Page 2 of 12
PS9.1 | Common Psychosexual Disorders — SDL Guide (Part 2)
Diagnosis and Mental Status Examination
The clinical assessment of psychosexual disorders requires a structured, sensitive, and non-judgemental approach. The psychiatric interview in this domain must balance thoroughness with rapport — patients who sense condemnation or hurry will disclose nothing. Beginning with open-ended, normalising questions ('Many of my patients find it difficult to talk about sexual concerns — it is completely confidential here, and I want to understand if there is anything in this area I can help with') sets the tone.
A full sexual history includes: onset and duration, pattern (global/situational, lifelong/acquired), impact on relationship and self-esteem, partner's perspective, previous treatment attempts, and relevant medical, surgical, and medication history. The PLISSIT model is not only a counselling framework but also a diagnostic scaffolding tool: at the 'Limited Information' stage you ask about specific symptoms; 'Specific Suggestions' begins after you have enough diagnostic data.
The mental status examination (MSE) in psychosexual disorders focuses on:
- Appearance and behaviour: note grooming, self-care, avoidance of eye contact when discussing sexuality — these may reflect shame or depression.
- Mood and affect: depression and anxiety are both common comorbidities and common causes of sexual dysfunction — assess for depressed mood, anhedonia, excessive worry.
- Thought content: beliefs about sexuality (guilt, religious prohibitions, misconceptions about normal function), performance expectations, partner blame or self-blame.
- Insight: does the patient recognise the problem as having both organic and psychological dimensions? Patients who externalise entirely ('it is a blood problem') or internalise entirely ('I am broken') are harder to engage in sex therapy.
- Cognitive function: concentration and memory deficits may reflect depression or organic brain disease.
Investigations to consider (targeted to clinical suspicion):
- Fasting blood glucose, HbA1c — to exclude diabetes
- Testosterone, prolactin, thyroid function tests — hormonal causes of desire and arousal disorders
- Lipid profile, blood pressure — cardiovascular risk for vascular ED
- Nocturnal penile tumescence (Rigiscan) — organic vs psychogenic ED
- Gynaecological examination (for dyspareunia/vaginismus) to exclude structural pathology
- Validated rating scales: IIEF (International Index of Erectile Function), FSFI (Female Sexual Function Index), PEDT (Premature Ejaculation Diagnostic Tool)
ICD-11 diagnostic requirements for all sexual dysfunctions: persistent or recurrent problem, clinically significant distress, minimum duration typically several months, exclusion of non-sexual mental disorders, relationship factors, and medical conditions as primary explanations. Always use ICD-11 (the current national and WHO standard) and note which system you are using when documenting.
Management — Pharmacological, Psychological, and Couple-based
Management of psychosexual disorders is inherently multimodal — and this multidimensionality is not a theoretical nuance but a practical clinical necessity. A purely biomedical approach without addressing relational and psychological dimensions fails most patients, because the organic and the psychological are bidirectionally entwined. A man who receives a PDE5 inhibitor for erectile dysfunction but whose performance anxiety is never addressed may find the medication works physically yet provides no restoration of confidence or spontaneity. Conversely, psychological therapy without attending to treatable organic causes — uncontrolled diabetes, hyperprolactinaemia, an offending antipsychotic — leaves the patient facing an avoidable biological obstacle to recovery. The clinician must therefore hold both dimensions simultaneously, formulate a working hypothesis about the relative contribution of each, and address them in a sequenced or parallel fashion depending on severity. This is what separates competent psychosexual medicine from symptomatic pharmacology.
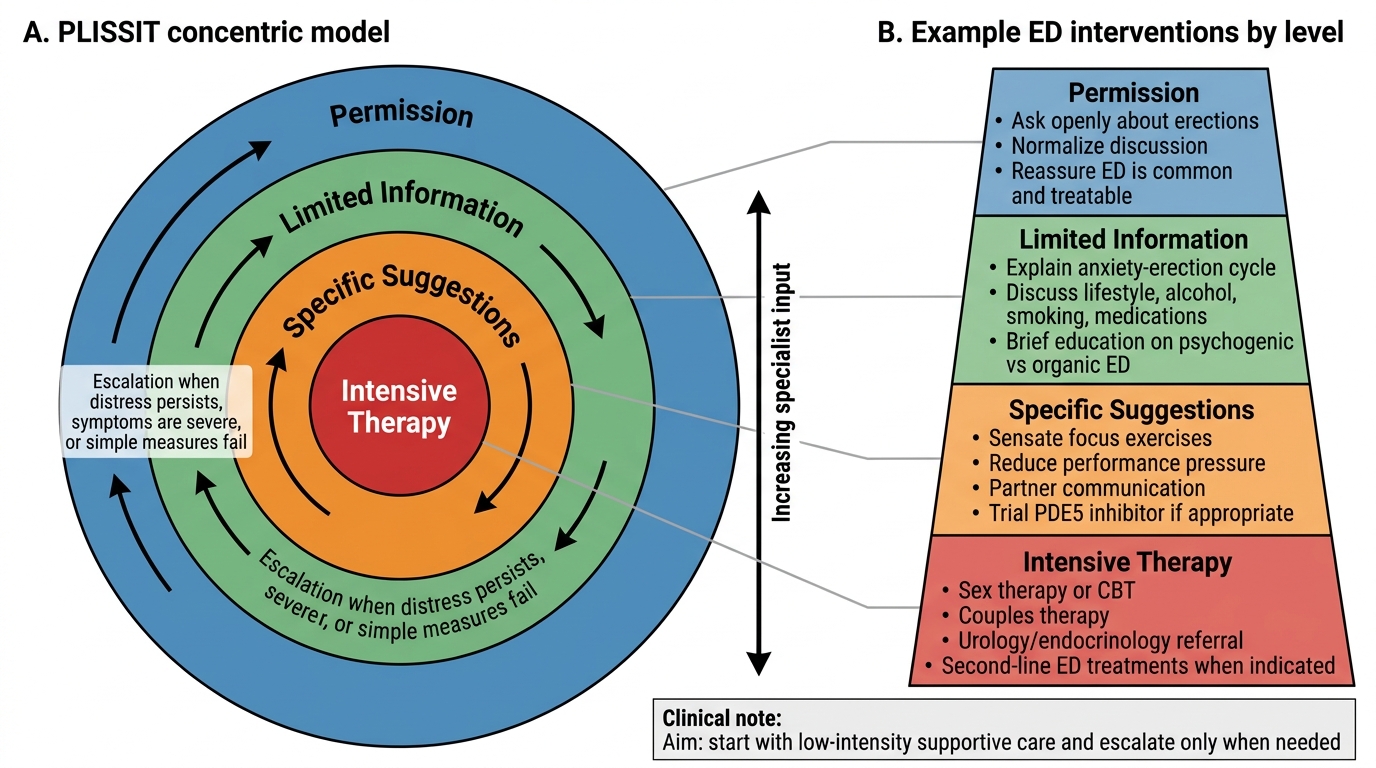
The PLISSIT model (developed by Annon, 1976) provides the canonical framework for graduated intervention by any clinician, regardless of their specialisation.
The PLISSIT model has four levels:
1. Permission (P): the clinician legitimises the patient's concerns by acknowledging that sexual problems are common, normal to discuss, and appropriate to treat. This alone — simple normalisation — has substantial therapeutic impact for many patients.
2. Limited Information (LI): provide brief, accurate psychoeducation about normal sexual function, common myths, and the mechanism of the specific disorder. Example: explaining the anxiety-erection failure cycle demystifies ED and often reduces performance anxiety immediately.
3. Specific Suggestions (SS): targeted behavioural strategies. For ED: sensate focus exercises, non-demand pleasuring; for PE: start-stop technique (Semans) and squeeze technique (Masters & Johnson); for vaginismus: graded vaginal dilation using dilators and relaxation training.
4. Intensive Therapy (IT): formal sex therapy (psychosexual therapy, cognitive-behavioural sex therapy) and/or pharmacotherapy for cases that do not respond to P/LI/SS.
Pharmacotherapy by disorder:
- Erectile dysfunction: Phosphodiesterase type 5 (PDE5) inhibitors are first-line — sildenafil, tadalafil, vardenafil. They potentiate NO-mediated smooth muscle relaxation in the corpus cavernosum. Contraindicated with nitrates (risk of severe hypotension). Tadalafil has a longer half-life (36 hours — 'the weekend pill'). Second-line options: intraurethral alprostadil, vacuum erection devices, intracavernosal injections; surgical implants for refractory cases.
- Premature ejaculation: Dapoxetine (30 mg or 60 mg on demand, 1–3 hours before intercourse) is the only approved on-demand SSRI for PE; it inhibits serotonin reuptake and delays ejaculation. Off-label: daily low-dose paroxetine, sertraline, or clomipramine (the latter is most effective but has greater side effects). Topical anaesthetics (lidocaine-prilocaine cream/spray) reduce penile sensitivity and are a useful adjunct.
- HSDD (male): address treatable causes — testosterone replacement for hypogonadism (under endocrinology guidance), replace offending medications where possible.
- Vaginismus: topical lidocaine for procedural examination; muscle relaxants (short-term) as adjunct to dilator therapy; management of comorbid anxiety (SSRIs if warranted).
- HSDD in women: oestrogen (local vaginal) for atrophic vaginitis; flibanserin (approved in some countries for premenopausal FSIAD — not widely used in India).
Psychotherapy options:
- Sex therapy (Masters and Johnson model): structured programme of sensate focus exercises, communication exercises, and gradual exposure; couple-based.
- Cognitive-Behavioural Therapy (CBT): target performance anxiety cognitions, self-monitoring beliefs, catastrophising.
- Mindfulness-based approaches: evidence base growing for FSIAD and PE.
- Couples therapy: when relationship conflict is a primary maintaining factor; often needed alongside individual treatment.
General principles: involve the partner wherever possible; address comorbid depression and anxiety; set realistic expectations; follow up to monitor progress and adjust treatment.
PLISSIT Model for Erectile Dysfunction Care
SELF-CHECK
A 32-year-old man with premature ejaculation (IELT < 1 minute, lifelong) asks about the first-line pharmacological option. Which of the following is correct?
A. Sildenafil 50 mg on demand — PDE5 inhibitor of choice for PE
B. Dapoxetine 30–60 mg taken 1–3 hours before intercourse — the only approved on-demand SSRI for PE
C. Daily fluoxetine 20 mg — first-line for premature ejaculation
D. Intracavernosal alprostadil — indicated when oral treatment fails
Reveal Answer
Answer: B. Dapoxetine 30–60 mg taken 1–3 hours before intercourse — the only approved on-demand SSRI for PE
Dapoxetine is a short-acting SSRI specifically approved for on-demand treatment of premature ejaculation. Its rapid absorption and short half-life make it suitable for as-needed dosing. PDE5 inhibitors treat erectile dysfunction, not PE. Daily SSRIs (paroxetine, sertraline, clomipramine) are used off-label; fluoxetine's long half-life makes it less preferred. Intracavernosal alprostadil is a second-line treatment for erectile dysfunction, not PE.
CLINICAL PEARL
The anxiety-erection failure cycle is self-sustaining — breaking it once may restore normal function. When a patient with psychogenic ED understands that performance anxiety causes sympathetic activation which physiologically prevents erection (adrenaline causes penile smooth muscle contraction, the opposite of what is needed), they are far less likely to catastrophise a failed erection. Psychoeducation at the 'Limited Information' level of PLISSIT can interrupt this cycle before any medication is prescribed. Always offer this before reaching for a prescription pad — and always check for concurrent depression, which is both a cause and consequence of sexual dysfunction.
Self-Assessment — Synthesising the Clinical Framework
Having completed this module, you should now be able to approach a patient presenting with a psychosexual concern with both clinical structure and human sensitivity. The foundational skill is not pharmacological — it is the ability to hold a non-judgemental space in which the patient feels safe enough to disclose a deeply private difficulty. Without that, no treatment reaches them.
The clinical framework rests on four pillars. First, phase-based classification: before you can treat, you must know which phase is disrupted. The ICD-11 framing (desire, arousal, orgasm, sexual pain) tells you where to look for organic causes, which validated rating scale to use, and which treatment options are phase-appropriate. A prescriber who reaches for sildenafil in a patient whose primary complaint is absent desire has mis-targeted the phase.
Second, organic-versus-psychogenic differentiation: the history (situational vs global, preserved nocturnal erections, sudden vs gradual onset), targeted investigations (testosterone, prolactin, blood glucose, NPT where indicated), and MSE together generate a working hypothesis about causation. Mixed aetiology is the rule, not the exception — document both dimensions and plan to address both.
Third, the PLISSIT framework positions every clinician — generalist and specialist alike — to intervene at the level their training permits. The psychiatrist should be competent through Specific Suggestions and prepared to refer for Intensive Therapy when needed. Knowing which behavioural technique maps to which disorder (start-stop for PE; graded dilators for vaginismus; sensate focus for performance-anxiety-driven ED) is clinical competency, not optional knowledge.
Fourth, partner inclusion and couple-centred care: sexual dysfunction almost always affects both partners. The man's ED is his wife's HSDD; her vaginismus is his anxiety. Treatment that ignores the relational system fails. Involve the partner wherever confidentiality permits and the patient consents.
The Mental Healthcare Act 2017 and the ethical obligations of the profession mandate that all patients — regardless of their sexual history, orientation, or relationship structure — receive dignified, non-discriminatory care. A clinician's personal discomfort is never a clinical reason to under-investigate or under-treat a sexual dysfunction.