Page 1 of 10
PA20.3 | Multiple Myeloma — Lab Findings & Diagnosis — SDL Guide
Learning Objectives
- Trace the differentiation pathway from B-cell to plasma cell and explain its significance in understanding clonal disorders.
- Define multiple myeloma and describe the pathogenesis including the role of cytokines and osteoclast activation.
- List the CRAB features and additional clinical manifestations of multiple myeloma.
- Interpret the key laboratory findings — M-spike on SPEP, Bence-Jones protein, rouleaux, and bone marrow plasma cell percentage — and explain their diagnostic significance.
- State the diagnostic criteria for multiple myeloma and distinguish it from MGUS and Waldenström macroglobulinaemia.
INSTRUCTIONS
Multiple myeloma is the archetype of plasma cell dyscrasias — a group of disorders defined by clonal expansion of immunoglobulin-secreting plasma cells. For a Year-2 pathology student, this topic bridges haematology, renal pathology, and bone disease under a single unifying mechanism: a malignant clone that floods the body with a useless monoclonal protein while crowding out normal marrow function. The laboratory findings are among the most clinically distinctive in all of pathology, making this a perennial exam and clinical favourite.
References
- Robbins & Kumar: Basic Pathology, 11th ed., Ch 12 (Haematopoietic and Lymphoid Systems) (textbook)
- Harsh Mohan: Textbook of Pathology, 8th ed., Ch 13 (Disorders of Leucocytes and Lymphoreticular Tissues) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 62-year-old man walks in with six months of progressively worsening back pain. His GP treated it as a disc problem — but an X-ray reveals multiple punched-out lesions in the skull, and his blood report shows a strikingly high total protein with a haemoglobin of 8 g/dL. The lab calls you about a peculiar band on his serum protein electrophoresis. What is destroying his bones, paralyzing his kidneys, and producing this anomalous protein — all at once?
RECALL
Before tackling myeloma, lock in these Year-1 anchors:
- B lymphocyte → activated by antigen → differentiates into plasma cell (via germinal centre reaction, somatic hypermutation, class switching)
- Plasma cells are terminally differentiated; they do NOT circulate — they reside in bone marrow
- Each plasma cell secretes a single class of immunoglobulin (IgG, IgA, IgM, IgD, or IgE) made of two heavy chains + two light chains (κ or λ)
- Normal marrow contains <5% plasma cells
- Serum protein electrophoresis (SPEP) separates proteins by charge: albumin runs fastest (furthest), then α1, α2, β, γ globulins. Immunoglobulins migrate in the γ-β region.
If any of these feel hazy, skim your Year-1 immunology notes before continuing — myeloma pathogenesis will make much more sense.
What Is Multiple Myeloma?

Multiple Myeloma: Clonal Plasma Cell Neoplasm of Bone Marrow
Multiple myeloma (MM) is a malignant neoplasm of clonal plasma cells that proliferate within the bone marrow and secrete a single structurally identical immunoglobulin or immunoglobulin fragment — the monoclonal protein (M-protein).
Key defining features:
• Clonal — all malignant cells descend from one transformed precursor and make identical immunoglobulin
• Bone marrow is the primary site; "multiple" reflects the multifocal nature of marrow involvement
• The M-protein is functionally useless (does not provide immune defence) yet accumulates to high concentrations
• Normal immunoglobulin production is suppressed (immune paresis), predisposing to infections
MM accounts for ~10% of all haematologic malignancies and is predominantly a disease of adults over 60 years.
Cross-reference: MM sits at the end of the B-cell neoplasm spectrum covered in Cluster H8 — from CLL/SLL (early B-cell) → follicular lymphoma → diffuse large B-cell lymphoma → plasmacytoma → multiple myeloma (terminally differentiated B-cell).
Pathogenesis

Pathogenesis of Multiple Myeloma
The malignant transformation occurs in a post-germinal centre, class-switched B cell (or early plasma cell precursor). Key pathogenetic steps:
1. Clonal plasma cell expansion in marrow
Malignant plasma cells home to and proliferate within the bone marrow microenvironment, supported by interactions with stromal cells.
2. Cytokine-driven growth — IL-6 axis
Interleukin-6 (IL-6) is the principal growth and survival factor for myeloma cells. Stromal cells and the myeloma cells themselves produce IL-6 in an autocrine/paracrine loop, driving clonal expansion and resistance to apoptosis.
3. Osteoclast activation — RANKL pathway
Myeloma cells and stromal cells produce RANK-L (receptor activator of NF-κB ligand), which activates osteoclasts while simultaneously suppressing osteoblasts (via DKK-1). The net result: pure osteolytic bone destruction with NO new bone formation — the hallmark of myeloma bone disease.
Contrast with metastatic carcinoma (which can be osteoblastic, e.g., prostate) and Paget's disease (increased both osteoclast and osteoblast activity).
4. M-protein accumulation
The monoclonal protein (most commonly IgG > IgA > IgD > IgM/IgE) saturates reticuloendothelial clearance, deposits in tissues (kidney, nerves), and raises serum viscosity. Free light chains (κ or λ) spill into urine as Bence-Jones protein.
CLINICAL PEARL
Why does myeloma cause ONLY lytic lesions (no sclerosis)? Because myeloma cells produce DKK-1, which specifically inhibits the Wnt signalling pathway in osteoblasts, completely uncoupling bone resorption from formation. A bone scan is therefore often NEGATIVE in myeloma (no osteoblast activity = no tracer uptake) — plain X-ray or MRI is required to detect the lytic lesions. This is a classic exam trap.
Clinical Features — CRAB and Beyond
Clinical Features of Multiple Myeloma: CRAB and Beyond
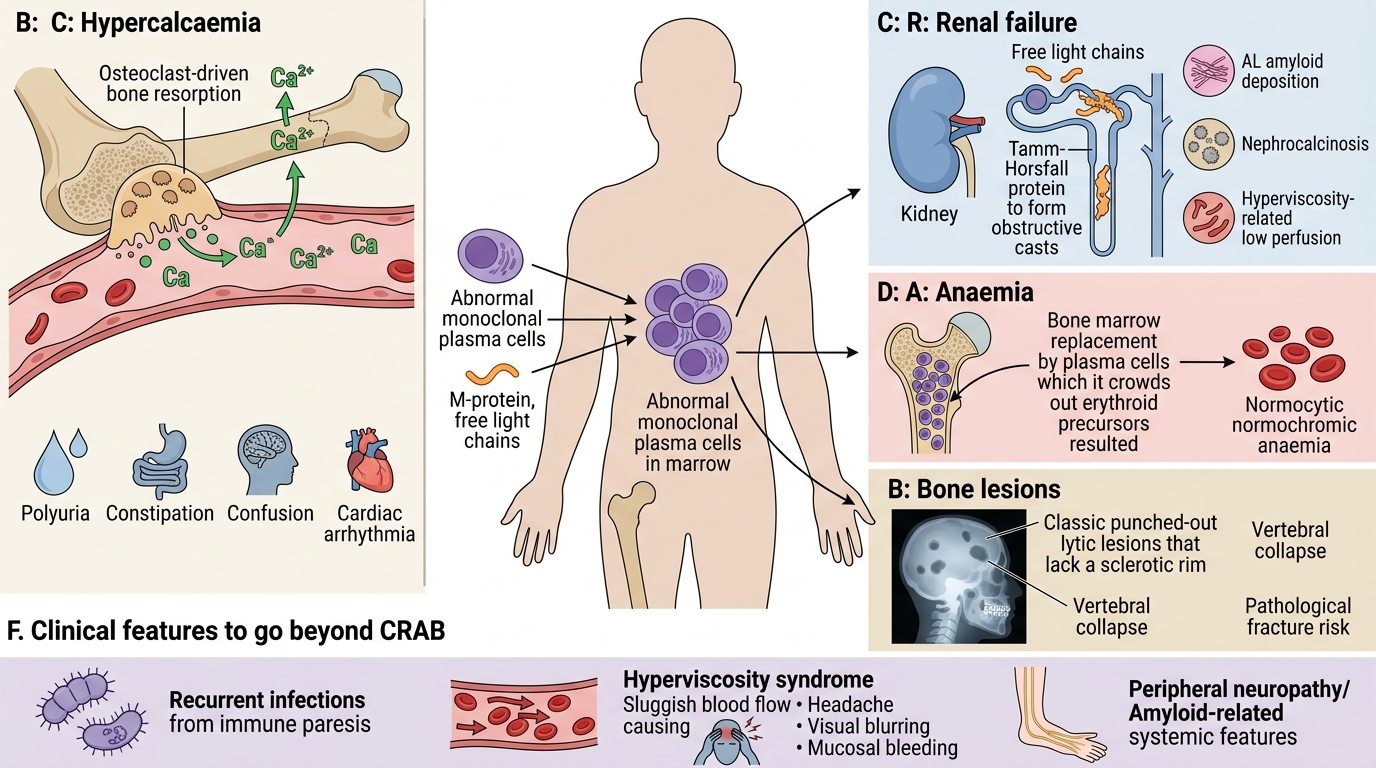
The mnemonic CRAB captures the four myeloma-defining organ damage events:
C — HyperCalcaemia
Osteoclastic bone resorption releases calcium into the blood. Symptoms: polyuria, constipation, confusion, cardiac arrhythmias. Ca²⁺ >2.75 mmol/L (corrected for albumin).
R — Renal Failure
Multiple mechanisms:
• Light chain cast nephropathy ("myeloma kidney") — free light chains precipitate with Tamm-Horsfall protein in tubules, forming obstructive casts → tubular atrophy
• AL amyloidosis — light chain fragments deposit as amyloid fibrils (particularly λ chains)
• Hypercalcaemia → nephrocalcinosis
• Hyperviscosity → reduced renal perfusion
A — Anaemia
Normocytic normochromic anaemia from marrow replacement (plasma cell crowding displaces erythroid precursors) + chronic disease cytokines suppressing erythropoiesis.
B — Bone Lesions
Classic "punched-out" lytic lesions on plain X-ray (no sclerotic rim). Predilection: axial skeleton (vertebrae, skull, pelvis, ribs, proximal long bones). Vertebral collapse → back pain, pathological fractures, spinal cord compression.
Additional features beyond CRAB:
• Recurrent infections — immune paresis (suppressed normal Ig) + neutropenia from marrow replacement; encapsulated organisms (pneumococcus) predominate
• Hyperviscosity syndrome — IgA/IgG3 paraproteins cause sludging → headache, visual blurring, mucosal bleeding; more dramatic in Waldenström (IgM)
• Peripheral neuropathy — M-protein or amyloid deposits on myelin sheaths
• AL amyloidosis — macroglossia, carpal tunnel syndrome, restrictive cardiomyopathy
SELF-CHECK
A myeloma patient with severe back pain undergoes a bone scan — it is reported as normal. The most likely explanation is:
A. The scan was technically inadequate and should be repeated
B. Myeloma causes purely lytic lesions with no osteoblast activity, so there is no tracer uptake
C. The back pain is unrelated to myeloma in this case
D. Bone scan is the wrong modality; only PET-CT is useful in myeloma
Reveal Answer
Answer: B. Myeloma causes purely lytic lesions with no osteoblast activity, so there is no tracer uptake
Myeloma bone disease is purely osteolytic — RANKL activates osteoclasts but DKK-1 simultaneously suppresses osteoblasts. Technetium-99m bone scans detect osteoblast activity (new bone formation). In the absence of osteoblast activity, there is no tracer uptake and the scan appears normal or falsely negative. Plain X-ray (skeletal survey) and MRI are the standard imaging modalities for myeloma bone disease.