Page 11 of 21
PA16.3 | Acquired Haemolytic Anaemias & Smear Morphology — SDL Guide (Part 2)
The Direct Antiglobulin Test (DAT / Direct Coombs) — Principle & Interpretation
Direct Antiglobulin Test: Principle and Interpretation
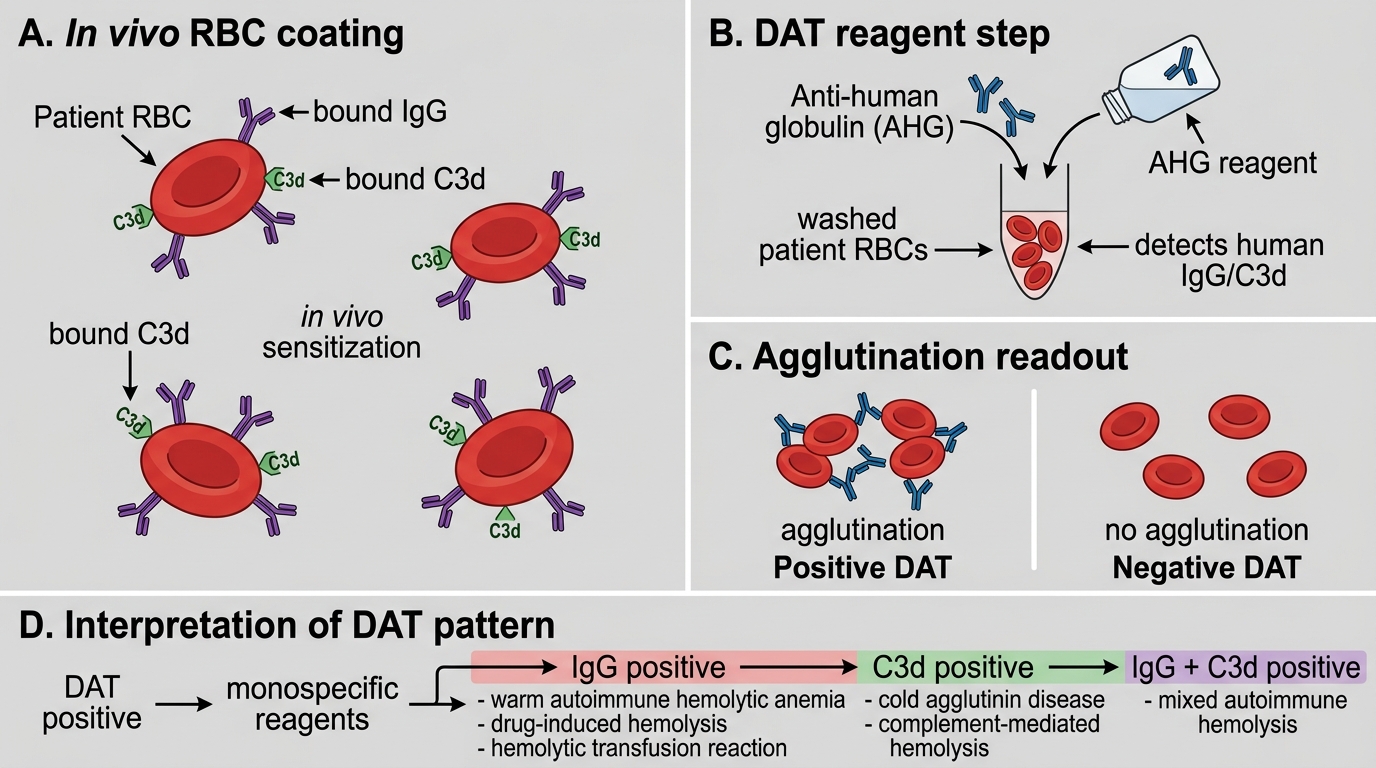
The direct antiglobulin test (DAT) detects antibodies or complement (C3d) bound to the patient's own circulating red cells.
Principle:
1. Patient's washed red cells (already coated in vivo) are incubated with anti-human globulin (AHG) reagent — a polyclonal antibody that cross-links human IgG and C3d.
2. Cross-linking of IgG or C3d on adjacent red cells → agglutination = positive DAT.
3. Specific reagents distinguish IgG-positive from C3d-positive results.
Interpretation grid:
| DAT result | Most likely type |
|---|---|
| IgG positive, C3d negative | Warm AIHA (IgG alone) |
| IgG positive, C3d positive | Warm AIHA (IgG + complement activation) |
| IgG negative, C3d positive | Cold AIHA (IgM dissociated, C3d remains) |
| Negative | Non-immune haemolysis (MAHA, PNH, mechanical, etc.) |
Indirect Coombs test: Detects free antibody in the patient's serum against test red cells — used in cross-matching, not primary haemolysis diagnosis.

Direct Antiglobulin Test (DAT) Principle
CLINICAL PEARL
DAT-negative haemolysis does NOT rule out immune-mediated disease. Approximately 5–10% of warm AIHA cases are DAT-negative (antibody titre too low for the assay, IgA or IgM antibodies missed by standard reagent, or complement-only coating). If haemolysis is brisk and the smear shows spherocytes, request a more sensitive gel-card DAT or flow cytometric Coombs before dismissing immune cause.
Microangiopathic Haemolytic Anaemia (MAHA)
⚑ AI image — pending faculty review (auto-QA score 8/10; best of 3 attempts)
Microangiopathic Haemolytic Anaemia
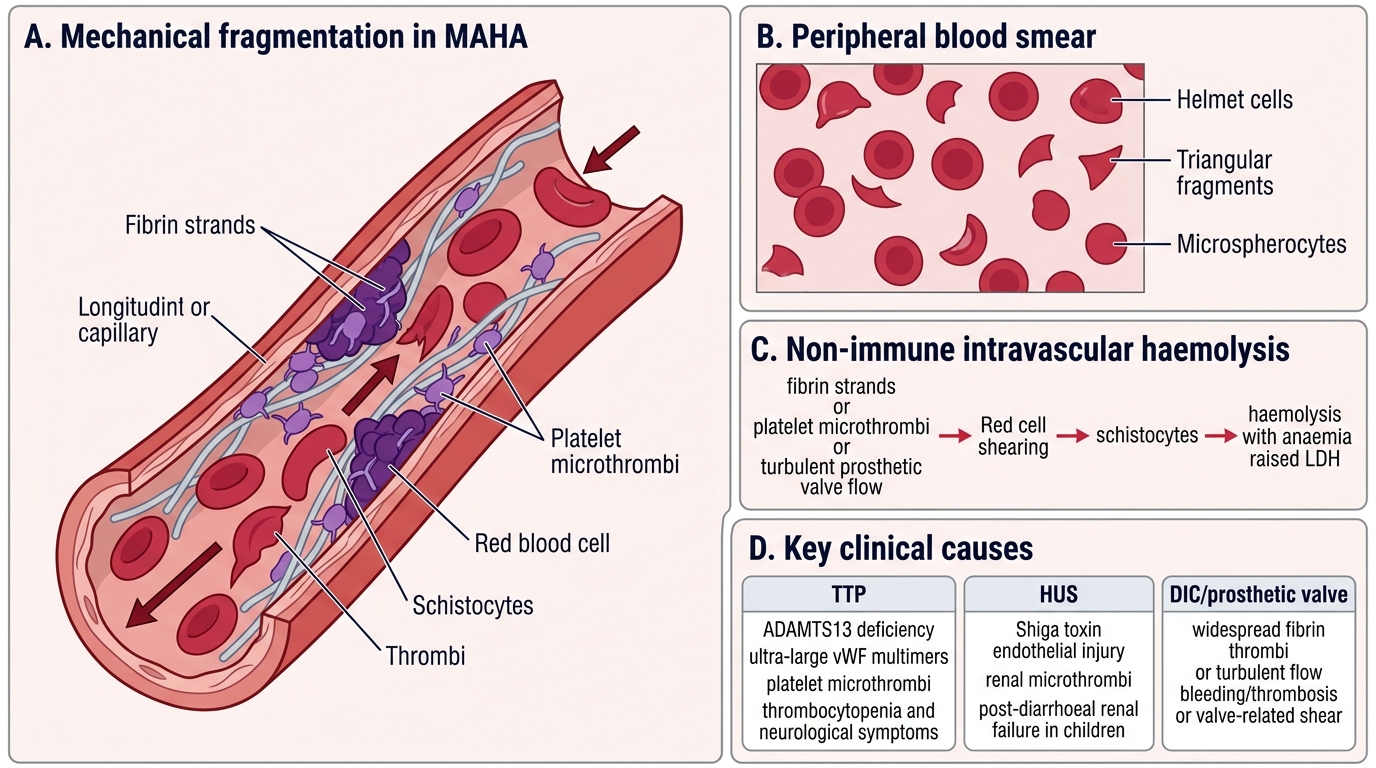
Microangiopathic haemolytic anaemia (MAHA) is mechanical, non-immune fragmentation haemolysis caused by red cells colliding with pathological intravascular surfaces.
Mechanism: Fibrin strands, platelet microthrombi, or turbulent flow (prosthetic valves) physically shear red cells → schistocytes (helmet cells, triangular fragments, microspherocytes).
Key causes and distinguishing features:
| Cause | Key pathology | Distinguishing features |
|---|---|---|
| TTP (thrombotic thrombocytopenic purpura) | ADAMTS13 deficiency → ultra-large vWF multimers → platelet microthrombi | Pentad: MAHA + thrombocytopenia + fever + renal failure + neurological symptoms |
| HUS (haemolytic uraemic syndrome) | Shiga toxin (STEC O157:H7) → endothelial injury → renal microthrombi | Post-diarrhoeal, predominantly renal failure, children |
| DIC | Widespread fibrin deposition in vessels | Prolonged PT, APTT, ↓fibrinogen, ↑D-dimer; often in sepsis/obstetric emergency |
| Mechanical valve | Turbulent flow + prosthetic surface | Isolated MAHA, no thrombocytopenia, audible valve click |
Peripheral smear hallmark: Schistocytes (>1% of RBCs diagnostic) + polychromasia. No spherocytes (different mechanism).

TTP Peripheral Blood Smear: Schistocytes and Thrombocytopenia
DAT: Negative (non-immune).
SELF-CHECK
A 35-year-old woman presents with sudden confusion, petechiae, and anaemia. CBC shows Hb 7 g/dL, platelets 18 × 10⁹/L. Peripheral smear: numerous helmet-shaped RBC fragments, polychromasia. Creatinine: 1.8 mg/dL. DAT: negative. Which diagnosis fits BEST?
A. Warm autoimmune haemolytic anaemia
B. Hereditary spherocytosis with aplastic crisis
C. Thrombotic thrombocytopenic purpura (TTP)
D. G6PD deficiency after oxidative stress
Reveal Answer
Answer: C. Thrombotic thrombocytopenic purpura (TTP)
The triad of MAHA (schistocytes on smear), severe thrombocytopenia, and neurological symptoms (confusion) with negative DAT is the classic presentation of TTP. ADAMTS13 deficiency leads to ultra-large vWF multimers, spontaneous platelet microthrombi throughout the microvasculature, and mechanical shearing of red cells. HUS would be more renal-dominant and post-diarrhoeal. Spherocytes and a positive DAT would point to AIHA. G6PD produces bite cells, not schistocytes.
Paroxysmal Nocturnal Haemoglobinuria (PNH)

Paroxysmal Nocturnal Haemoglobinuria: Mechanism, Features, and Diagnosis
Paroxysmal nocturnal haemoglobinuria (PNH) is an acquired clonal haematopoietic stem cell disorder caused by a somatic mutation in the PIG-A gene (X-linked), which is essential for GPI-anchor biosynthesis.
Pathogenesis:
1. Absence of GPI-anchored complement regulatory proteins — particularly CD55 (decay-accelerating factor) and CD59 (protectin) — on the red cell surface.
2. Without CD55/CD59 to brake complement, the membrane attack complex (C5b-9) forms freely on PNH red cells.
3. Result: intravascular haemolysis, especially during sleep (due to relative acidosis of nocturnal apnoea) — classic morning haemoglobinuria.
Clinical triad: Haemolytic anaemia + venous thrombosis (especially unusual sites: hepatic vein → Budd-Chiari, cerebral venous sinus) + cytopenias.
Smear: Often normocytic/normochromic or mildly macrocytic (due to haemolysis + folate use). No specific morphological hallmark.
Diagnosis: Flow cytometry — reduced or absent CD55 and CD59 on red cells and granulocytes (high sensitivity). The older Ham's acidified serum test has been replaced.
DAT: Negative (complement, not antibody).