Page 14 of 27
PA21.4 | Transfusion Reactions & Investigation — SDL Guide (Part 2)
Allergic/Urticarial and Anaphylactic Reactions

Allergic and Anaphylactic Transfusion Reactions
Allergic (urticarial) reactions are the second most common type, affecting ~1% of transfusions.
Mechanism: IgE antibodies in the recipient react with donor plasma proteins → mast cell and basophil degranulation → histamine release.
Features: Urticaria, pruritus, flushing — without fever. Usually mild; transfusion can be slowed and restarted after antihistamine.
Anaphylactic reactions are rare but life-threatening.
Mechanism: The classic scenario is IgA deficiency in the recipient. IgA-deficient patients develop anti-IgA IgG or IgE antibodies after exposure. When transfused with IgA-containing blood products, massive anaphylaxis follows.
Features: Rapid onset — urticaria, bronchospasm, angioedema, hypotension, cardiovascular collapse — without fever (unlike AHTR).
Management: Adrenaline (epinephrine) IM; oxygen; IV fluids. Future transfusions must use washed red cells (IgA removed) or blood from IgA-deficient donors.
Transfusion-Related Acute Lung Injury (TRALI)
Transfusion-Related Acute Lung Injury (TRALI)
Transfusion-related acute lung injury (TRALI) is a leading cause of transfusion-related mortality in high-income settings.
Mechanism:
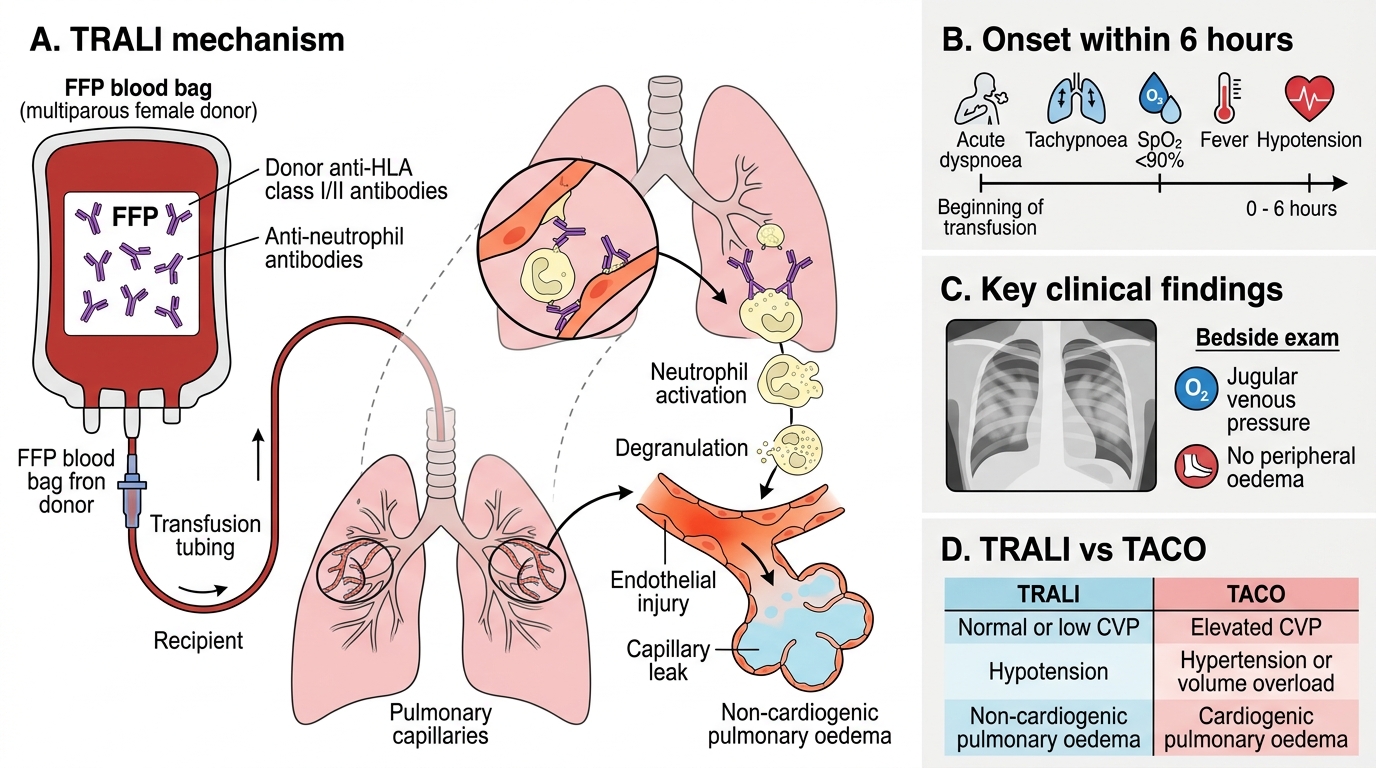
• Donor blood (especially multiparous female donors) contains anti-HLA class I/II or anti-neutrophil antibodies.
• These antibodies activate recipient neutrophils in pulmonary capillaries.
• Neutrophil degranulation → endothelial injury → non-cardiogenic pulmonary oedema.
Clinical features (onset within 6 hours):
• Acute respiratory distress — tachypnoea, hypoxia (SpO₂ <90%)
• Bilateral pulmonary infiltrates on chest X-ray
• No elevated JVP or cardiac cause (distinguishes from TACO)
• Fever, hypotension
Key distinction from TACO: TRALI = normal/low CVP, non-cardiogenic; TACO = elevated CVP, cardiogenic. Both present with respiratory distress and bilateral infiltrates.
Prevention: Many blood banks defer high-risk donors (multiparous women with anti-leukocyte antibodies) from plasma-containing donations.
SELF-CHECK
A patient develops acute respiratory distress with bilateral pulmonary infiltrates and hypotension 3 hours after receiving fresh frozen plasma (FFP). JVP is normal and there is no peripheral oedema. Which transfusion reaction is most likely?
A. Transfusion-associated circulatory overload (TACO)
B. Anaphylactic reaction
C. Transfusion-related acute lung injury (TRALI)
D. Acute haemolytic transfusion reaction (AHTR)
Reveal Answer
Answer: C. Transfusion-related acute lung injury (TRALI)
TRALI presents with acute non-cardiogenic pulmonary oedema — bilateral infiltrates, hypoxia, and hypotension within 6 hours, with a normal JVP. FFP from multiparous donors is a common implicated product because it contains anti-HLA antibodies. TACO (A) also causes bilateral infiltrates but JVP is elevated and it is cardiogenic. Anaphylaxis (B) causes bronchospasm and urticaria, not bilateral infiltrates. AHTR (D) causes haemolysis and renal failure, not isolated lung injury.
Acute Non-Immune Reactions

Acute Non-Immune Transfusion Reactions
1. Transfusion-Associated Circulatory Overload (TACO)
TACO is the leading cause of transfusion mortality in elderly patients and in those with poor cardiac or renal reserve.
Mechanism: Rapid or excessive volume infusion → left ventricular failure → cardiogenic pulmonary oedema.
Features: Dyspnoea, hypertension, elevated JVP, bilateral crackles, orthopnoea — onset during or shortly after transfusion.
Prevention: Transfuse slowly (1 unit over 3–4 hours); use a loop diuretic between units in at-risk patients.
2. Septic (Bacterial) Reaction
Mechanism: Bacterial contamination of the blood unit — most commonly Yersinia enterocolitica (stored RBCs, psychrophilic) or Staphylococcus aureus (platelets, room temperature storage).
Features: High fever, rigors, hypotension, shock — often within minutes; clinically mimics AHTR.
Investigation: Blood culture from the patient AND the unit simultaneously.
3. Metabolic/Citrate Complications
Massive transfusion (>10 units in 24 h) can cause:
• Citrate toxicity → chelates ionised calcium → hypocalcaemia → tetany, cardiac arrhythmias.
• Hyperkalaemia — stored red cells leak potassium; dangerous in renal failure.
• Hypothermia — cold blood lowers core temperature; impairs coagulation.