Page 5 of 13
PS1.2-3 | Psychiatric History and Mental Status Examination — SDL Guide
Learning Objectives
- Demonstrate the ability to elicit a structured psychiatric history from a patient presenting with a psychiatric disorder
- Perform a systematic mental status examination (MSE) covering all eight domains
- Interpret key MSE findings and relate them to common psychiatric diagnoses
- Apply ethical and communication principles in conducting psychiatric interviews
INSTRUCTIONS
The psychiatric history and mental status examination are the two indispensable clinical skills of psychiatry — together they constitute what a physical examination and ECG are to cardiology. Unlike most medical specialties, psychiatry has no single biomarker or imaging test that clinches a diagnosis: the clinician's interaction with the patient IS the primary diagnostic instrument. Mastering these skills will make you a more competent clinician across every specialty, because patients with psychiatric comorbidity are encountered in every ward, clinic, and emergency department.
References
- Ahuja N. A Short Textbook of Psychiatry, 8th ed., Ch. 3 & 4 (textbook)
- Kaplan & Sadock's Synopsis of Psychiatry, 12th ed., Ch. 5 (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
You are the intern on duty in the psychiatry emergency. A young man, approximately 25 years old, is brought in by his mother. He has not slept for four days, is speaking very fast, jumps from topic to topic, claims he has been chosen by God to deliver an important message to the Prime Minister, and has been giving away his belongings to strangers. His mother is terrified. In the next 30 minutes, you need to establish rapport, take a focused but comprehensive history, and perform a mental status examination to frame a working diagnosis and initiate management. There is no blood test to confirm bipolar disorder. Your interaction with this patient — how you ask questions, what you observe, how you systematically document what you find — is both the diagnostic test and the therapeutic beginning.
WHY THIS MATTERS
The psychiatric history and mental status examination are not specialty-specific niche skills — they are core competencies for every medical graduate. Patients with depression, anxiety, psychosis, and substance use disorders present to general medicine, neurology, obstetrics, paediatrics, and emergency medicine at least as often as to psychiatry clinics. The ability to screen for suicide risk, recognise a first episode of psychosis, identify alcohol withdrawal, or diagnose delirium in a postoperative patient can be life-saving. Moreover, the communication skills underlying a good psychiatric interview — active listening, non-judgemental questioning, empathy, containment of distress — are the same skills that differentiate a good clinician from an average one in every specialty.
RECALL
From your medicine and surgery postings, you will have taken medical histories and performed physical examinations. The psychiatric history follows a similar structure but with important differences: the informant is often a family member (because the patient may lack insight), the timeline of symptom onset and course is more complex (mood disorders can be episodic over years), and psychological stressors, premorbid personality, and family psychiatric history are as diagnostically important as physical examination findings. You also have prior knowledge of neuroanatomy — the limbic system (hippocampus, amygdala, anterior cingulate cortex) is central to emotion regulation; the prefrontal cortex governs executive function and impulse control; the striato-thalamo-cortical circuits are implicated in OCD; and the mesolimbic dopamine pathway is central to psychosis.
Clinical Indications and the Therapeutic Frame of the Psychiatric Interview
The psychiatric interview is indicated whenever a patient presents with symptoms or behaviours that suggest a disturbance in thinking, mood, perception, behaviour, or cognition — regardless of the clinical setting. While routine psychiatric referrals to an outpatient clinic are one context, the interview is also critically indicated in: a general medicine patient with unexplained somatic complaints disproportionate to identified pathology; a patient presenting to an emergency department following a self-harm or overdose; a patient who refuses a medically necessary intervention and whose decision-making capacity needs assessment; a postoperative patient who develops acute confusion (possible delirium); a pregnant or postpartum woman with depressive, anxious, or psychotic symptoms; and any patient whose physical illness is compounded by psychological distress that is impeding recovery.
Provided image
The therapeutic frame of the psychiatric interview differs from a standard medical history in one fundamental respect: the process of the interview is itself therapeutic. By asking thoughtful, open questions, demonstrating genuine curiosity about the patient's experience, and maintaining a non-judgemental stance, the clinician communicates that the patient's mental experience is legitimate, worthy of attention, and amenable to help. This is particularly important because patients with psychiatric disorders often present to medical services after years of their symptoms being dismissed, stigmatised, or attributed to weakness of character. A well-conducted interview can reduce a patient's shame, increase their willingness to disclose, and improve therapeutic engagement — all of which directly affect treatment outcomes.
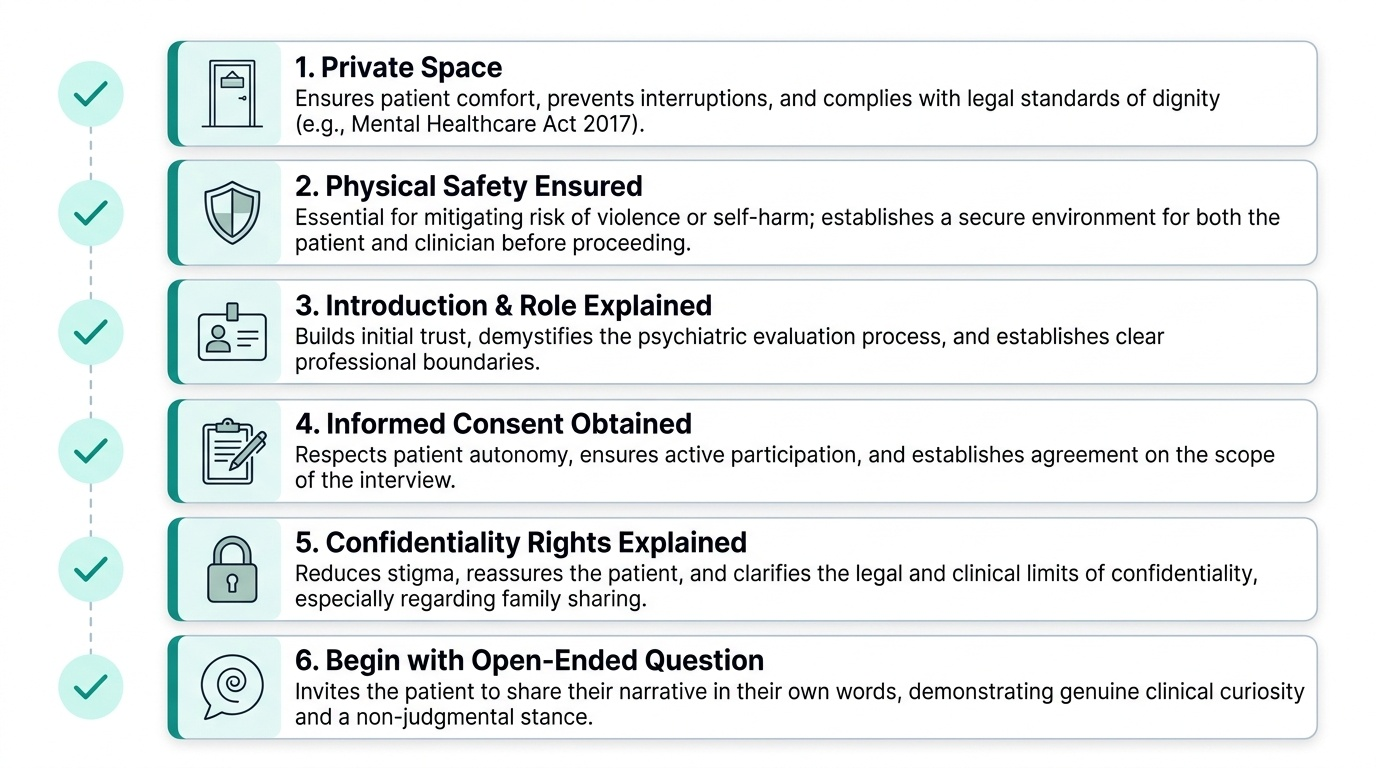
Practical preconditions for a good psychiatric interview include: a private, quiet space free from interruptions (this is a non-negotiable requirement under the Mental Healthcare Act 2017); ensuring the patient's physical safety (if there is a risk of violence or self-harm, appropriate precautions must be in place before proceeding); introducing yourself clearly and explaining your role; obtaining informed consent for the interview and for any information-sharing with family members (bearing in mind the patient's right to confidentiality even from family under the 2017 Act); and beginning with open-ended questions ('Can you tell me what has been troubling you?' rather than 'Do you hear voices?').
Governing Principles of the Psychiatric Interview
Several foundational principles govern the psychiatric interview and distinguish it from the structured, closed-question format that may be more familiar from physical medicine consultations. These principles are not merely courtesies — they directly affect the quality of the diagnostic information obtained and the patient's willingness to engage with treatment.
Principle 1: Begin with open-ended, then funnel to closed questions. Start with a broad invitation ('Tell me what has been happening' or 'What brings you here today?') and allow the patient to narrate in their own words. Only after the patient has offered their narrative should you direct the interview toward specific symptom areas. This 'open → specific → closed' funnel yields richer clinical information than a checklist-based approach because it allows the patient to introduce topics the clinician might not have anticipated.
Principle 2: Active listening and empathic attunement. Active listening is not passive waiting — it involves verbal acknowledgements ('I understand,' 'Please go on'), reflection ('So what you are saying is...'), and appropriate emotional validation ('That sounds like a very frightening experience'). Empathy does not mean agreeing with the patient's delusional beliefs — it means communicating that you understand the patient's distress and take it seriously, while maintaining your clinical objectivity.
Principle 3: Non-judgemental stance. Patients with psychiatric disorders — particularly those involving substance use, self-harm, or suicidal ideation — often anticipate being judged or criticised. A non-judgemental approach ('I'm going to ask you some questions that we ask everyone who comes with these kinds of difficulties — please feel free to answer as openly as you can') normalises sensitive disclosures and reduces the risk of underreporting.
Principle 4: Safety assessment must be explicit and non-deferred. Suicidal ideation, intent, and plan must be asked about directly in every psychiatric interview. There is a common clinical myth that 'asking about suicide will plant the idea' — this has been conclusively refuted by research. Asking about suicidal ideation does not increase suicide risk and may relieve the patient's sense of isolation. The assessment of suicidal ideation (passive wish to be dead vs. active thoughts of killing oneself), intent (does the patient intend to act on these thoughts?), plan (has a specific method been considered?), means (does the patient have access to the intended means?), and protective factors (family, religion, children, future plans) constitutes the risk stratification that determines the urgency of the clinical response.
Principle 5 — Collateral history is essential: Because insight is impaired in psychotic and manic states, and because a patient's account of their own behaviour may be distorted by the illness, information from a reliable family member or caregiver is often indispensable. The clinician should explain to the patient that they will also speak to a family member and seek the patient's permission — except in situations where the patient lacks decision-making capacity or the collateral history is urgently required for safety.
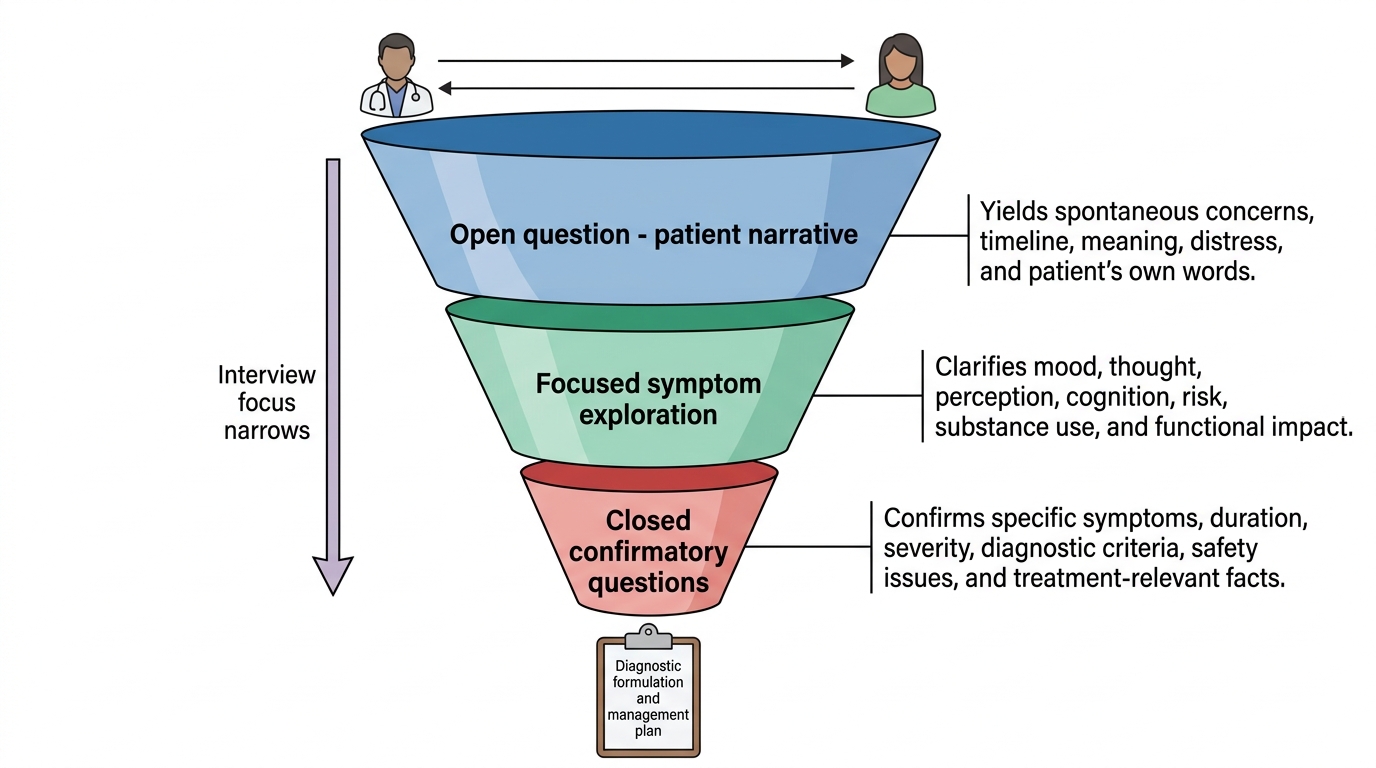
Open-to-Closed Questioning Funnel in Psychiatric Interviews
Eliciting the Psychiatric History: Structure and Content
The psychiatric history is typically structured across the following domains, each of which contributes essential information to the diagnostic formulation. The order below reflects the standard sequence taught in Ahuja's textbook and commonly used in Indian psychiatric practice, though experienced clinicians adapt this flexibly to each patient.
1. Identifying data and referral source: Name, age, sex, education, occupation, marital status, religion, socioeconomic background, who referred the patient and why. These data contextualise the clinical presentation and are relevant to treatment planning (e.g. occupational impact of symptoms, economic barriers to medication).
2. Chief complaint in the patient's own words: Quote the patient verbatim where possible ('He says the television is sending messages to him specifically'). Determine who considers this a complaint — the patient, the family, or society.
3. History of presenting illness (HPI): This is the most critical section. Explore: onset (sudden, gradual, precipitant — a psychosocial stressor? a substance? a postpartum period?); duration (apply the relevant diagnostic duration criteria); course (continuous, episodic, deteriorating, improving?); severity (impact on functioning — work, relationships, self-care); associated symptoms across all psychiatric domains (mood, perception, thought content, cognitive function, sleep, appetite, libido, energy, psychomotor activity); and any prior treatment received. For each positive symptom, explore its first occurrence, frequency, and variability.
4. Past psychiatric history: Any previous episodes of the same or different psychiatric illness; hospitalisations; treatments received (medications, psychotherapy, ECT) and their response; any previous suicide attempts (method, severity, treatment received, and the patient's current attitude toward the attempt).
5. Past medical and surgical history: Chronic medical conditions (particularly neurological, endocrine, and systemic diseases); medications (many drugs cause psychiatric symptoms — steroids, beta-blockers, antihypertensives, anticonvulsants, antimalarials); surgeries and anaesthetics; head injuries.
6. Family history: First-degree psychiatric illness (schizophrenia, bipolar disorder, major depression, OCD, suicide) — family history is a major risk factor for most primary psychiatric disorders and is relevant to genetic counselling.
7. Personal history: Prenatal and birth history (obstetric complications); developmental milestones; schooling and academic performance; occupational history; relationship and sexual history; marital and parenting history; forensic history (legal difficulties, which may be sequelae of psychiatric illness or substance use).
8. Psychosexual history: Where clinically relevant, explore sexual development, orientation, and any sexual dysfunction (which may be a symptom of depression or an adverse effect of psychotropic medication).
9. Substance use history: Systematically screen for use of tobacco (amount, duration), alcohol (quantity, frequency, CAGE questions), cannabis, opioids, stimulants, sedative-hypnotics, and any other substances. For each substance: age of first use, current use pattern, features of dependence (loss of control, withdrawal, tolerance, continued use despite harm).
10. Premorbid personality: What was the patient like BEFORE this illness? This is best obtained from a reliable informant. Premorbid personality informs the differential diagnosis (e.g. premorbid schizotypal traits may predispose to schizophrenia; premorbid perfectionism and conscientiousness may be a risk factor for OCD).
- Socioeconomic and cultural context: Living situation, financial resources, social support network, religious beliefs and practices (particularly where beliefs may be relevant to the assessment of delusions), and cultural attitudes toward psychiatric illness and its treatment.
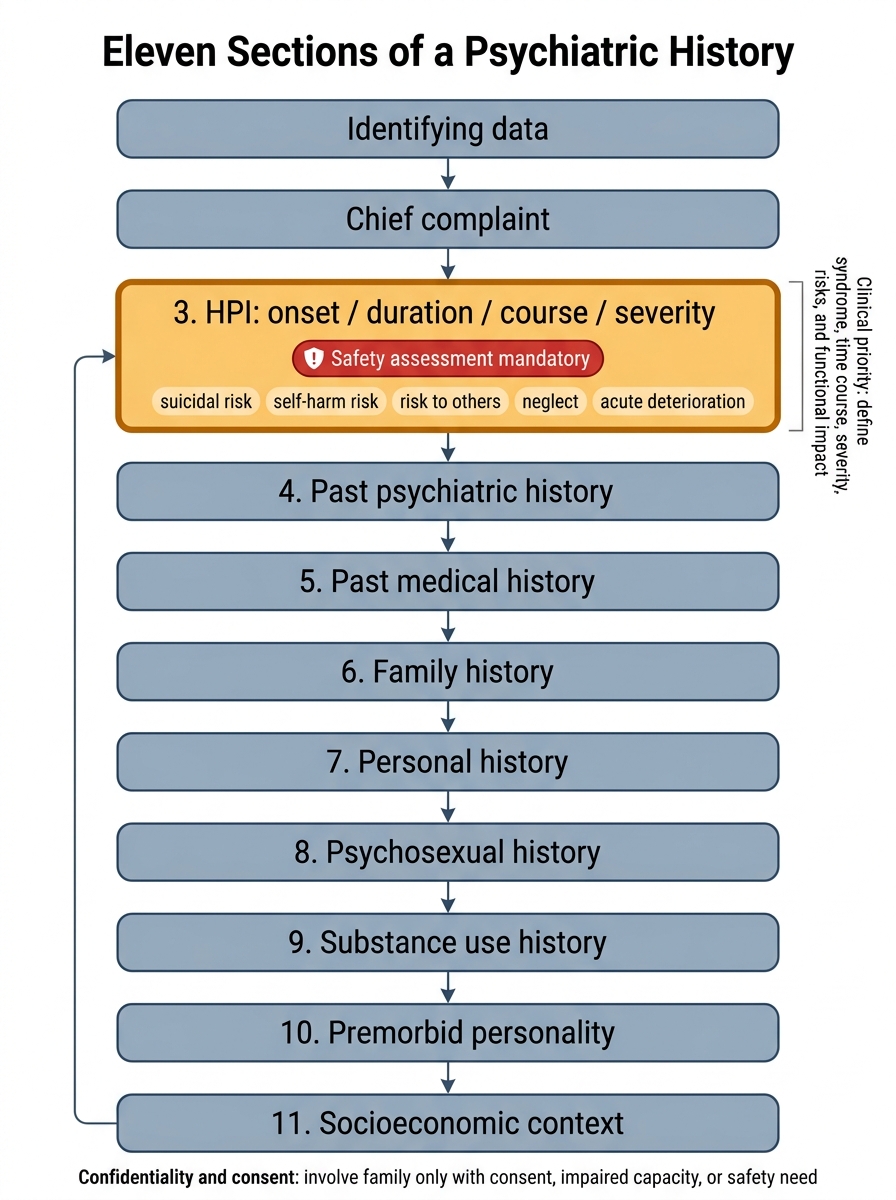
Eleven Sections of a Psychiatric History
SELF-CHECK
During a psychiatric history, a 22-year-old woman with a first episode of apparent psychosis tells you she prefers you not to speak to her family. Which is the most appropriate response under the Mental Healthcare Act 2017?
A. Proceed to speak with the family immediately — psychiatric patients cannot make valid consent decisions
B. Respect her preference and do not involve the family unless she lacks decision-making capacity or safety requires it
C. Involve the family as this is standard of care for first-episode psychosis
D. Document her preference but involve the family anyway, as collateral history is clinically necessary
Reveal Answer
Answer: B. Respect her preference and do not involve the family unless she lacks decision-making capacity or safety requires it
Under the Mental Healthcare Act 2017, persons with mental illness retain the right to confidentiality, including with respect to family members, unless they lack decision-making capacity or safety requires disclosure. A first episode of psychosis does not automatically remove decision-making capacity — capacity must be formally assessed. If the patient has capacity, her preference not to involve her family must be respected, except in a genuine safety emergency. Document the patient's preference clearly.