Page 2 of 27
PA21.1 | ABO & Rh Blood Group Systems — SDL Guide (Part 2)
ABO Inheritance and the Bombay Phenotype

ABO Inheritance and the Bombay Phenotype
Inheritance pattern:
• A and B alleles are codominant (both expressed when present together → AB phenotype)
• O allele is functionally recessive (the enzyme is non-functional, so group O is expressed only when homozygous OO or when no A/B allele is present)
• Possible genotypes: AA, AO (both express Group A phenotype), BB, BO (Group B), AB (Group AB), OO (Group O)
Bombay phenotype (Oh):
Rarely (~1 in 10,000 in India, higher in South India), the H gene itself is homozygous non-functional. No H substance is produced → no A or B antigens can be made regardless of the ABO genotype.
• Bombay individuals type as Group O on routine testing, but their plasma contains anti-A + anti-B + anti-H — the most potent combination.
• They can only receive blood from other Bombay donors.
• Clinical trap: a Bombay patient who receives routine Group O blood will have a life-threatening haemolytic transfusion reaction (because Group O cells still carry abundant H antigen).
• Bombay phenotype is more prevalent in India than in Europe — clinically relevant for the Indian physician.
CLINICAL PEARL
Universal donor and its limits: Group O Rh-negative blood is called the 'universal donor' because it lacks A, B, and D antigens. In life-threatening emergencies when blood group is unknown, O-negative packed red cells are given. However, this is NOT truly universal: (1) The plasma of O whole blood contains anti-A and anti-B which can haemolyse recipient cells if given in large volumes — use packed cells, not whole blood. (2) O-negative is only ~7% of donors, so stocks are limited and should be reserved for true emergencies. (3) Bombay patients cannot receive even O-negative blood safely.
ABO Incompatibility: Mechanism of Intravascular Haemolysis
ABO Incompatibility: Intravascular Haemolysis Mechanism
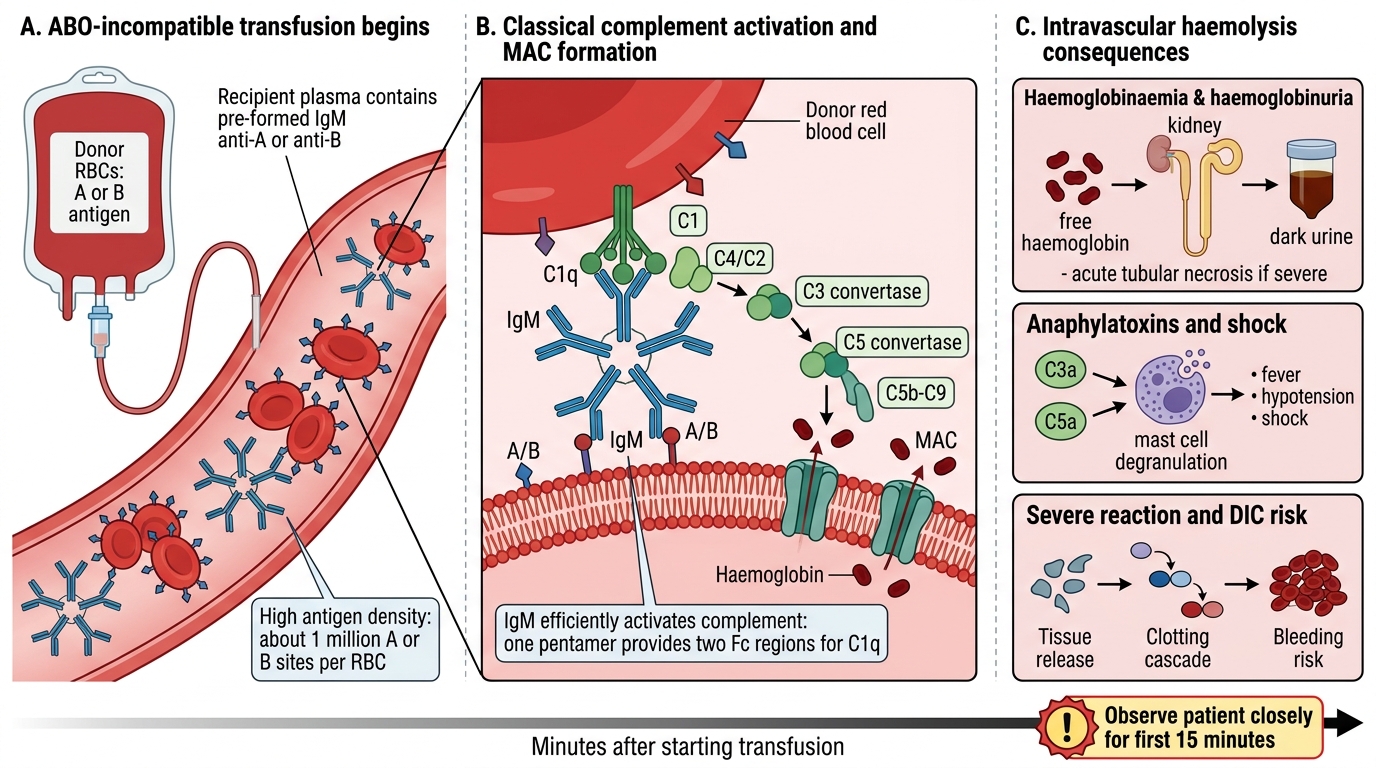
When ABO-incompatible blood enters the circulation:
1. Pre-formed IgM anti-A or anti-B binds immediately to antigens on donor RBCs (antigen density is high — ~1 million A or B sites per RBC).
2. IgM pentamers are highly efficient at activating the classical complement pathway (two Fc regions needed to bind C1q — one IgM molecule provides both).
3. Complement cascade proceeds to completion → membrane attack complex (MAC) inserts into the RBC membrane → intravascular haemolysis (haemoglobin released directly into plasma).
4. Released haemoglobin → haemoglobinaemia → haemoglobinuria (dark urine) → acute tubular necrosis if severe.
5. Complement fragments (C3a, C5a) → mast cell degranulation → fever, hypotension, shock.
6. Tissue factor release → DIC risk in severe reactions.
This entire sequence can begin within minutes of starting a transfusion — hence the rule to observe the patient for the first 15 minutes of every transfusion.
The Rh System: D Antigen and Rh Status

RhD Antigen and Rh Status
The Rh system is the second most clinically important blood group system. It comprises over 50 antigens encoded by two closely linked genes on chromosome 1 (RHD and RHCE), but clinical practice focuses almost entirely on the D antigen (also called RhD).
- Rh-positive (Rh+): D antigen present on RBCs (~85% of the Indian population)
- Rh-negative (Rh−): D antigen absent (~15% — varies by ethnicity)
The D antigen is a transmembrane protein (not an oligosaccharide like ABO antigens). It is the most immunogenic of all blood group antigens apart from ABO — a single exposure to as little as 0.1 mL of Rh+ blood in an Rh-negative individual can trigger sensitisation.
Critical difference from ABO:
• There are no natural anti-D antibodies. Rh-negative individuals do NOT have anti-D in their plasma unless previously sensitised.
• Anti-D is an immune antibody — it forms only after exposure to D antigen (via transfusion or fetomaternal haemorrhage).
• Class: IgG (monomeric, crosses the placenta).

Rh Blood Group System: RhD Protein Expression