Page 1 of 23
PA19.1 | Approach to Lymphadenopathy — SDL Guide
Learning Objectives
- Recall the normal microanatomy of a lymph node (cortex, paracortex, medulla) and their cellular constituents.
- Define lymphadenopathy and distinguish physiological from pathological causes.
- Apply the reactive vs neoplastic framework to classify the causes of lymphadenopathy.
- Identify the three reactive hyperplasia patterns and map each to a clinical aetiology.
- Use clinical discriminators — size, consistency, tenderness, mobility, site, and age — to build a working differential diagnosis.
- Justify why excision biopsy is preferred over FNAC when lymphoma is suspected.
- Recognise how this module connects to SDL2 (TB lymphadenitis), SDL3 (Hodgkin lymphoma), and SDL4 (Non-Hodgkin lymphoma).
INSTRUCTIONS
Lymphadenopathy is one of the most common signs a Year-2 student will encounter on ward rounds and in the exam hall. A single palpable node might represent a trivial viral infection or a curable lymphoma — and the clinical features that separate them are learnable, systematic, and high-yield. This module builds the diagnostic framework you will use repeatedly through your clinical years. Work through it in one sitting (~19 min); revisit the reactive hyperplasia patterns before SDL3.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 13 (Diseases of White Blood Cells, Lymph Nodes, Spleen, and Thymus) (textbook)
- Harsh Mohan Textbook of Pathology, 7th ed., Ch 31 (Lymph Nodes and Spleen) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old engineering student comes to the OPD with a 6-week history of a painless neck swelling. He has no fever, no weight loss — yet. His father asks: "Is it cancer, doctor?" You palpate a firm, non-tender, rubbery, 3 × 4 cm node in the posterior triangle. You cannot answer the father's question yet — but by the end of this module you will know exactly what clinical features to elicit, what they mean pathologically, and which investigation to order next.
RECALL
Before we explore disease, anchor the normal anatomy.
A lymph node is an encapsulated, bean-shaped secondary lymphoid organ interposed in the lymphatic system. Its architecture is organised into three compartments:
- Cortex — outermost zone; contains primary follicles (resting, naïve B cells) and secondary follicles (B cells that have encountered antigen, forming a germinal centre surrounded by a mantle zone).
- Paracortex (deep cortex) — thymus-dependent zone; home to T lymphocytes and interdigitating dendritic cells that present antigen. Expands dramatically during viral infections and drug reactions.
- Medulla — innermost zone; composed of medullary cords (plasma cells, macrophages) and medullary sinuses (macrophage-lined channels that filter lymph before it exits via the efferent lymphatic).
Afferent lymphatics pierce the capsule and drain into the subcapsular sinus. Lymph percolates through cortical and medullary sinuses, exits via the hilum, and drains into the venous circulation.

Normal Lymph Node Microanatomy
Relevant to PA19.1: every compartment has a signature expansion pattern — and each pattern points to a different cause of lymphadenopathy.
Defining Lymphadenopathy
Defining Lymphadenopathy: Size, Duration, and Red Flags
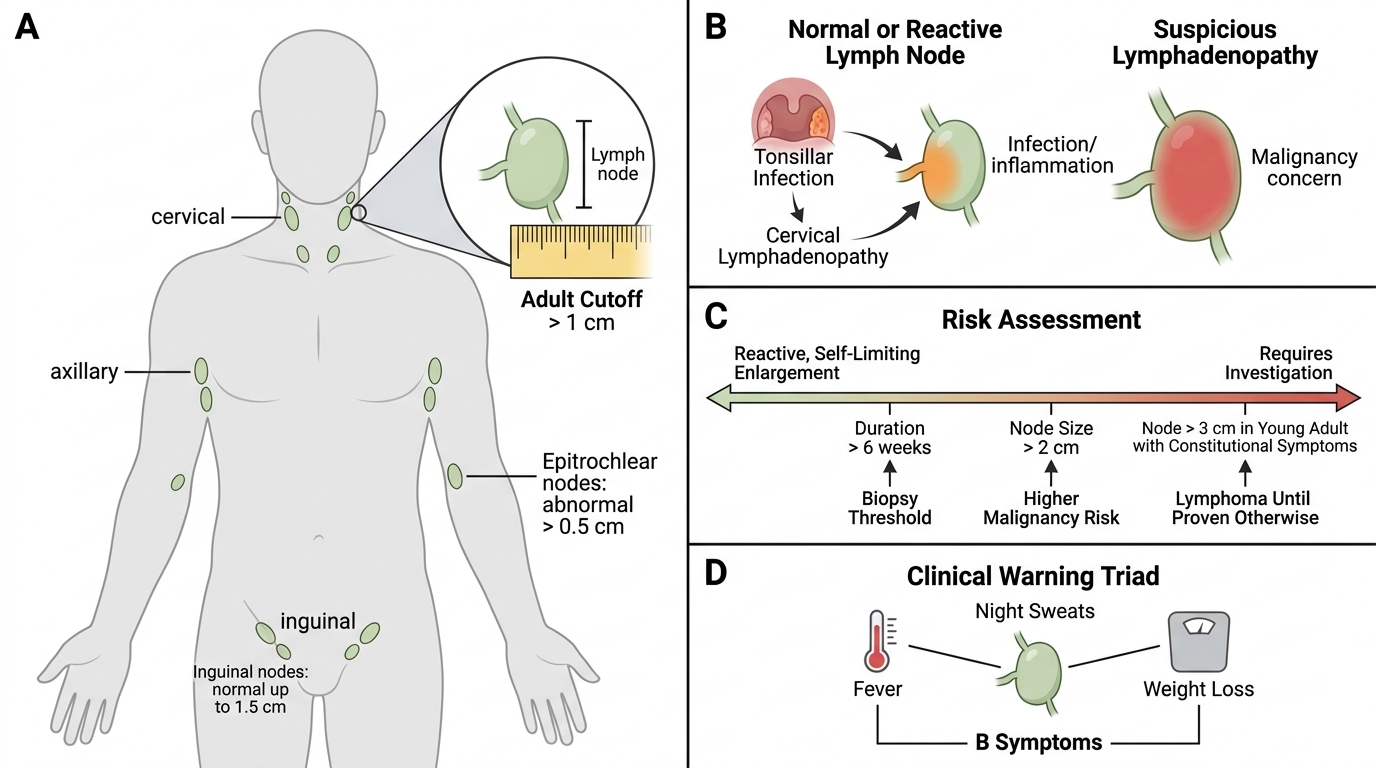
Lymphadenopathy is defined as enlargement of one or more lymph nodes beyond normal size limits:
- Adults: node > 1 cm in any axis (exception: inguinal nodes — up to 1.5 cm are normal; epitrochlear nodes > 0.5 cm are abnormal).
- Children: lymph nodes up to 2 cm in the cervical region may be reactive and normal.
Not all node enlargement is pathological. Reactive lymphadenopathy in response to a local infection (e.g., a tonsillar infection causing cervical lymphadenopathy) is normal immune physiology. The clinician's task is to decide when enlargement crosses from reactive/self-limiting to a process that demands investigation.
Key dimensions to assess:
1. Duration — > 6 weeks of unexplained persistent enlargement requires biopsy.
2. Size — nodes > 2 cm carry higher malignancy risk; nodes > 3 cm in a young adult with constitutional symptoms are flagged as lymphoma until proven otherwise.
3. Associated features — fever, night sweats, and weight loss ('B symptoms' in lymphoma staging) significantly raise malignancy suspicion.
Causes Framework: The Three-Tier Classification

Three-Tier Classification of Lymphadenopathy Causes
Organise causes under three tiers:
Tier 1 — Reactive / Benign
The node responds to a stimulus but retains normal architecture.
Infections — bacterial:
• Pyogenic (Staphylococcus, Streptococcus) — tender, fluctuant, localised.
• Tuberculous — matted, may caseate and collar-stud. See SDL2.
• Others: cat-scratch disease (Bartonella henselae), brucellosis, syphilis, plague.
Infections — viral:
• Infectious mononucleosis (EBV) — generalised, posterior cervical nodes; paracortical expansion.
• CMV, HIV (early stage — generalised persistent generalised lymphadenopathy, PGL).
Reactive hyperplasia without infection:
• Rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), Castleman disease.
Tier 2 — Neoplastic
The node's architecture is partly or wholly replaced by tumour.
Primary neoplasms of lymphoid tissue:
• Hodgkin lymphoma (HL) — bimodal age peak (15–34, > 55); rubbery, non-tender, often mediastinal.
• Non-Hodgkin lymphoma (NHL) — heterogeneous group; can be nodal or extranodal.
Secondary (metastatic) neoplasms:
• Carcinoma metastases — breast, lung, thyroid, GI, head-and-neck primaries drain to regional nodes. Stone-hard, fixed, irregular.
Tier 3 — Miscellaneous / Other
• Sarcoidosis — non-caseating granulomas; bilateral hilar + cervical/supraclavicular involvement.
• Dermatopathic lymphadenopathy — draining nodes in chronic skin disease (eczema, psoriasis).
• Drug-induced — phenytoin, allopurinol → generalised.
• Amyloidosis (secondary), storage disorders (Gaucher, Niemann-Pick).
SELF-CHECK
A 45-year-old woman with known rheumatoid arthritis presents with bilateral, soft, mildly tender axillary lymphadenopathy. Which reactive hyperplasia pattern is MOST likely to be seen on biopsy?
A. Sinus histiocytosis
B. Follicular hyperplasia
C. Paracortical hyperplasia
D. Granulomatous lymphadenitis
Reveal Answer
Answer: B. Follicular hyperplasia
Follicular hyperplasia is the signature of B-cell stimulation and is classically seen in autoimmune conditions (RA, SLE, early HIV) and bacterial infections. Follicles enlarge dramatically with prominent germinal centres. Paracortical hyperplasia (option C) reflects T-cell activation — typical of viral infections and drug reactions. Sinus histiocytosis (option A) is seen in draining nodes of carcinoma. Granulomatous pattern (option D) fits TB or sarcoidosis.
Reactive Hyperplasia Patterns — The Architectural Key

Reactive Hyperplasia Patterns in Lymph Nodes
Three morphological patterns of reactive change are recognised. Identifying the pattern narrows the aetiology before you even know the microbiology:
1. Follicular hyperplasia
Compartment: Cortex (B-cell zone)
Morphology: Enlarged, numerous secondary follicles with prominent, irregular, polarised germinal centres. Tingible-body macrophages (engulfing apoptotic lymphocytes) visible in germinal centres.
Aetiology: B-cell stimulation — RA, SLE, early HIV, Toxoplasma, bacterial infections.
Clinico-pathological hook: Germinal centre cells (centroblasts/centrocytes) can undergo malignant transformation → follicular lymphoma mimics this pattern grossly, but lacks tingible-body macrophages and shows bcl-2 positivity.
2. Paracortical (interfollicular) hyperplasia
Compartment: Paracortex (T-cell zone)
Morphology: Expansion of the T-cell zone with activated immunoblasts (large, pale nuclei, prominent nucleoli). Follicles compressed or absent.
Aetiology: T-cell stimulation — EBV (infectious mononucleosis), CMV, drug reactions (Dilantin/phenytoin), vaccinations.
Clinico-pathological hook: Dermatopathic lymphadenopathy (chronic skin disease) produces paracortical expansion with melanin-laden macrophages.
3. Sinus histiocytosis
Compartment: Medullary and subcapsular sinuses
Morphology: Distension of sinuses by proliferating macrophages (histiocytes). Node architecture otherwise preserved.
Aetiology: Drainage from carcinoma (regional nodes of breast, lung, bowel). The macrophages are responding to tumour antigens. Extreme form: Rosai-Dorfman disease (massive sinus histiocytosis with emperipolesis).
Clinico-pathological hook: Sinus histiocytosis in a cervical or axillary node should prompt a search for an ipsilateral primary carcinoma.

Reactive Hyperplasia Patterns in Lymph Nodes
CLINICAL PEARL
Follicular hyperplasia vs Follicular lymphoma — the key distinction:
Both show prominent follicles on low-power microscopy. Follicular hyperplasia has polarised germinal centres (dark/light zones), tingible-body macrophages, and varied follicle sizes. Follicular lymphoma has back-to-back follicles of uniform size, no tingible-body macrophages, bcl-2 positivity (t(14;18) translocation prevents apoptosis), and monotonous centrocytes. Always think: "is there apoptosis happening here?" — its absence in a follicular lesion is a red flag for malignancy.