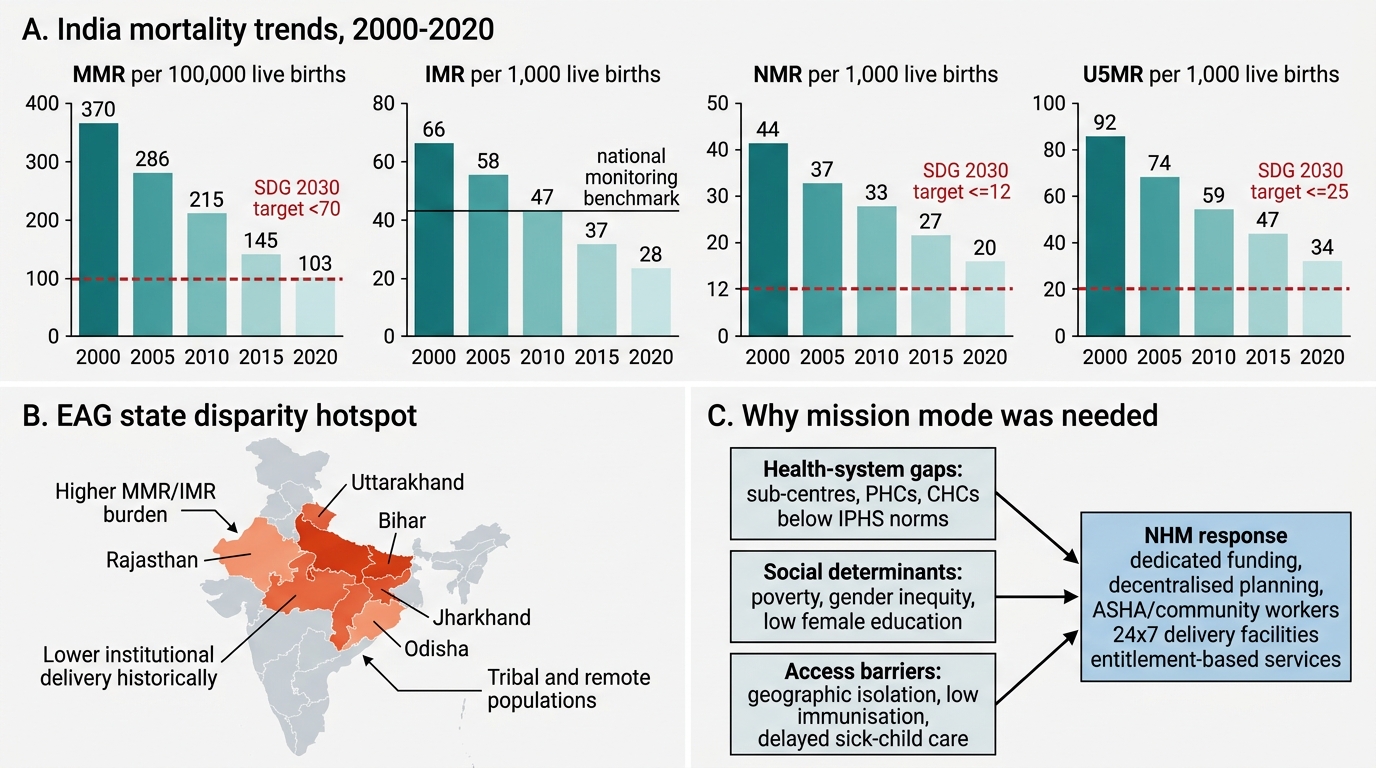
India MCH Mortality Trends and EAG Disparities
Why Mission Mode? Determinants of MCH Programme Gaps
The 'mission mode' of NHM — with its dedicated funding streams, decentralised implementation, community health worker architecture, and entitlement-based service guarantees — was chosen because earlier, fragmented approaches to maternal and child health had consistently failed to reach the most vulnerable populations. Understanding why a mission-mode approach was necessary requires understanding the determinants of India's MCH gap.
Health system barriers were the most proximate cause: India had severe shortfalls in sub-centres, PHCs, and CHCs meeting Indian Public Health Standards (IPHS) norms. In 2005, the NRHM found that over 40% of sub-centres and PHCs in high-focus states had inadequate staffing, infrastructure, or drug supply to deliver even basic maternal and child health services. The concept of a 24×7 delivery facility — available any night and any week — was absent at most PHCs.
Social and economic determinants were equally important. Tribal, Dalit, and Muslim women in India's high-focus states had dramatically lower institutional delivery rates, lower immunisation uptake, and lower care-seeking rates for sick children than the national average — reflecting intersections of poverty, educational disadvantage, gender discrimination, and geographic isolation. No clinical intervention could reach these women without a demand-side mechanism to mobilise them and an economic barrier-removal strategy (free services, transport incentives).
Geographic access barriers — the distance from village to facility, lack of roads in tribal areas, absence of emergency referral transport — were a direct contributor to deaths that occurred during the delay between deciding to seek care and arriving at a facility. The three-delays model (delay in deciding, delay in reaching, delay in receiving care) framed NHM's referral-transport and facility-strengthening investments.
Programmatic fragmentation compounded these barriers: before NRHM, vertical programmes (malaria control, family planning, immunisation, RCH) operated in silos with separate reporting lines, separate budgets, and separate community workers — creating confusion for beneficiaries and inefficiency at the facility level. NRHM's flexible pool mechanism integrated these vertical programmes under a single district health plan.
SELF-CHECK
Which of the following BEST describes the relationship between NRHM, NUHM, and NHM?
A. NHM replaced both NRHM and NUHM, which no longer exist as programmes
B. NHM is the umbrella mission launched in 2013 that integrates NRHM (rural, 2005) and NUHM (urban, 2013) under a single framework
C. NRHM and NUHM are parallel missions that operate independently under NHM coordination
D. NUHM was created before NRHM to address urban slum health, and NRHM was added later
Reveal Answer
Answer: B. NHM is the umbrella mission launched in 2013 that integrates NRHM (rural, 2005) and NUHM (urban, 2013) under a single framework
NHM was launched in April 2013 as the umbrella programme that integrates the existing NRHM (National Rural Health Mission, launched 2005, focused on rural areas and EAG high-focus states) and the newly created NUHM (National Urban Health Mission, launched alongside NHM in 2013, covering urban underserved populations). NRHM and NUHM continue as sub-missions within the NHM framework — they were not abolished but integrated. The unification addressed the gap that NRHM had left urban slums uncovered.