Page 7 of 13
PS1.2-3 | Psychiatric History and Mental Status Examination — SDL Guide (Part 3)
Self-Assessment and Consolidation
Having worked through the full arc of the psychiatric history and MSE — from the indications and principles of the interview, through the structured content of the history, to the eight MSE domains and their clinical interpretation — you should now be equipped to approach a psychiatric patient with systematic confidence. This section consolidates the key frameworks and tests your ability to integrate them.
The psychiatric history follows a standard structure: identifying data → chief complaint → HPI (onset, duration, course, associated symptoms) → past psychiatric history → past medical history → family history → personal and developmental history → substance use history → premorbid personality → socioeconomic and cultural context. The most critical section is the HPI, within which suicidal ideation and safety must be explicitly assessed in every patient.
The MSE must cover all eight domains in every assessment. The mnemonic domains are: Appearance and Behaviour → Speech → Mood and Affect → Thought (Form, Content, Possession) → Perception → Cognition → Insight → Judgement. Each domain has specific clinical descriptors, and abnormal findings must be documented with specific examples rather than vague category labels.
The pattern-recognition approach to MSE interpretation allows you to map clusters of findings to diagnostic categories: pressured speech + flight of ideas + grandiosity + decreased need for sleep = manic episode; auditory third-person hallucinations + loosening of associations + blunted affect + thought broadcasting = schizophrenia; visual hallucinations + disorientation + fluctuating consciousness = delirium (organic); psychomotor retardation + low mood + worthlessness + suicidal ideation = major depressive episode. These patterns are not diagnostic short-cuts — they are evidence-based anchors that guide further assessment.
Suicide risk assessment is a mandatory competency within the psychiatric interview: assess ideation (passive vs. active), intent, plan, access to means, and protective factors. Any patient with active suicidal intent and a specific plan requires immediate safety measures including assessment for psychiatric admission under the Mental Healthcare Act 2017.
The application of these skills in clinical settings is developed through supervised practice with real patients under faculty observation. The ability to conduct a comprehensive psychiatric interview and MSE, synthesise the findings into a formulation, and communicate this clearly in case notes and ward rounds is the core clinical skill set of the graduating MBBS student in psychiatry.
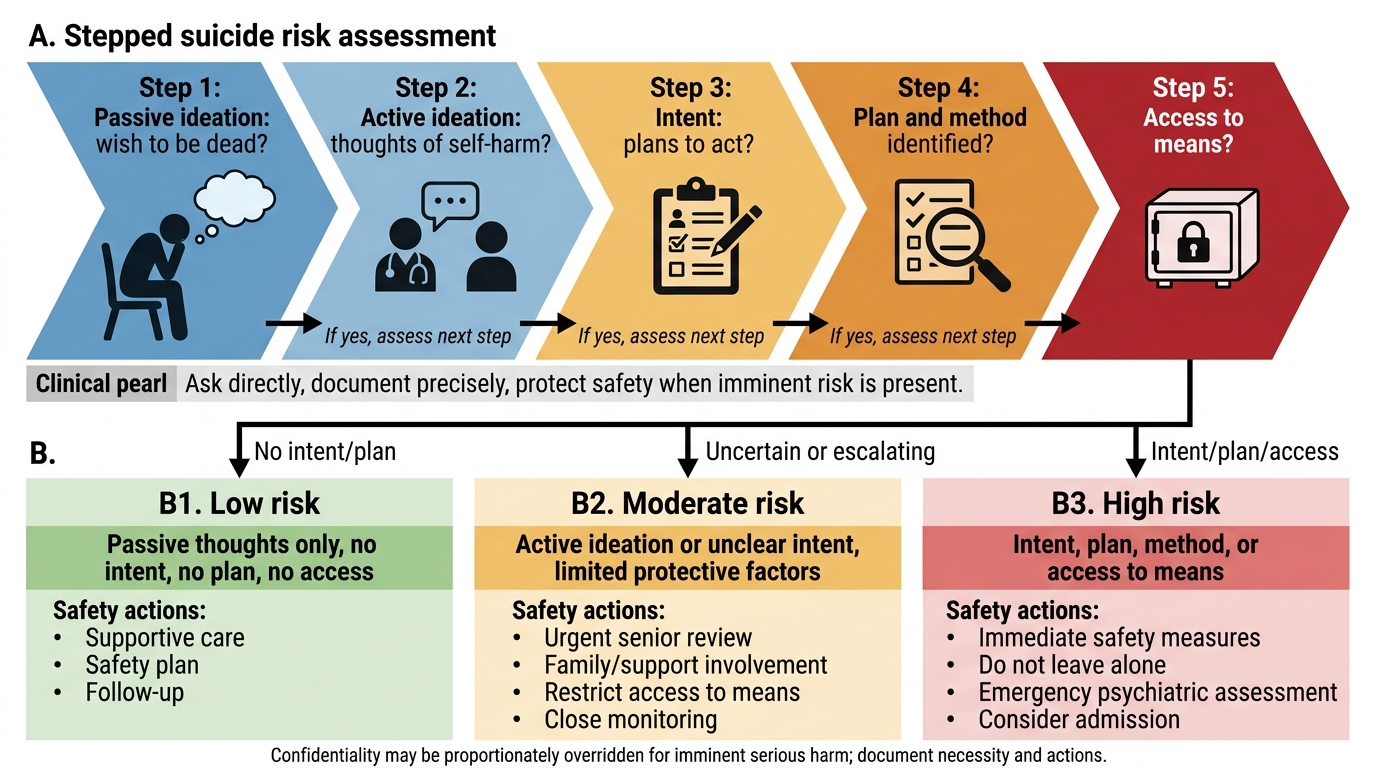
Stepped Suicide Risk Assessment Algorithm
CLINICAL PEARL
The single most important safety question in any psychiatric interview is the direct assessment of suicidal risk — and it must never be omitted. Use a graduated approach: 'Sometimes when people feel as distressed as you have been describing, they have thoughts of not wanting to be alive — have you had any such thoughts?' If the patient says yes, move to active ideation: 'Have you thought about actually harming yourself or ending your life?' If yes, assess the plan: 'Do you have a specific plan in mind? Have you thought about how you would do it?' Each step narrows the risk level. Document your findings precisely. Remember: the legal and ethical duty to protect patient safety may override confidentiality obligations where there is imminent risk of serious harm — but the Mental Healthcare Act 2017 mandates that this override is proportionate, necessary, and documented.