Page 2 of 12
PA19.4 | Splenomegaly — Causes & Differentiation — SDL Guide (Part 2)
Category 1 — Congestive Splenomegaly
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
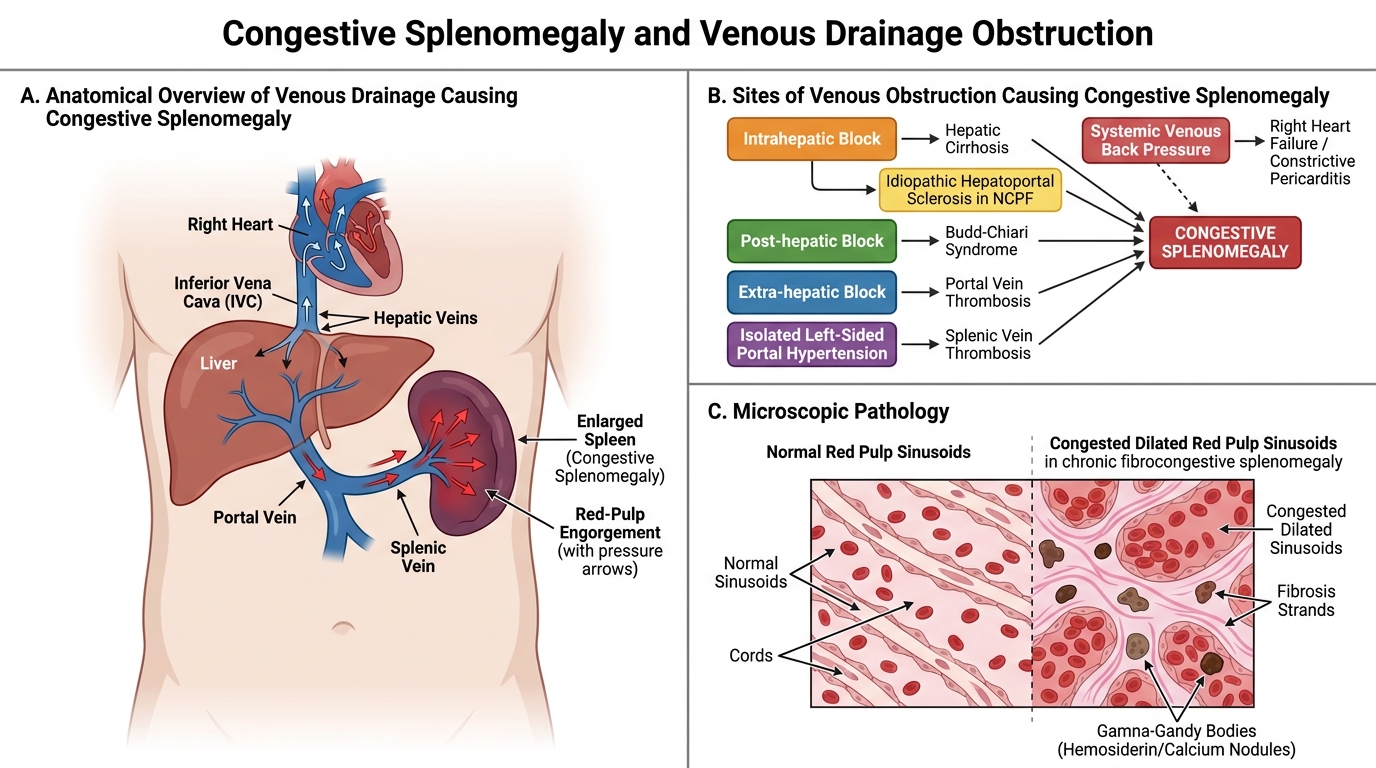
Congestive Splenomegaly: Venous Back Pressure and Red Pulp Congestion
Any condition that raises pressure in the portal or splenic venous system causes passive engorgement of the red pulp sinusoids.
Causes:
• Hepatic cirrhosis (commonest cause in India) — intrahepatic block → portal hypertension → splenomegaly. Associated with hypersplenism (see block 9).
• Non-cirrhotic portal fibrosis (NCPF) — idiopathic hepatoportal sclerosis; common in India; massive splenomegaly with relatively preserved liver function.
• Budd-Chiari syndrome — hepatic vein thrombosis → post-hepatic block.
• Portal vein thrombosis — extra-hepatic block; often presents in children.
• Splenic vein thrombosis — causes isolated 'sinistral' (left-sided) portal hypertension.
• Right heart failure / constrictive pericarditis — raised systemic venous pressure backs up through the inferior vena cava into the portal circulation.
Pathology: sinusoidal dilatation, red pulp congestion, fibrocongestive splenomegaly on chronicity (Gamna-Gandy bodies = haemosiderin/calcium deposits visible on MRI).
Category 2 — Infective Splenomegaly

Infective Splenomegaly: Mechanisms and Key Causes
Infections enlarge the spleen through two routes: (a) macrophage hyperplasia in response to phagocytosed organisms (red pulp expansion) and (b) immune/follicular hyperplasia in the white pulp.
Key pathogens:
- Malaria — Plasmodium parasites parasitise RBCs; macrophages in red pulp phagocytose parasitised cells and deposit malarial pigment (haemozoin). Chronic malaria → tropical splenomegaly syndrome (massive, reactive). Rupture risk in acute P. vivax.
- Kala-azar (visceral leishmaniasis, VL) — Leishmania donovani amastigotes multiply within red pulp macrophages → enormous macrophage expansion → massive splenomegaly (often the largest spleens in medicine; a hallmark of VL). Pancytopenia due to hypersplenism.
- Infective endocarditis — septic emboli seed the spleen; small multiple abscesses or reactive splenomegaly.
- EBV (infectious mononucleosis) — white pulp hyperplasia; atypical lymphocytes; risk of spontaneous splenic rupture (avoid contact sports for 4 weeks).
- Tuberculosis — miliary spread → discrete granulomas in white and red pulp; rarely causes massive splenomegaly.
- Typhoid — macrophage hyperplasia; typhoid nodules (collections of macrophages); spleen soft and prone to rupture.
Geography is a diagnostic clue: kala-azar (Bihar, Jharkhand, West Bengal — hyper-endemic belt); malaria (pan-India, seasonal).
SELF-CHECK
A 28-year-old man from Muzaffarpur (Bihar) has had fever, weight loss, and progressive abdominal distension for 8 months. Spleen reaches the right iliac fossa. Haemoglobin 6.8 g/dL, TLC 2.1 × 10⁹/L, platelets 55 × 10⁹/L. Bone marrow biopsy shows hypercellularity. The MOST likely diagnosis is:
A. Visceral leishmaniasis (kala-azar)
B. Chronic myeloid leukaemia
C. Thalassaemia major
D. Non-cirrhotic portal fibrosis
Reveal Answer
Answer: A. Visceral leishmaniasis (kala-azar)
Geography (Bihar hyper-endemic for Leishmania donovani), massive splenomegaly, pancytopenia, and hypercellular marrow (hypersplenism picture) are classic for kala-azar. CML would show leukocytosis and BCR-ABL. Thalassaemia major presents in childhood. NCPF rarely causes pancytopenia of this severity.
Category 3 — Haematological Splenomegaly

Haematological Splenomegaly: Infiltration vs Work Hypertrophy
Two distinct mechanisms operate here — infiltration by malignant cells, and work hypertrophy from haemolysis.
Myeloproliferative/Lymphoid infiltration:
• CML — neoplastic myeloid progenitors home to the spleen and proliferate; splenic extramedullary haematopoiesis compounds this. Spleen may reach 3–5 kg — the classic cause of massive splenomegaly in haematological malignancy. Cross-ref Cluster H7.
• Myelofibrosis (Primary myelofibrosis) — progressive marrow fibrosis drives haematopoiesis entirely to the spleen and liver (myeloid metaplasia); massive splenomegaly + leukoerythroblastic blood film.
• Lymphomas and leukaemias — NHL (especially splenic marginal zone lymphoma), CLL, hairy cell leukaemia, ALL — all infiltrate white and/or red pulp. Cross-ref Cluster H8.
Haemolytic work hypertrophy:
• Thalassaemia major — massive ineffective erythropoiesis in the marrow + extramedullary haematopoiesis in spleen → progressive splenomegaly. Splenectomy deferred as long as possible (removes residual haematopoietic reserve).
• Hereditary spherocytosis (HS) — spherocytes fail to traverse slit pores → trapped and destroyed in red pulp; spleen hyperplastic. Splenectomy is curative.
• Autoimmune haemolytic anaemia (AIHA) — IgG-coated RBCs destroyed in spleen (Fc-receptor-mediated); moderate splenomegaly.
• ITP — anti-platelet IgG; platelet destruction in spleen; spleen may be normal or mildly enlarged (important: splenomegaly in ITP is mild at most — a massively enlarged spleen in thrombocytopenia should suggest another diagnosis).
Cross-ref H5 (thalassaemia, HS, AIHA) and H7 (CML, myelofibrosis).