Page 11 of 23
PA19.3 | Lymphomas — Hodgkin vs Non-Hodgkin — SDL Guide (Part 4)
Pathogenesis — Translocations, EBV, and Immunodeficiency
Major Pathogenetic Mechanisms in Lymphoma
Three pathogenetic mechanisms account for most lymphomagenesis:
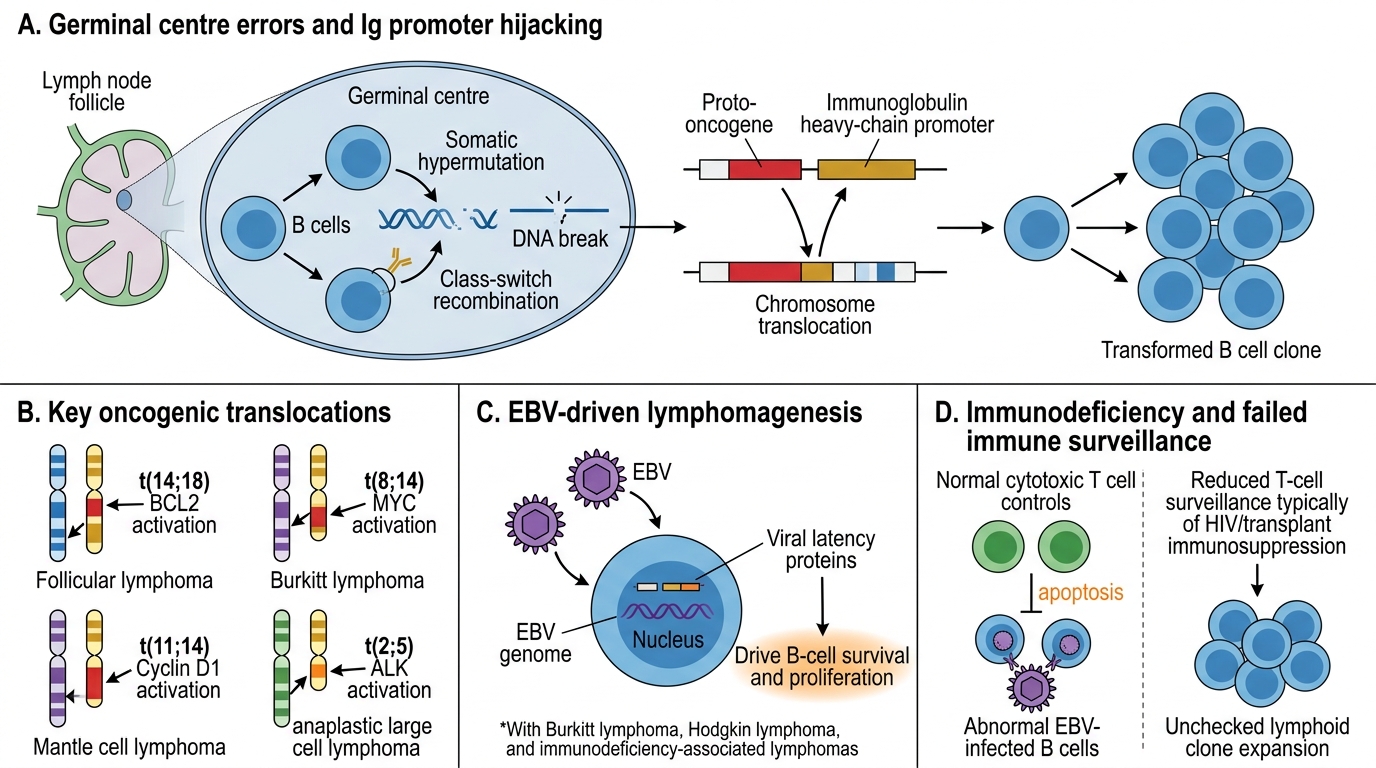
1. Oncogenic Translocations (Immunoglobulin Promoter Hijacking)
B-cell lymphomas exploit the somatic hypermutation and class-switch recombination machinery of the germinal centre. Errors during these physiological processes translocate proto-oncogenes next to constitutively active immunoglobulin gene promoters:
| Translocation | Gene deregulated | Lymphoma |
|---|---|---|
| t(14;18)(q32;q21) | BCL2 (anti-apoptotic) | Follicular lymphoma |
| t(8;14)(q24;q32) | MYC (proliferation) | Burkitt lymphoma |
| t(11;14)(q13;q32) | Cyclin D1 (cell-cycle) | Mantle cell lymphoma |
| t(2;5)(p23;q35) | ALK (signalling kinase) | ALCL (T-cell) |
2. EBV-Driven Oncogenesis
EBV infects B cells via CD21. In immunocompromised hosts, latent EBV proteins (LMP1, LMP2A) mimic CD40 and B-cell receptor signalling respectively, driving B-cell proliferation without normal antigenic stimulus. In HL, EBV infects the RS cell precursor and activates NF-κB, suppressing apoptosis.
3. Immunodeficiency
Normal immune surveillance identifies and eliminates EBV-infected, malignantly transformed B cells. HIV-related CD4 depletion, post-transplant immunosuppression, and congenital immunodeficiencies all remove this surveillance, dramatically increasing lymphoma risk — particularly EBV-driven NHLs (post-transplant lymphoproliferative disorder, primary CNS lymphoma in AIDS).
Diagnosis — Excision Biopsy and Immunohistochemistry

Excision Biopsy and IHC in Lymphoma Diagnosis
The diagnostic pathway for suspected lymphoma is standardised:
Step 1 — Excision Biopsy
The entire lymph node is removed intact. This preserves architecture (follicular vs diffuse pattern) and allows fresh tissue allocation for:
- Fixed sections → H&E morphology
- Frozen/fresh → flow cytometry (immunophenotyping of live cells)
- Cytogenetics/FISH → translocation detection
Step 2 — Immunohistochemistry (IHC) Panel
A minimum panel is applied to distinguish HL from NHL and determine NHL subtype:
| Marker | Significance |
|---|---|
| CD45 (LCA) | Pan-leucocyte; negative in classic RS cells |
| CD20 | B-cell marker; positive in most B-NHL and NLPHL |
| CD3 | T-cell marker |
| CD15, CD30 | Positive in cHL RS cells |
| CD10 | Germinal-centre marker; positive in FL, Burkitt, DLBCL-GCB |
| BCL2 | Anti-apoptotic; positive in FL (within follicles — key diagnostic feature) |
| Ki-67 | Proliferation index; ~100% in Burkitt, <20% in FL |
Cross-reference:
- H7 (CLL/SLL overlap): SLL is NHL territory — same clone, different site predominance
- H11 (Myeloma): Multiple myeloma is a plasma cell neoplasm — a post-germinal-centre B-cell malignancy; it is technically an NHL but is classified and managed separately