Page 4 of 12
PS9.2 | LGBTQA+ Inclusive Psychiatric Practice — SDL Guide
Learning Objectives
- State the current legal position in India regarding same-sex relations and transgender rights, citing correct legislation and judgment years
- Identify the key changes in ICD-11 relevant to LGBTQA+ identities and the declassification of homosexuality
- Describe the governing ethical, humanitarian, and human-rights principles applicable to psychiatric care of LGBTQA+ patients
- Apply an affirmative, non-discriminatory clinical method when assessing and managing LGBTQA+ patients
- Recognise the health disparities affecting LGBTQA+ individuals and respond appropriately with inclusive clinical practice
- Explain why conversion therapy is condemned and constitutes professional misconduct
INSTRUCTIONS
Competency PS9.2 requires you to demonstrate knowledge of medico-legal, societal, ethical, and humanitarian principles in dealing with the LGBTQA+ community. This is a principles-and-skills SDL: the goal is not disease management but clinical conduct — the values, knowledge of law, and practical methods that enable you to provide dignified, non-discriminatory psychiatric care to every patient, regardless of their sexual orientation or gender identity. This module will give you the legal literacy, ethical framework, and clinical tools to fulfil this professional obligation.
References
- Ahuja N. A Short Textbook of Psychiatry, 8th ed. Jaypee Brothers; 2022. Chapter 1 (Ethics), Chapter 19 (Psychosexual). (textbook)
- NALSA v. Union of India, (2014) 5 SCC 438. Supreme Court of India. (legal)
- Navtej Singh Johar v. Union of India, (2018) 10 SCC 1. Supreme Court of India. (legal)
- Transgender Persons (Protection of Rights) Act 2019. Ministry of Social Justice and Empowerment, Government of India. (legislation)
- Mental Healthcare Act 2017. Ministry of Health and Family Welfare, Government of India. (legislation)
- ICD-11 for Mortality and Morbidity Statistics. World Health Organization; 2022. (guideline)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 24-year-old transgender woman is referred to the outpatient psychiatry clinic by a general practitioner with a note: 'Patient has gender confusion — please advise.' She enters the room nervously, having been misgendered in the waiting area. She tells you: 'I have come here for support with depression, not to be told something is wrong with me.' She is on hormonal therapy prescribed by an endocrinologist. She has stable employment, a supportive partner, and has never expressed psychosis or suicidal ideation. How you respond in the next five minutes will determine whether she ever seeks psychiatric help again — and whether you have fulfilled your professional obligation under Indian law and medical ethics. This module gives you the knowledge, the legal grounding, and the clinical method to get it right.
WHY THIS MATTERS
The LGBTQA+ community — persons who identify as lesbian, gay, bisexual, transgender, queer, asexual, or with another minority sexual orientation or gender identity — has historically been subjected to pathologisation, criminalisation, and institutional harm within healthcare settings. In India, two landmark Supreme Court judgments have fundamentally altered the legal landscape, and the ICD-11 has removed all diagnoses based on sexual orientation. As a future clinician, you will encounter LGBTQA+ patients across every specialty. Psychiatric consultations in this population are shaped by minority stress, stigma-related mental health disparities, and the fear of discrimination. Competency PS9.2 exists because the profession has a specific obligation: to know the law, uphold ethics, and provide affirmative care — not to be neutral, and certainly not to cause harm through ignorance or bias.
RECALL
Before we begin, activate what you already know:
- IPC Section 377: the colonial-era provision that criminalised 'carnal intercourse against the order of nature'; this section's consensual adult application was challenged and addressed in 2018.
- Mental Healthcare Act 2017: replaced the Mental Health Act 1987; decriminalised suicide attempt; established advance directives and nominated representatives; explicitly prohibits discrimination.
- ICD-10 vs ICD-11: ICD-10 contained diagnostic categories related to sexual orientation (e.g., 'Ego-dystonic sexual orientation'); ICD-11 removed all diagnoses based on sexual orientation and reclassified gender incongruence.
- Principles of medical ethics: autonomy, beneficence, non-maleficence, justice — and the specific NMC obligation of non-discrimination.
- Social determinants of mental health: stigma, discrimination, family rejection, and social exclusion are independent risk factors for depression, anxiety, and suicidality.
Clinical Indication and Relevance — Why This Competency Matters
LGBTQA+ individuals present to psychiatric care for the full spectrum of mental health conditions — depression, anxiety, PTSD, substance use disorders, self-harm, and suicidality. What distinguishes their clinical context is not a unique set of mental disorders, but a higher burden of these common disorders driven primarily by minority stress: the chronic, identity-specific stress arising from stigma, discrimination, internalised shame, identity concealment, and structural exclusion. Understanding this aetiological context is the first step in competent care.
Research consistently demonstrates that LGBTQA+ individuals have significantly elevated rates of depression (2–3× the general population), anxiety, post-traumatic stress (particularly from family rejection and violence), substance use, and suicidal ideation and attempts. These disparities are not inherent to LGBTQA+ identity — they are caused by hostile social environments. The minority stress model (Meyer, 2003) identifies three proximal stressors: concealment of identity, internalised homophobia/transphobia (shame arising from internalising societal prejudice), and the expectation of rejection (a hypervigilant anticipatory state that causes chronic psychological arousal).
In the Indian context, these stressors are particularly acute. Despite legal reform, family rejection after disclosure, housing and employment discrimination, and social ostracism remain common. Transgender women face intersectional discrimination — based on both gender identity and, frequently, caste and class. The clinician who is unaware of this context will attribute the patient's distress to the 'wrong' cause and prescribe the 'wrong' solution (medicating minority stress without addressing its social source).
This SDL exists because neutrality is not a professional option in the face of documented harm. An inclusive psychiatrist does not merely avoid being overtly discriminatory — they actively create a safe clinical environment, use affirming language, and are capable of explaining to a patient and their family the current medical, ethical, and legal position clearly and correctly.
Governing Principles — Legal Framework in India
The legal foundation of LGBTQA+ rights in India rests on three landmark decisions and two key statutes, all of which have direct clinical relevance.
NALSA v. Union of India (2014) — Transgender Rights Recognition
In April 2014, the Supreme Court of India, in National Legal Services Authority v. Union of India, delivered a unanimous judgment recognising the right of transgender persons to self-identify their gender. The Court held that: (1) transgender persons are entitled to recognition as a 'third gender'; (2) non-recognition of gender identity violates the fundamental rights to dignity and autonomy under Article 21 of the Constitution; and (3) the state has an obligation to provide welfare measures including healthcare, education, and social security for transgender persons. This judgment was the constitutional foundation for the right to self-identification — prior to this, there was no legal mechanism for a transgender person to change their legal gender.
The Transgender Persons (Protection of Rights) Act, 2019 subsequently operationalised some of these rights in legislation, providing for self-declaration of gender identity, anti-discrimination protection, and rights to healthcare, education, and employment. Importantly, this Act has been critiqued by activists for requiring a district-level certification process that may be intrusive, but it is the current operative legal framework.
Navtej Singh Johar v. Union of India (2018) — Decriminalisation of Consensual Same-Sex Relations
In September 2018, a five-judge Constitutional Bench of the Supreme Court of India, in Navtej Singh Johar & Others v. Union of India, read down Section 377 of the IPC to the extent it applied to consensual sexual acts between adults in private. The Court held, unanimously, that: (1) Section 377 violated Articles 14, 15, 19, and 21 of the Constitution; (2) homosexuality is not a mental disorder; (3) LGBTQA+ persons are entitled to equal citizenship. Critically, the Court read down (narrowed the application of) Section 377 — it did not repeal the entire section. Section 377 continues to apply to non-consensual acts, acts with minors, and acts with animals. The clinical significance is absolute clarity: consensual same-sex relations between adults in India are NOT criminal. Clinicians who conflate 'legal status' with 'morality' or who counsel patients based on incorrect legal information are causing clinical harm.
It is equally important to note that the Supreme Court, in Supriyo v. Union of India (2023), declined to recognise same-sex marriage as a fundamental right, holding that this is a matter for Parliament to legislate. This means decriminalisation does not imply marriage equality — these are legally separate questions. A clinician who conflates them provides incorrect information and may harm advocacy by overstating the law.
Mental Healthcare Act 2017
The Mental Healthcare Act 2017 (MHCA 2017) replaced the Mental Health Act 1987. Its key provisions directly relevant to LGBTQA+ care include: (1) recognition of the right to live in a community, without discrimination; (2) prohibition of denial of care on the basis of gender, sexual orientation, or any other protected characteristic; (3) the right to dignity, privacy, and confidentiality; (4) the right to make advance directives about treatment; (5) decriminalisation of suicide attempt (removes the criminal liability under Section 309 IPC). A clinician who refuses to treat or substandard-treats an LGBTQA+ patient on the basis of their identity is in violation of the MHCA 2017.
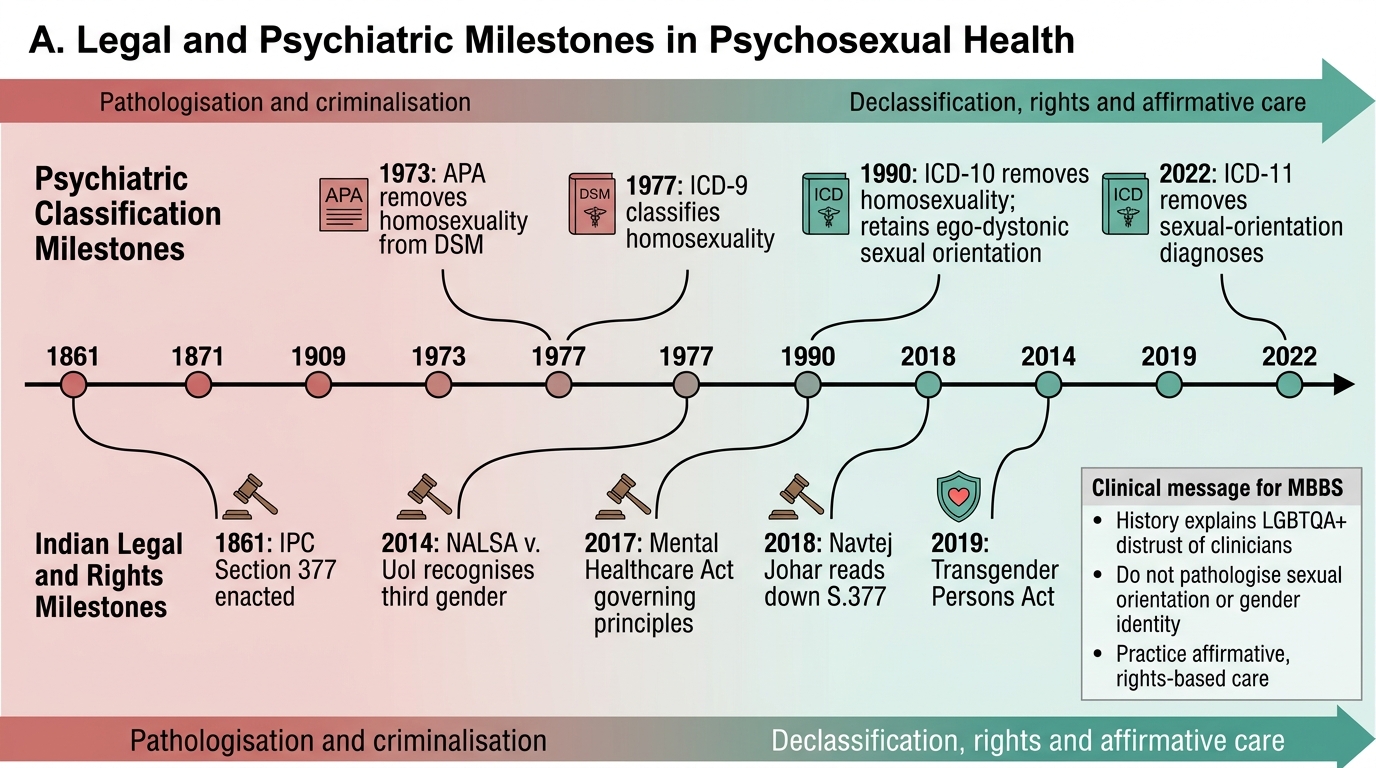
Milestones in Psychosexual Health: Law, Psychiatry and Rights
Governing Principles — ICD-11 Declassification and Medical Science
The history of psychiatry's relationship with sexual and gender diversity is a cautionary tale about how the profession can codify prejudice as pathology — and then must correct it. Understanding this history is not merely academic: it explains why LGBTQA+ patients distrust clinicians and why affirmative practice requires active positioning.
Homosexuality and psychiatry: the American Psychiatric Association removed homosexuality from the DSM in 1973, following decades of activism and the recognition that its inclusion was not based on empirical evidence of harm or disorder, but on societal norms. The ICD-9 continued to list it until 1990 when ICD-10 removed homosexuality as a diagnostic category. However, ICD-10 retained 'Ego-dystonic sexual orientation' (F66.1) — a diagnosis for distress arising from unwanted homosexual urges — which continued to be misused as a justification for conversion practices.
ICD-11 (2022): the current revision has removed all diagnoses based on sexual orientation, including ego-dystonic sexual orientation. There is no ICD-11 diagnosis whose criterion is homosexuality, bisexuality, or any sexual orientation. Sexual orientation is not a clinical variable for diagnosing mental disorders. A clinician who records 'homosexuality' as a diagnosis is using an obsolete and ethically condemned classification.
Gender incongruence in ICD-11: this is a critical and often misunderstood distinction. ICD-11 did NOT delete the concept of gender incongruence. Rather, it moved gender incongruence from the mental disorders chapter to Chapter 17 — Conditions Related to Sexual Health. The rationale was pragmatic: retaining the category enables access to gender-affirming care (hormonal therapy, surgical referral) through health systems, while removing the stigma of a 'mental disorder' classification. Being transgender is therefore not classified as a mental disorder in ICD-11, but the ICD-11 category 'gender incongruence of adolescence or adulthood' exists to enable clinical care access.
This distinction matters in practice: when a clinician tells a patient 'you have a mental disorder because you are transgender,' they are factually wrong under ICD-11. When they explain that a clinical code exists to enable access to appropriate care, and that this is a health condition classified in a chapter distinct from mental disorders, they are accurate and helpful.
Conversion therapy is any practice — whether psychotherapeutic, pharmacological, or spiritual — that aims to change a person's sexual orientation or gender identity. It is condemned by the World Psychiatric Association, the World Health Organization, the Psychological and Psychiatric professional bodies in India, and the National Medical Commission. It is not merely ineffective (evidence shows it does not change sexual orientation); it causes documented psychological harm including depression, anxiety, self-harm, and suicidality. A psychiatrist who engages in or refers for conversion therapy violates NMC ethics, the non-maleficence principle, and the patient's right to dignity under the Constitution and the MHCA 2017. This is professional misconduct.
SELF-CHECK
In Navtej Singh Johar v. Union of India (2018), the Supreme Court:
A. Struck down Section 377 IPC in its entirety, decriminalising all sexual acts
B. Read down Section 377 IPC to decriminalise consensual sexual acts between adults, while retaining the section's applicability to non-consensual acts, acts with minors, and acts with animals
C. Recognised same-sex marriage as a fundamental right under the Constitution
D. Only addressed the rights of transgender persons, not homosexual individuals
Reveal Answer
Answer: B. Read down Section 377 IPC to decriminalise consensual sexual acts between adults, while retaining the section's applicability to non-consensual acts, acts with minors, and acts with animals
The Navtej Johar judgment (2018) specifically read down (narrowed the application of) Section 377 IPC so that it no longer applies to consensual sexual acts between adults in private. The section itself was not repealed — it continues to cover non-consensual acts, acts with minors, and bestiality. Same-sex marriage was not addressed (that was the Supriyo v. UoI case in 2023, which declined to recognise it). NALSA (2014) addressed transgender rights; Navtej Johar addressed the decriminalisation of consensual same-sex relations.