Page 1 of 14
RD4.1 | Imaging Requisitions, Urgency Communication and Specialist Clarification — SDL Guide
Learning Objectives
- Explain why an imaging requisition is a clinical communication act that determines protocol, urgency and patient safety, not a clerical form.
- Construct a high-quality imaging requisition containing a focused clinical history, a specific clinical question, a provisional diagnosis, and the mandatory safety flags.
- Convey clinical urgency in a way that drives correct scheduling, distinguishing routine, urgent and emergent requests.
- Clarify the appropriateness of an imaging procedure with the radiologist when in doubt, using referral guidance (ACR Appropriateness Criteria / AERB) and the justification principle.
- Close the imaging loop by acting on the report, communicating critical results, and avoiding duplicate examinations.
INSTRUCTIONS
Every imaging study a primary-care physician orders begins with a requisition, and the quality of that requisition determines whether the radiologist can protocol the correct study, prioritise the patient appropriately, and answer the actual clinical question safely. A vague or unsafe request wastes radiation, delays diagnosis, and occasionally harms patients. This module treats the requisition as a structured clinical skill — what to write, how to convey urgency, and when to pick up the phone and ask the radiologist — so that your collaboration with imaging specialists is grounded in clear, safe, purposeful communication.
References
- Sutton's Textbook of Radiology, 6th edition, Chapter 1 (Principles and the Imaging Request) (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter 1 (Principles of Medical Imaging and Referral) (textbook)
- Atomic Energy Regulatory Board (AERB) Safety Manual for Diagnostic Radiology, India — referral and justification (guideline)
- ACR Appropriateness Criteria (American College of Radiology) — evidence-based imaging referral (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
At 2 a.m. a house officer types into the radiology request system: 'CT abdomen. Pain.' Nothing else — no history, no specific question, no renal function, no mention that the patient is 32 weeks pregnant. The on-call radiologist, who has never seen this patient, must now telephone the ward to find out what is actually being asked, discovers the pregnancy, and the whole study is reconsidered at 2 a.m. when an ultrasound should have been the first step. The scan is delayed by hours, the patient is anxious, and a near-miss radiation exposure to a fetus was avoided only by luck. Contrast this with a one-line requisition that reads: '32-week pregnant woman, RIF pain and fever 12 h, ?appendicitis vs ?ovarian pathology; please advise modality — would prefer USG given pregnancy.' The same clinician, the same patient — but one of these requisitions is a clinical act and the other is a hazard.
WHY THIS MATTERS
The imaging requisition is the single most frequent point of contact between a primary-care physician and the imaging service, and it is where most avoidable imaging errors originate. NMC competency RD4.1 specifically requires you to collaborate with imaging specialists — to provide relevant clinical information, to convey clinical urgency so the patient is scheduled correctly, and to clarify appropriateness when you are in doubt. These are not radiology-department problems: a missing eGFR on a contrast request, an unflagged pacemaker on an MRI request, or an absent clinical question are failures of the requesting clinician. A poor requisition produces the wrong protocol, the wrong priority, an uninterpretable report ('clinical correlation advised'), repeat imaging, and sometimes patient harm. A good requisition lets the radiologist tailor the protocol, prioritise correctly, answer your question, and keep the patient safe. This skill is examined in clinical postings, in the OSCE, and — most importantly — exercised every working day of your career.
RECALL
Before reading further, bring forward what you already know from the radiology foundation module and from earlier clinical learning:
- Modality dose hierarchy: a chest X-ray delivers ~0.02 mSv whereas a CT abdomen-pelvis delivers ~8-10 mSv — several hundred times more. Dose is therefore a reason to state your question precisely so the lowest-dose adequate study is chosen.
- Ultrasound and MRI are non-ionising; ultrasound is first-line for biliary, renal, obstetric and vascular questions and is preferred in pregnancy and children.
- Iodinated contrast carries a risk of contrast-associated kidney injury, so renal function (eGFR) is needed before contrast CT; gadolinium carries a risk of nephrogenic systemic fibrosis in severe renal failure.
- MRI has real contraindications — pacemakers/ICDs, cochlear implants, ferromagnetic intra-ocular foreign bodies, certain aneurysm clips — so implant/device status must be declared.
- AERB is India's statutory radiation regulator and mandates that every ionising study be clinically justified — a responsibility shared by the requesting clinician.
If any of these feel hazy, a quick review of the foundation module before continuing will make the requisition principles below click into place.
Why the Requisition Is a Clinical Act, Not a Form
An imaging requisition is best understood not as an administrative form that releases a slot on a scanner, but as a written clinical consultation between you and the radiologist. When you request an investigation you are asking a specialist colleague — who will never have examined your patient — to design, supervise and interpret a study on your behalf. Everything the radiologist decides flows from what you write: which modality is appropriate, which protocol to run, whether to give contrast, how urgently to fit the patient in, and how to read the resulting images. The radiologist's report is only as good as the clinical question it was asked to answer. This is precisely why the indication and the specific clinical question matter so much: an image is not self-interpreting, and the same set of pixels can mean different things depending on the question being asked of them.
Framing the requisition as a clinical act has three immediate consequences for how you write it:
- It must carry the reasoning, not just the order. The radiologist needs to know what you are worried about and why, so the study can be tailored to confirm or refute it.
- It must enable a safe study. The safety flags you provide (renal function, contrast allergy, pregnancy, implants) are the only way the radiologist can avoid harming a patient they cannot examine.
- It must communicate priority. The radiologist schedules dozens of patients; only your requisition tells them whether this one can wait two weeks or needs to be in the scanner within the hour.
The rest of this module unpacks each of these — content, safety, urgency and clarification — as a learnable, repeatable skill.
Principles of a High-Quality Imaging Requisition
A high-quality requisition is governed by a simple principle: give the radiologist everything they need to choose the right study, run it safely, and answer your question — and nothing that merely clutters. In practice this resolves into a small set of mandatory components, each of which serves a distinct purpose in the radiologist's decision-making. The single most common defect is omitting the specific clinical question: a request that says 'abdominal pain, please scan' forces the radiologist to guess, whereas '?acute appendicitis' or '?renal calculus' directs the protocol and the search pattern. The second most common defect is omitting safety information, which is the only mechanism by which a clinician who is not present can prevent contrast injury or an MRI accident.
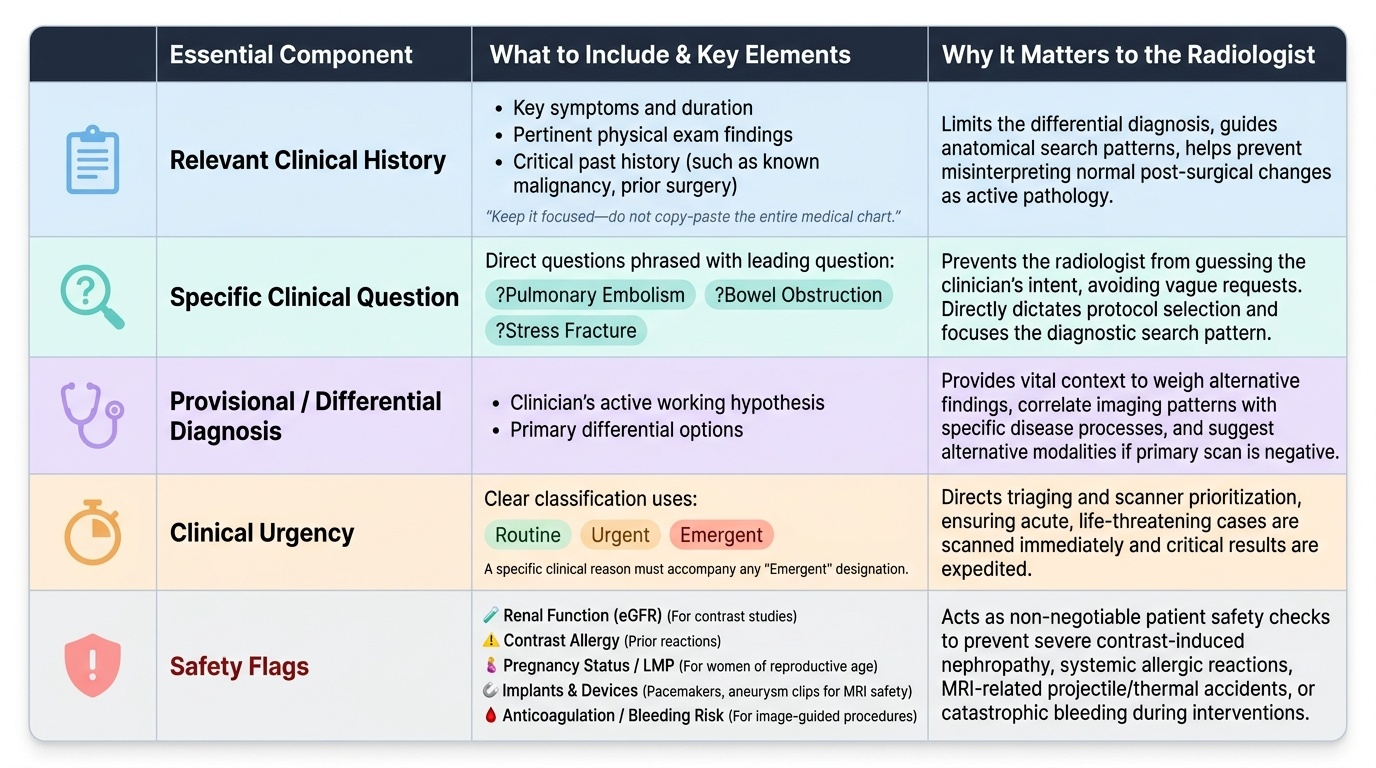
The essential components of a high-quality requisition are:
- Relevant, focused clinical history: the key symptoms, duration, relevant examination findings and pertinent past history (e.g. known malignancy, prior surgery, immunosuppression). Focused — not the entire chart.
- A specific clinical question: what you want the study to answer, phrased as a question (?pulmonary embolism, ?bowel obstruction, ?stress fracture).
- A provisional or differential diagnosis: your working hypothesis, which lets the radiologist weigh alternatives.
- Clinical urgency: routine, urgent or emergent, with a reason if emergent.
- Safety flags (the non-negotiable patient-safety set): renal function (eGFR) for any contrast study; known contrast allergy or prior reaction; pregnancy status / last menstrual period in reproductive-age women; implants and devices (pacemaker, ICD, cochlear implant, aneurysm clip, ferromagnetic foreign body) for any MRI request; and anticoagulation/bleeding risk for image-guided procedures.
- Patient identifiers and the requesting clinician's contact details, so the radiologist can reach you to clarify or to convey a critical result.
Provided image
Constructing the Requisition — A Step-by-Step Method
Knowing the components is not the same as reliably producing them under time pressure at 3 a.m., so it helps to have a repeatable method. A useful structure borrows from the SBAR communication framework already familiar from clinical handover — Situation, Background, Assessment, Recommendation/Request — adapted to the imaging request. Working through a fixed sequence ensures the specific question and the safety flags are never the parts that get dropped when you are busy, because they have a dedicated slot in your mental template. The goal is a requisition that a radiologist who has never met the patient can read once and immediately understand what to do, how urgently, and how to keep the patient safe.
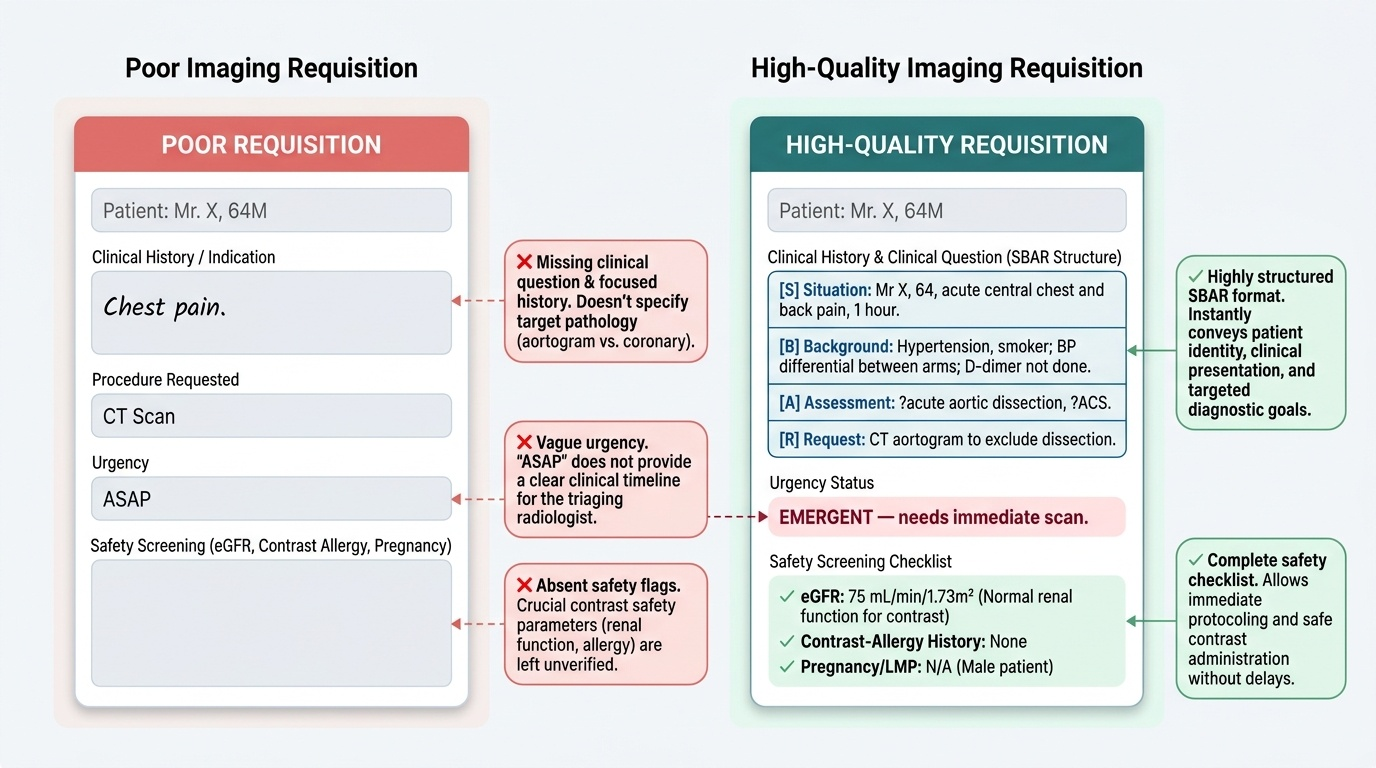
A step-by-step method for constructing the requisition:
- Situation — state who the patient is and the headline problem in one line: 'Mr X, 64, acute central chest and back pain, 1 hour.'
- Background — the focused relevant history: 'Hypertension, smoker; BP differential between arms; D-dimer not done.'
- Assessment — your provisional/differential diagnosis: '?acute aortic dissection, ?ACS.'
- Request — the specific clinical question and the study you propose: 'CT aortogram to exclude dissection.'
- Urgency — explicitly: 'EMERGENT — needs immediate scan.'
- Safety flags — run the checklist every time: eGFR (for contrast), contrast-allergy history, pregnancy/LMP (reproductive-age women), implants/devices (any MRI), anticoagulation (for procedures). Record each as present/absent rather than leaving it blank — a blank tells the radiologist nothing about whether you checked.
- Contact — your name and a number the radiologist can call.
A practical discipline: before you submit, re-read the requisition and ask, 'If I were the radiologist and had never seen this patient, could I choose the protocol and run it safely from this alone?' If not, add what is missing.
Provided image
SELF-CHECK
A primary-care physician requests a contrast-enhanced CT abdomen for a 70-year-old man with weight loss and a suspected pancreatic mass. Which single piece of information is MOST important to include on the requisition to allow the study to proceed safely?
A. The patient's occupation and social history
B. The renal function (eGFR), because iodinated contrast risks contrast-associated kidney injury
C. The exact time the patient last ate
D. The patient's height and weight only
Reveal Answer
Answer: B. The renal function (eGFR), because iodinated contrast risks contrast-associated kidney injury
For any iodinated-contrast CT, renal function (eGFR) is the critical safety flag: iodinated contrast can precipitate contrast-associated acute kidney injury, particularly at low eGFR, so the radiologist needs the eGFR to decide whether to proceed, modify, or seek an alternative. Occupation and last meal are not the primary safety determinants here, and height/weight alone does not address the contrast-safety question.