Page 4 of 11
PS8.1 | Stress Related Disorders Referral — SDL Guide
Learning Objectives
- Describe the clinical features of Acute Stress Disorder (ASD), Post-Traumatic Stress Disorder (PTSD), and Adjustment Disorder
- Apply DSM-5 and ICD-11 diagnostic criteria, explicitly attributing duration thresholds to their classification system
- Construct a timeline-based differential that distinguishes ASD from PTSD from Adjustment Disorder
- Identify the neurobiological and psychological mechanisms underlying trauma-related disorders
- Formulate an appropriate management plan including psychological first aid, trauma-focused CBT, and pharmacotherapy when indicated
- Apply referral criteria to decide when a primary care physician should escalate to secondary psychiatric services
INSTRUCTIONS
Every general practitioner will encounter patients who have experienced traumatic or stressful events — road traffic accidents, natural disasters, domestic violence, workplace accidents, bereavement. The critical skill is knowing whether the patient's reaction is a normal human response or a disorder requiring intervention, and whether that intervention can stay in primary care or must be referred. NMC competency PS8.1 requires you to diagnose both Acute Stress Disorder and Adjustment Disorder and make appropriate referral decisions — a competency tested in clinical postings and in MBBS assessment.
References
- Ahuja N. A Short Textbook of Psychiatry, 8th ed. Jaypee Brothers, 2022. Ch. 8: Stress-Related and Trauma-Related Disorders (textbook)
- Kaplan & Sadock's Synopsis of Psychiatry, 12th ed. Wolters Kluwer, 2022. Ch. 14: Trauma- and Stressor-Related Disorders (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
Clinical scenario: It is 3 weeks after a major road traffic accident in which a 27-year-old bus driver narrowly survived when his vehicle overturned. He was not physically injured but witnessed a passenger die. He now presents to your PHC with inability to sleep, recurring vivid images of the accident 'appearing in my mind like a film,' extreme startle response to any vehicle horn, emotional numbness, and avoidance of bus stands. He tells you his wife says he has 'changed completely.' He broke down during the interview and said he has been dreaming about the accident every night.
Is this a normal grief response, Acute Stress Disorder, the beginning of PTSD, or something else? What do you do next — and crucially, do you manage him here or refer him today?
WHY THIS MATTERS
Trauma exposure is ubiquitous in clinical practice. India sees over 450,000 road traffic accidents annually; domestic violence affects an estimated 30% of married women; healthcare workers, police personnel, and NDRF first responders face occupational trauma. The Indian Army and paramilitary services regularly present returning personnel with stress-related disorders to government hospitals. Under NMC Competency PS8.1, you are expected to diagnose stress-related disorders and make appropriate referral — not to transfer all of them immediately. The primary care level skills of recognising ASD and adjustment disorder, delivering psychological first aid, and applying structured referral criteria are among the most practically important skills of your internship year. Getting the differential right determines whether a patient receives the right treatment in time — or waits months for a psychiatric appointment while their condition becomes entrenched.
RECALL
Two pieces of prior learning ground today's content.
First, from Physiology (PY): the stress response is mediated by the HPA axis. A perceived threat activates the hypothalamus → pituitary (ACTH release) → adrenal cortex (cortisol release), alongside acute sympathetic activation (adrenaline, noradrenaline). In the short term, this enhances alertness, memory consolidation, and physical performance. In pathological states, chronic or traumatic HPA activation disrupts hippocampal neurogenesis (impairing contextual memory and fear extinction) and produces amygdala hyperreactivity — the neurobiological core of PTSD.
Second, from Psychology (PS1 — principles of psychiatry): the distinction between a normal stress response and a disorder is fundamental. Not all distress after a traumatic event is a psychiatric disorder. The ICD-11 explicitly classifies 'Acute Stress Reaction' (6MB20) as a normal, time-limited response to an exceptional stressor — not a mental disorder. A psychiatric diagnosis is only appropriate when the response causes clinically significant impairment and meets the specific duration and symptom criteria of the chosen classification system.
Clinical Presentation of Stress-Related Disorders
Stress-related and trauma-related disorders form a spectrum defined by three axes: the type of precipitant (traumatic event vs any stressor), the timing of symptom onset relative to the precipitant, and the duration of symptoms. Understanding this three-axis framework converts an apparently confusing differential into a structured diagnostic exercise.
Acute Stress Disorder (ASD — DSM-5 diagnosis) presents in the immediate aftermath of a traumatic event — one involving actual or threatened death, serious injury, or sexual violence. The patient develops ≥9 symptoms from five clusters: intrusion (flashbacks, nightmares, distressing memories), negative mood (persistent inability to experience positive emotions), dissociation (altered sense of reality, depersonalisation, dissociative amnesia), avoidance (efforts to avoid distressing reminders of the trauma — places, people, thoughts), and arousal (hypervigilance, exaggerated startle, sleep disturbance, irritability, concentration problems). The critical timing feature is that ASD symptoms occur from 3 days to 1 month after the traumatic event. ASD is a DSM-5 diagnosis; ICD-11 uses the term 'Acute Stress Reaction' but classifies it as a normal response category (6MB20), not a formal disorder — this distinction must be stated when documenting or discussing with supervisors.
Post-Traumatic Stress Disorder (PTSD) shares the same four symptom clusters as ASD (intrusion, avoidance, negative cognitions and mood, hyperarousal — DSM-5 Criterion B, C, D, E) but is defined by duration >1 month after the traumatic event. PTSD may develop directly after the traumatic event, or transition from untreated ASD as the one-month mark is crossed. ICD-11 also recognises Complex PTSD (Cptsd) — a distinct disorder seen after prolonged, repeated interpersonal trauma (childhood abuse, domestic violence, captivity) — characterised by PTSD features plus disturbances in self-organisation: emotion dysregulation, negative self-concept, and interpersonal difficulties.
Adjustment Disorder is clinically and conceptually distinct from ASD/PTSD in one crucial way: it does not require a traumatic event — any identifiable stressor suffices (job loss, marital conflict, academic failure, medical diagnosis, financial problems). The patient develops emotional or behavioural symptoms that are disproportionate to the severity of the stressor, with marked distress exceeding what would be culturally expected. Under ICD-11, onset is within 1 month of the stressor; under DSM-5, onset is within 3 months. Both systems require resolution within 6 months of the stressor ending (assuming the stressor does not persist). Subtypes include: with depressed mood, with anxiety, with mixed anxiety and depressed mood, with disturbance of conduct.
| Disorder | Precipitant type | Onset | Duration | Classification |
|---|---|---|---|---|
| Acute Stress Disorder | Traumatic event (death/injury/sexual violence) | ≥3 days post-trauma | 3 days–1 month | DSM-5 (ICD-11 = normal reaction) |
| PTSD | Traumatic event | Any time post-trauma | >1 month | DSM-5 + ICD-11 |
| Adjustment Disorder | Any identifiable stressor | ≤1 month (ICD-11) / ≤3 months (DSM-5) | Resolves ≤6 months post-stressor | DSM-5 + ICD-11 |
SELF-CHECK
A 25-year-old woman was in a house fire 2 weeks ago — she escaped unharmed but has since had daily flashbacks, nightmares, emotional numbness, and avoids driving past the street where her house stood. She reports significant difficulty at work. By DSM-5, what is the most accurate diagnosis at this time?
A. PTSD — the core symptom clusters are present
B. Adjustment Disorder — the stressor is identifiable and she's reacting with distress
C. Acute Stress Disorder — symptoms started after a traumatic event and have lasted less than 1 month
D. Normal grief reaction — no diagnosis required
Reveal Answer
Answer: C. Acute Stress Disorder — symptoms started after a traumatic event and have lasted less than 1 month
At 2 weeks post-trauma, the duration places her within the 3 days–1 month window for Acute Stress Disorder (DSM-5). PTSD requires >1 month duration — cannot yet be diagnosed. Adjustment disorder does not require a traumatic event AND requires that symptoms are NOT better explained by another disorder (here ASD is the more specific fit). ICD-11 would classify her as having an Acute Stress Reaction (normal, non-disorder) — this is an important cross-system distinction to know.
Psychopathology and Aetiology: How Trauma Becomes a Disorder
Not everyone exposed to a traumatic event develops ASD or PTSD. Understanding why some individuals develop pathological responses and others do not is both scientifically important and clinically relevant — it guides which patients are at higher risk and most in need of early intervention.
The neurobiological model centres on a failure of the normal fear extinction process. After a traumatic event, the amygdala encodes an intense fear memory. Under normal circumstances, the prefrontal cortex (PFC) — particularly the ventromedial PFC — inhibits the amygdala and facilitates extinction: the gradual reduction of fear responses when the threatening cue is no longer followed by harm. In PTSD, neuroimaging consistently shows amygdala hyperreactivity (enhanced fear encoding) combined with reduced hippocampal volume (impairing contextual memory and safety learning) and blunted PFC activity (impaired extinction and emotional regulation). The result is a frozen fear memory — the trauma remains neurologically 'present' and is continually re-experienced through flashbacks and nightmares rather than being integrated as a past event.
The HPA axis dysregulation in PTSD is distinctive: unlike depression (which shows elevated basal cortisol), PTSD is characterised by low basal cortisol with an exaggerated cortisol response to trauma cues. This is thought to reflect a sensitised negative feedback loop. Chronic cortisol dysregulation itself causes hippocampal neuronal atrophy — creating a vicious cycle where early trauma impairs the very system (hippocampus) needed for contextual processing of fear memories.
The Ehlers-Clark cognitive model (the primary evidence base for CBT in PTSD) proposes that PTSD is maintained by two types of maladaptive cognitive processing: (1) excessively negative appraisals of the trauma and its sequelae ('I am permanently damaged,' 'Nowhere is safe,' 'What happened was my fault') and (2) a trauma memory that is poorly elaborated and contextualised — stored as sensory fragments and situationally triggered rather than as a coherent autobiographical narrative. The treatment goal of trauma-focused CBT is to update these appraisals and transform the trauma memory into a processed, integrated narrative.
Risk factors for developing ASD/PTSD after trauma include: severity of trauma exposure (dose-response relationship); peri-traumatic dissociation (loss of continuous memory during the event); prior trauma history; pre-existing depression or anxiety disorder; female gender (approximately twice the prevalence); lack of social support; acute peritraumatic physiological reactivity; and early avoidant coping. Protective factors include: high resilience, strong social support, rapid psychological first aid, timely debriefing in some settings, and absence of re-traumatisation.
Diagnosis: Distinguishing ASD, PTSD, and Adjustment Disorder
The differential diagnosis of stress-related disorders is most reliably approached through a timeline-first framework — establish the stressor type and timing before applying symptom criteria. This prevents the common error of applying PTSD criteria to an adjustment disorder (which does not require a traumatic stressor) or labelling a patient with ASD when they are still within the normal acute stress reaction period.
Step 1 — Was the stressor traumatic (as defined)? DSM-5 Criterion A for ASD/PTSD requires a traumatic stressor: exposure to actual or threatened death, serious injury, or sexual violence — through direct experience, witnessing, learning of it happening to a close family member/friend, or repeated/extreme exposure (first responders). If the stressor is significant but does not meet this definition (job loss, divorce, medical diagnosis, financial crisis), the diagnosis is Adjustment Disorder, not ASD/PTSD.
Step 2 — What is the duration since stressor onset? This immediately separates ASD from PTSD from Adjustment Disorder. A patient presenting with intrusion, avoidance, hyperarousal, and negative mood:
- At days 3–30 post-trauma → consider ASD (DSM-5)
- At >1 month post-trauma → consider PTSD (DSM-5 and ICD-11)
- After a non-traumatic stressor, onset ≤1 month (ICD-11)/≤3 months (DSM-5), symptoms resolve ≤6 months post-stressor → Adjustment Disorder
Step 3 — Apply symptom criteria.
For ASD (DSM-5): ≥9 symptoms from the five clusters (intrusion, negative mood, dissociation, avoidance, arousal); marked distress or functional impairment; not attributable to substance or medical condition.
For PTSD (DSM-5): presence of all four criterion sets — intrusion (B), avoidance (C), negative alterations in cognitions and mood (D), hyperarousal (E); duration >1 month (F); clinically significant distress or impairment (G).
For Adjustment Disorder (DSM-5): emotional or behavioural symptoms within 3 months of a stressor that are disproportionate to the stressor's expected severity or cultural context; not meeting criteria for another mental disorder; resolves within 6 months of stressor cessation.
Mental Status Examination features: In ASD/PTSD, expect anxious or dysphoric affect, hypervigilance (scanning behaviour, sitting with back to the wall), exaggerated startle on routine noise, intrusive imagery (patient may become distressed when describing the trauma), and possible emotional numbing or blunted affect. Dissociative symptoms (derealisation, depersonalisation) are especially prominent in ASD. In adjustment disorder, the affect is typically reactive (emotional, tearful) but not numbed; intrusive trauma imagery is absent; and the patient retains insight into the link between their distress and the stressor.
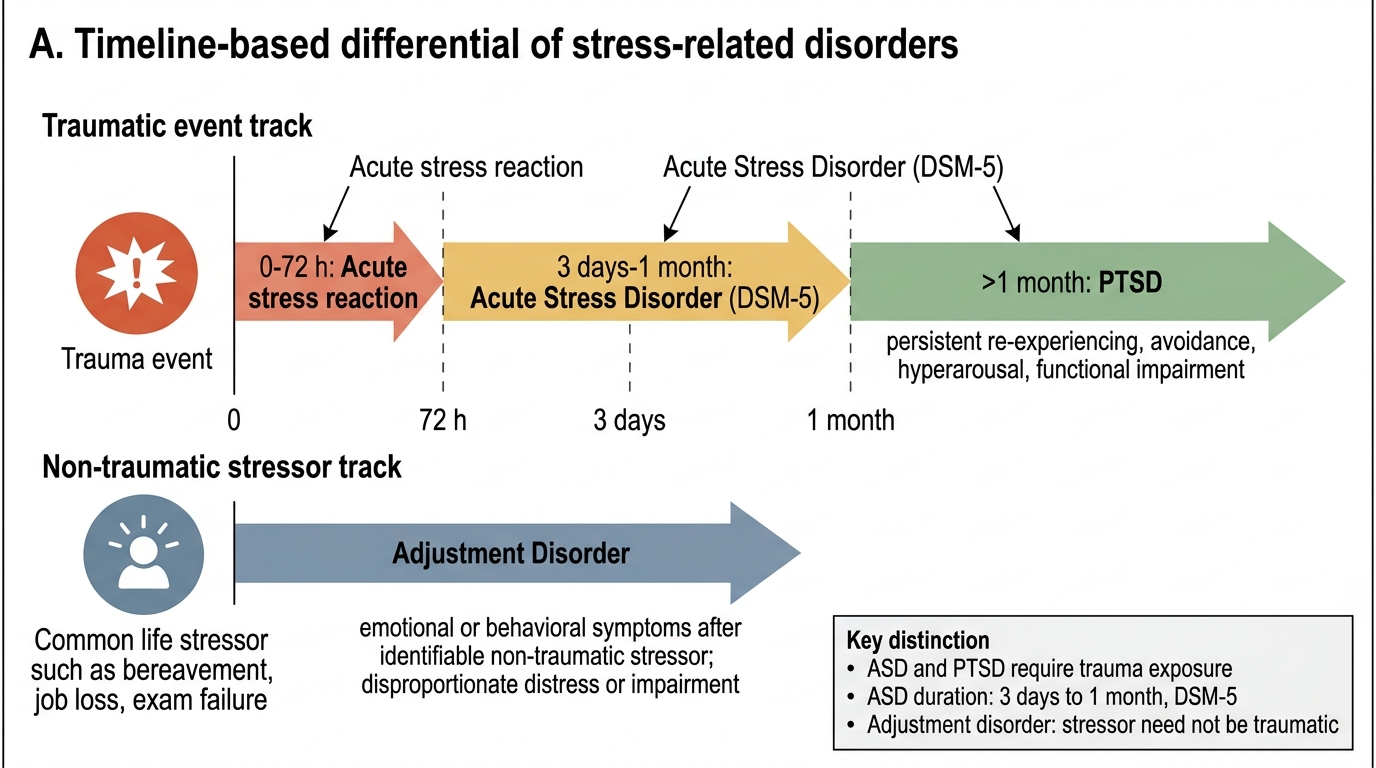
Timeline Differential of Stress-Related Disorders
SELF-CHECK
A government employee was passed over for promotion 5 months ago. Since then he has had persistent sadness, difficulty sleeping, and has started performing poorly at work. He has no traumatic stressor and has not improved despite reassurance. By ICD-11, adjustment disorder onset must be within how many months of the stressor?
A. Within 1 month of the stressor
B. Within 3 months of the stressor
C. Within 6 months of the stressor
D. Within 12 months of the stressor
Reveal Answer
Answer: A. Within 1 month of the stressor
ICD-11 requires adjustment disorder symptoms to begin within 1 MONTH of the identifiable stressor. DSM-5 uses a 3-month window. This distinction is clinically important — always state which system you are applying. In this case (5 months after the stressor, ICD-11 approach) the onset criterion is likely not met under ICD-11, but if symptoms started within 1 month of the promotion decision and are ongoing, it may still qualify. Both systems require that symptoms resolve within 6 months of the stressor ceasing.