Page 2 of 8
PS12.1 | Suicide Risk Assessment — SDL Guide (Part 2)
Risk Factor Framework and Interpretation
Once the six assessment domains have been explored, the clinician synthesises the findings into a risk stratification. This synthesis requires a structured conceptual framework for the factors that increase and decrease suicide risk. The most widely taught mnemonic in clinical psychiatric practice is SAD PERSONS, originally described by Patterson et al. (1983) and adapted for routine clinical use. While it has limitations as a standalone prediction tool — it was derived from a specific population and cannot reliably predict individual risk — it serves as a robust educational scaffold for organising the risk factor landscape and ensuring systematic coverage.
Provided image
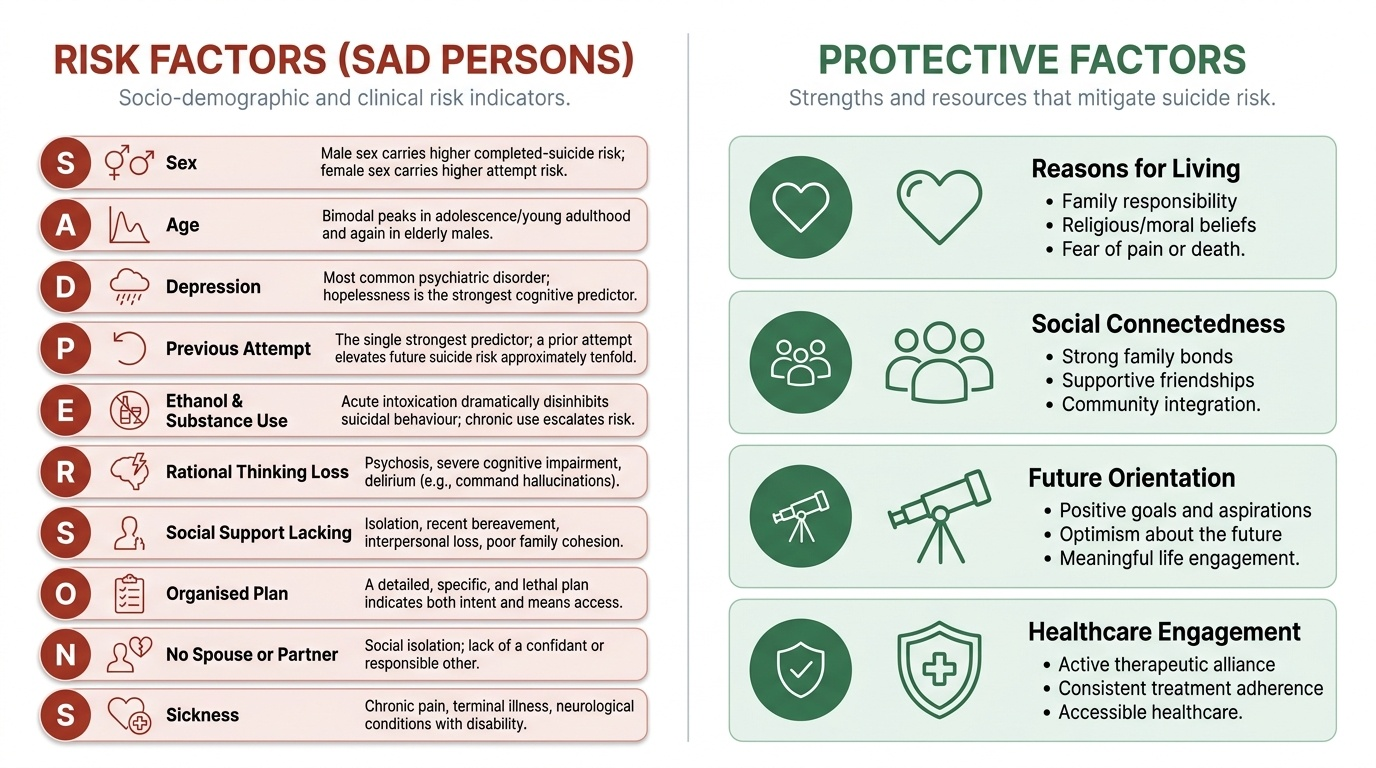
The SAD PERSONS mnemonic represents: Sex (male sex carries higher completed-suicide risk; female sex carries higher attempt risk), Age (bimodal peaks in adolescence/young adulthood and again in elderly males), Depression (the most common psychiatric disorder associated with suicide; within depression, hopelessness is the strongest cognitive predictor of suicidal behaviour), Previous attempt (the single strongest predictor — a prior attempt elevates future suicide risk approximately tenfold), Ethanol and substance use (acute intoxication dramatically disinhibits suicidal behaviour; chronic use escalates chronic risk), Rational thinking loss (psychosis, severe cognitive impairment, delirium — the patient may act on command hallucinations or delusional thinking), Social support lacking (isolation, recent bereavement, interpersonal loss, poor family cohesion), Organised plan (a detailed, specific, and lethal plan indicates both intent and means access), No spouse or partner (social isolation; lack of a confidant or responsible other), Sickness (chronic pain, terminal illness, neurological conditions — particularly those associated with disability and loss of function).
The corresponding protective factors are equally important to assess and document explicitly. These include: reasons for living (family responsibility, religious prohibitions against suicide, fear of pain or death), strong social supports, a sense of future orientation (concrete plans and goals), engagement with mental health treatment, problem-solving ability, and absence of access to lethal means. A patient with multiple risk factors but robust protective factors may be safely managed with intensive outpatient care; one with fewer risk factors but profound hopelessness and social isolation may warrant inpatient admission. The clinical decision requires weighing both sides of the ledger.
Risk stratification distils this integrated assessment into a clinical judgment of level of immediate risk:
| Risk Level | Clinical Profile | Immediate Action |
|---|---|---|
| Low | Passive ideation only, no plan, no intent, strong protective factors, no prior attempt or a distant low-lethality attempt | Safety planning, outpatient follow-up, family involvement, means restriction counselling |
| Moderate | Active ideation with some intent, vague or undetailed plan, limited protective factors, or one prior low-lethality attempt | Intensified outpatient monitoring, family safety-netting, crisis service referral; reassess within 24–48 h |
| High | Active ideation with clear intent, specific lethal plan, identified means access, prior high-lethality attempt, hopelessness, poor social support | Hospital admission; if voluntary admission refused and imminent risk is established, consider involuntary admission under MHCA 2017 |
A critical caveat applies to this table: risk stratification is a clinical guide, not a prediction. No validated instrument can reliably predict which individual patient will die by suicide. Stratification guides the intensity of intervention; it does not produce a certainty. The clinician must communicate this limitation honestly in documentation and in conversations with the patient and family.
Applied Practice — Safety Planning, Means Restriction, and Documentation
The structured assessment, however thorough, is only clinically complete when it is followed by action calibrated to the risk level. The three core applied responses to a suicide risk assessment are: safety planning, means restriction, and accurate documentation. Each represents a distinct but complementary layer of clinical intervention.
Safety planning is an evidence-based intervention in which the clinician and patient collaboratively construct a written, personalised crisis plan that the patient can use if suicidal urges intensify between clinical contacts. It is explicitly distinct from — and superior to — a simple 'no-suicide contract', which has no evidence base and may generate false reassurance by treating the patient's distress as a contractual matter rather than a clinical emergency. The Stanley-Brown Safety Planning Intervention (Stanley & Brown, 2012), which has strong evidence from randomised and quasi-experimental studies including an emergency department trial, involves six sequential steps that must be completed in order, with the easier steps placed first so the patient uses them before escalating to professional contact:
- Warning signs — the patient identifies personal signals that a suicidal crisis may be imminent: specific thoughts, feelings, behaviours, situations, or physiological states that precede escalating distress
- Internal coping strategies — activities the patient can perform alone to distract and self-soothe, without contacting another person (exercise, listening to music, practising deep breathing, mindfulness)
- Social contacts for distraction — specific people and social settings that provide distraction without requiring the patient to discuss her crisis; the purpose is engagement, not disclosure
- People to contact for support — specific trusted individuals the patient agrees to contact when distress is escalating; these are named people whose availability and willingness has ideally been confirmed
- Professionals and agencies to contact in a crisis — the treating psychiatrist or therapist, crisis helplines (iCall: 9152987821; Vandrevala Foundation: 1860-2662-345), and emergency services contact numbers
- Means restriction steps — concrete actions agreed between the patient and family to reduce access to the identified lethal means, documented in the plan itself
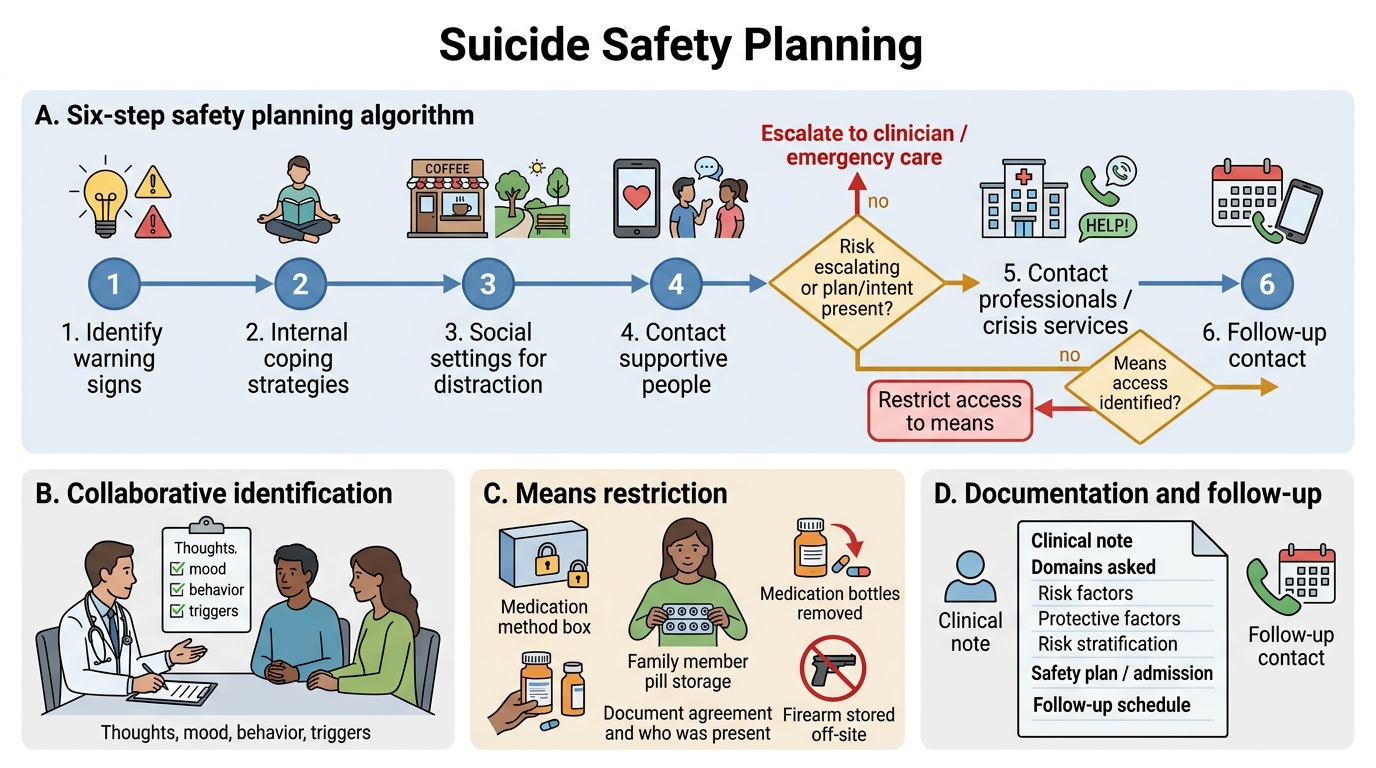
Six-Step Safety Planning Algorithm
Means restriction is among the most evidence-supported individual and population-level interventions in suicide prevention. At the individual level, this involves a frank and direct conversation — ideally conducted with a trusted family member present — about limiting access to the identified means: removing excess medication bottles from the home, transferring custody of pill storage to a family member, ensuring firearms are stored at a separate location, and discussing any other method-specific access. This conversation must be documented explicitly in the clinical record, including who was present and what was agreed.
Documentation is the third pillar of applied practice. A medico-legally defensible and clinically useful record of a suicide risk assessment must include: the specific domains explored and the patient's responses to each; the risk and protective factors identified; the clinical risk stratification and the reasoning behind it; the management decisions made (safety plan, admission, follow-up schedule); and the patient's and family's responses to the plan. The note must be specific — documenting that the clinician asked about past attempts, about plan, and about means access — not merely recording 'patient denies suicidal ideation.' A vague note is clinically inadequate and medico-legally indefensible.
Clinicians working in India must also be explicit with patients and families about the legal position under the Mental Healthcare Act 2017: persons who have attempted suicide are to be provided care, treatment, and rehabilitation — not criminal prosecution. This framing reorients the clinical encounter toward support rather than judgment, and is part of the clinician's duty under the Act.
CLINICAL PEARL
The single most dangerous error in suicide risk assessment is equating the absence of a stated plan with the absence of risk. Many patients who go on to die by suicide did not disclose a specific plan during a prior clinical encounter — either because they withheld it deliberately, because they had not fully formulated it at that point, or because the clinician did not ask directly enough. The structured six-domain approach described in this module is designed precisely to elicit the information that passive or euphemistic questioning misses. Never conclude an assessment early because the patient appears calm, cooperative, or because the immediate precipitant seems to have resolved. Suicidal calm following a period of agitation can indicate that a decision has been made and the ambivalence resolved — not that the crisis has passed.
Self-Assessment — Consolidating the Skill
Before you certify yourself ready for supervised clinical practice of this skill, work through the following structured self-assessment. This is not a passive recall exercise — it is a simulation of the clinical reasoning process you will need to execute at the bedside. Read the vignette, then answer each of the structured prompts in sequence, as if you were the treating clinician. Approach this seriously: the ability to reason through each domain systematically, and to identify where you are uncertain, is the competence this SDL is designed to build. If you find yourself uncertain at any step, return to the relevant section before proceeding — that is precisely what self-directed learning is designed to support.
Provided image
Vignette: Meera, a 24-year-old unmarried woman, is brought to the psychiatry OPD by her mother. She has been treated for major depressive disorder for three months and was recently passed over for a promotion at work. Her mother reports that Meera has been increasingly withdrawn and was found yesterday with a blister pack of her antidepressants, tearing out the tablets and placing them in a small envelope. When you ask Meera directly whether she has been thinking about ending her life, she says, 'Every day. I don't see the point anymore. I've thought about taking all these tablets at once.' She denies having done anything yet. She lives with her mother. She states she finds it difficult to imagine a reason not to do it.
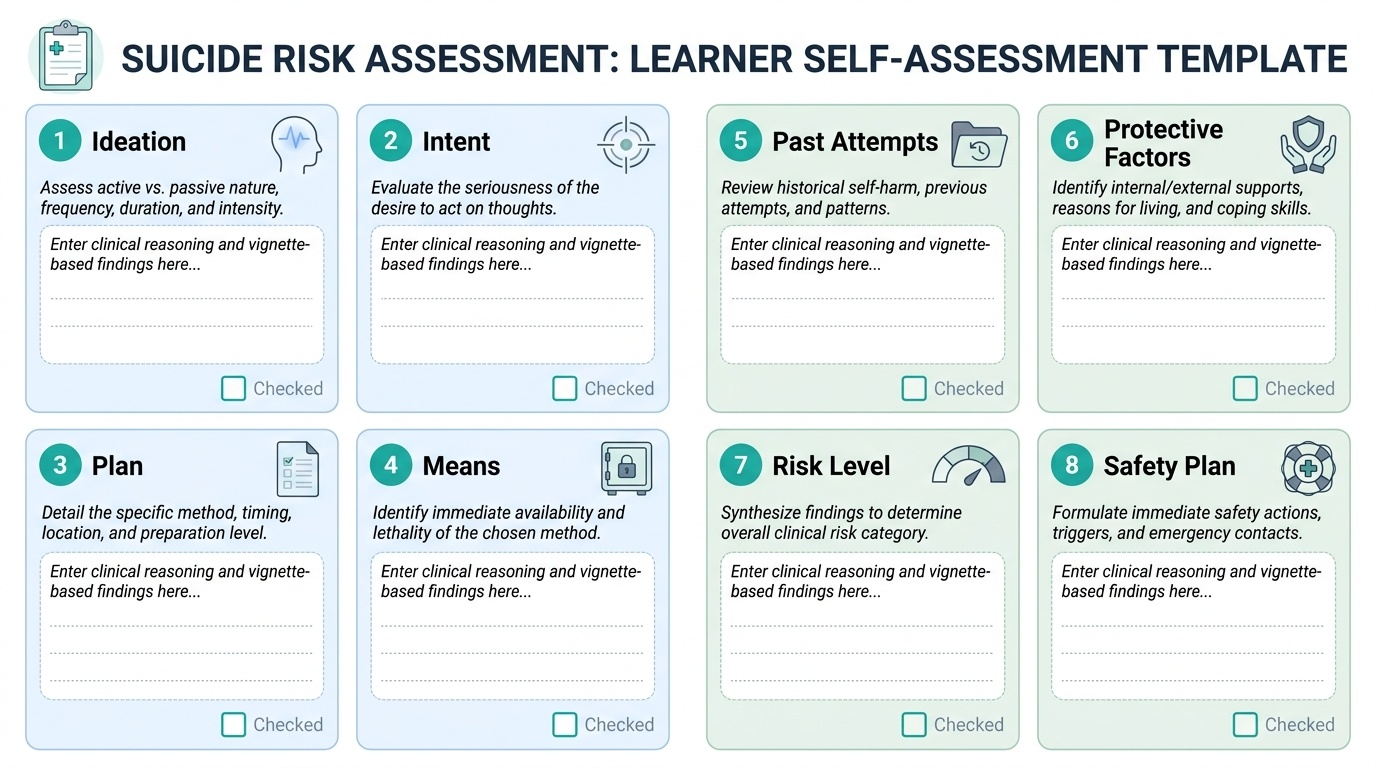
Structured self-check prompts:
- Ideation domain: Is Meera's suicidal ideation passive or active? How would you characterise its frequency and intensity based on the vignette? What three follow-up questions would you ask to characterise it further on the C-SSRS spectrum?
- Intent domain: What does Meera's statement 'I don't see the point anymore' and her difficulty imagining reasons not to act tell you about the degree of intent? What single direct question would most precisely clarify her intent at this moment?
- Plan and means access: What evidence of a plan is present? What is the identified method? What is the clinical significance of the tablets having been pre-sorted into an envelope? What immediate means restriction action would you take in this consultation?
- Past attempts: The vignette does not provide this information. Explain why the history of prior attempts is the single most important question you must ask before stratifying risk. What specific details about a prior attempt — if disclosed — would shift your stratification from moderate to high?
- Protective factors: Identify the one protective factor explicitly present in this vignette. What three additional protective factor questions would you direct to Meera and her mother?
- Risk stratification: Using the low/moderate/high framework from this SDL, stratify Meera's risk and provide a written justification that cites at least four features of the vignette.
- Mental Healthcare Act 2017: If Meera had taken an impulsive overdose two weeks ago but had been managed medically at a private clinic without psychiatric referral, which Act governs how that episode should be managed? What does Section 115 of the Mental Healthcare Act 2017 specifically state? Which Act does it replace, and what was the prior legal status of suicide attempt under the replaced legislation?
- Safety planning: Write out the six steps of the Stanley-Brown Safety Planning Intervention as they would apply specifically to Meera's situation. Include concrete means restriction recommendations and at least two crisis contact details.
This structured exercise covers every domain in this SDL. If you answered all eight prompts confidently and accurately, you are prepared for supervised clinical application of this skill. If you found yourself uncertain — particularly at prompts 4, 6, or 7 — return to those sections before your next clinical encounter. Confident, systematic, compassionate risk assessment is not just an examination skill: it is a life-saving clinical act.