Page 2 of 8
PS4.1 | Schizophrenia at Primary Care Level — SDL Guide (Part 2)
Management at Primary Care Level
Management of schizophrenia at primary care encompasses pharmacological treatment, psychosocial intervention, family psychoeducation, safety planning, and timely specialist referral. The primary care physician's role is not to provide complete tertiary psychiatric care but to initiate evidence-based treatment, support the patient and family through the first critical weeks, and establish an ongoing relationship that facilitates adherence and early detection of relapse.
Provided image
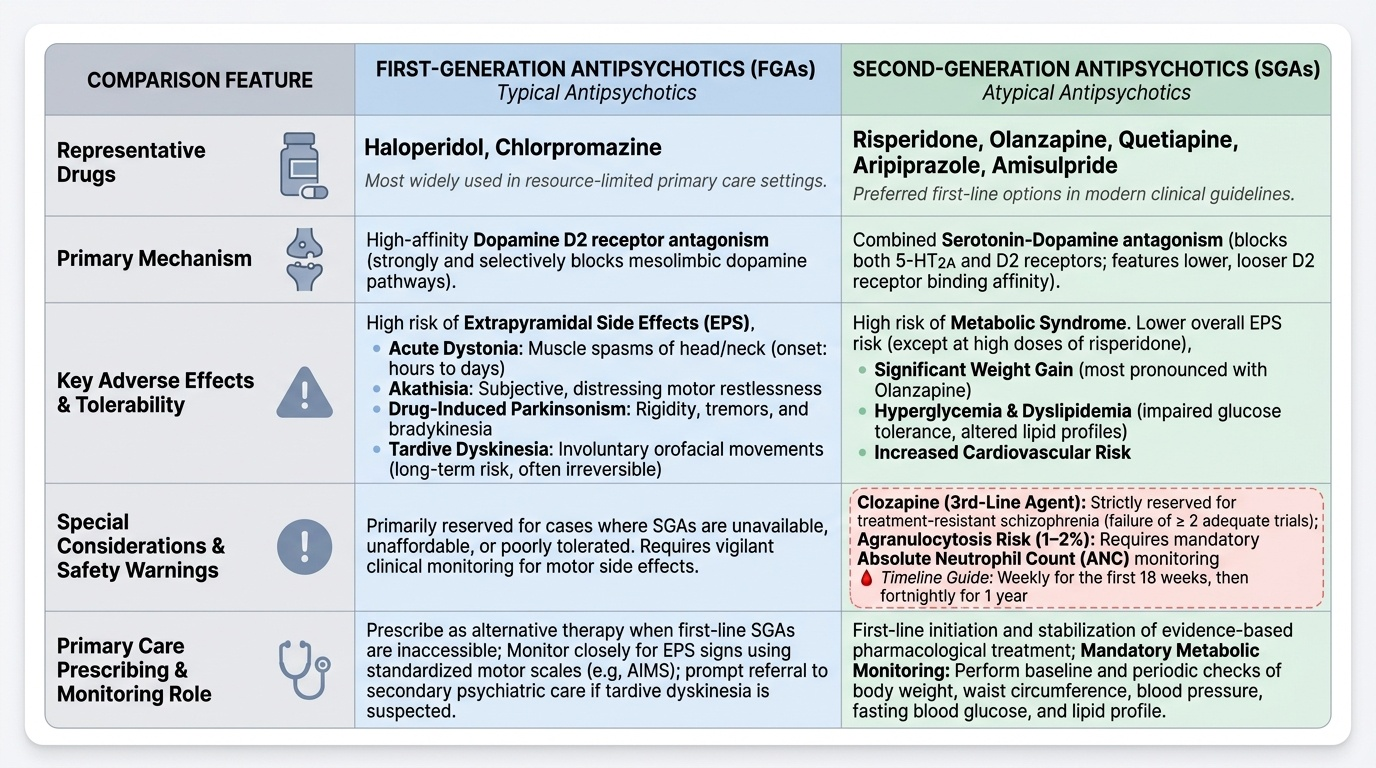
Pharmacological management — antipsychotic therapy:
The first-line pharmacological treatment for schizophrenia is an atypical (second-generation) antipsychotic (SGA). Commonly available first-line SGAs include risperidone, olanzapine, quetiapine, aripiprazole, and amisulpride. SGAs are preferred over typical (first-generation) antipsychotics (FGAs) as first-line because they carry a lower risk of extrapyramidal side effects (EPS) — though they are not entirely free of EPS, particularly at higher doses or with risperidone.
Typical (first-generation) antipsychotics — haloperidol and chlorpromazine being the most widely used in primary care settings — remain effective and may be used where SGAs are unavailable or unaffordable. Their principal limitation is a higher burden of EPS: acute dystonia (sustained muscle spasm, typically within hours to days of initiation), akathisia (subjective restlessness, a common cause of non-adherence), drug-induced parkinsonism (bradykinesia, rigidity, tremor), and tardive dyskinesia (involuntary orofacial and choreiform movements after prolonged use — often irreversible).
Atypical antipsychotics carry a different adverse effect profile, most notably metabolic syndrome — weight gain, hyperglycaemia, dyslipidaemia, and increased cardiovascular risk. This is most pronounced with clozapine and olanzapine. All patients on SGAs require baseline and periodic monitoring of weight, fasting glucose, and lipid profile.
Clozapine is a third-line agent reserved exclusively for treatment-resistant schizophrenia (failure of at least two adequate antipsychotic trials). It is the most effective antipsychotic available but carries a risk of agranulocytosis (1–2% of patients), which is potentially fatal and requires mandatory monitoring of the absolute neutrophil count (ANC) — weekly for the first 18 weeks, then fortnightly for one year, then monthly thereafter. Clozapine should NEVER be initiated at primary care without specialist supervision, and a definitive baseline ANC must be confirmed before starting.
Neuroleptic Malignant Syndrome (NMS) is a rare but life-threatening emergency that can occur with any antipsychotic. It is characterised by the tetrad of hyperthermia (fever), generalised lead-pipe muscular rigidity, autonomic instability (tachycardia, labile blood pressure, diaphoresis), and elevated serum creatine kinase (CK). NMS must be distinguished from serotonin syndrome — which presents with hyperreflexia, myoclonus, clonus (not lead-pipe rigidity), rapid onset (within hours), and a history of serotonergic agents rather than antidopaminergic drugs. If NMS is suspected, immediately discontinue the offending antipsychotic, provide supportive care, and arrange emergency referral.
Psychosocial management:
Pharmacological treatment alone is insufficient for full recovery. Family psychoeducation — providing the family with accurate information about the nature of schizophrenia, its course, medication benefits and side effects, and relapse warning signs — is the single most evidence-backed psychosocial intervention and substantially reduces relapse rates. Assertive community treatment (ACT) or community mental health team involvement should be arranged at the earliest opportunity. Cognitive Behavioural Therapy for Psychosis (CBTp) is effective for residual symptoms and is available at tertiary centres.
When to refer (primary care decision points):
1. First presentation with suspected psychosis — refer to psychiatry after initial assessment and stabilisation
2. Treatment failure after an adequate first-line trial (at least 4–6 weeks at adequate dose)
3. Suicidality or significant risk to self or others
4. Diagnostic uncertainty (especially when ruling out bipolar disorder or organic cause is complex)
5. Need for clozapine — mandatory specialist initiation and monitoring
6. Significant comorbid substance misuse requiring dual-diagnosis management
Follow-up at primary care: Once stabilised on medication and under specialist care, primary care plays a vital ongoing role: monitoring metabolic parameters, identifying early relapse signs, supporting medication adherence, managing intercurrent physical illnesses, and maintaining the therapeutic relationship with the patient and family.
SELF-CHECK
A patient on haloperidol for 6 months develops involuntary, repetitive chewing and tongue-rolling movements. What is the most likely diagnosis, and what is the most critical next step?
A. Acute dystonia; administer intramuscular benztropine immediately
B. Tardive dyskinesia; review the need for continued haloperidol and consider switching to an atypical antipsychotic after specialist consultation
C. Neuroleptic Malignant Syndrome; stop haloperidol and arrange emergency admission
D. Drug-induced parkinsonism; add levodopa to the regimen
Reveal Answer
Answer: B. Tardive dyskinesia; review the need for continued haloperidol and consider switching to an atypical antipsychotic after specialist consultation
Involuntary orofacial movements (chewing, tongue rolling, lip smacking) appearing after months to years of antipsychotic use are characteristic of tardive dyskinesia (TD) — a late-onset, often irreversible extrapyramidal side effect most associated with first-generation antipsychotics like haloperidol. The critical next step is to review whether the lowest effective dose can be used or the patient switched to an atypical antipsychotic (which carries lower TD risk) after specialist consultation. Acute dystonia presents early (hours to days) as sustained muscle spasm treated with anticholinergics (benztropine). NMS presents with fever, lead-pipe rigidity, and autonomic instability. Parkinsonism presents as bradykinesia, rigidity, and tremor — NOT involuntary orofacial movements — and levodopa is inappropriate for drug-induced parkinsonism.
CLINICAL PEARL
The 'treatment gap' trap: In India, the majority of patients with schizophrenia have never received any psychiatric treatment — the 'treatment gap' for schizophrenia exceeds 70%. As a primary care physician you will often encounter patients who have been ill for years without diagnosis, managed with traditional or faith-based care, or who relapsed because a prior treating physician abruptly stopped medication after symptom remission. Three rules prevent the most common primary-care errors: (1) Never stop antipsychotics abruptly — taper under specialist guidance; (2) Educate families that remission is NOT cure — maintenance therapy for at least 1–2 years after a first episode, and potentially lifelong after multiple episodes, is the current evidence-based recommendation; (3) NMS is a clinical emergency — if you see the tetrad of fever, lead-pipe rigidity, autonomic instability, and raised CK in a patient on any antipsychotic, stop the drug immediately and transfer to a higher centre. Do not wait for CK results before stopping.
Self-Assessment and Consolidation
Congratulations on completing this module. Before you proceed to the self-assessment questions below, take a moment to consolidate your learning by revisiting the key clinical decision points for schizophrenia at primary care. You have journeyed through the characteristic presentation of schizophrenia — the positive symptoms (delusions, hallucinations, thought disorder), negative symptoms (the 5As: avolition, alogia, anhedonia, affective flattening, asociality), and cognitive impairments — and you now understand why each cluster has distinct functional implications and treatment responses.
You have grounded your diagnostic reasoning in both ICD-11 (core symptoms ≥1 month) and DSM-5 (total duration ≥6 months including prodrome, with active phase ≥1 month) criteria, and you understand why this distinction matters in clinical communication and medico-legal contexts under the Mental Healthcare Act 2017. The Mental Status Examination — from appearance and speech through thought content, perception, cognition, and insight — is the systematic tool that transforms your clinical observations into a defensible diagnostic formulation.
In pharmacological management, you have established that atypical (second-generation) antipsychotics are the first-line treatment choice at primary care. You understand the contrasting adverse effect profiles: typical antipsychotics carry the burden of EPS (acute dystonia, akathisia, parkinsonism, tardive dyskinesia); atypical antipsychotics carry the burden of metabolic syndrome (weight gain, hyperglycaemia, dyslipidaemia) — most pronounced with clozapine and olanzapine. You have learned that clozapine is reserved for treatment-resistant schizophrenia, requires mandatory ANC monitoring (due to agranulocytosis risk), and must never be initiated at primary care without specialist supervision. You can now recognise Neuroleptic Malignant Syndrome (fever + lead-pipe rigidity + autonomic instability + raised CK) as a psychiatric emergency and distinguish it from serotonin syndrome (hyperreflexia, myoclonus, clonus, rapid onset, serotonergic agent history).
Finally, you appreciate that effective primary-care management of schizophrenia extends well beyond prescribing: family psychoeducation, adherence support, metabolic monitoring, early recognition of relapse, and timely specialist referral are the pillars of a comprehensive primary-care plan.
Self-assessment reflection questions:
1. A 28-year-old woman presents with 8 months of auditory hallucinations and persecutory delusions with no period of full remission. Which diagnostic category best fits under DSM-5, and what is your next management step?
2. Your patient on olanzapine has gained 8 kg in 3 months and his fasting glucose is 7.2 mmol/L. What monitoring should you have initiated at the start of treatment, and what action should you take now?
3. A patient on haloperidol develops fever of 39.5°C, generalised muscle rigidity, and blood pressure that keeps swinging. His CK comes back at 4,500 U/L. What is your diagnosis and what must you do immediately?