Page 2 of 11
RD7.2 | Imaging in ASOM and CSOM — SDL Guide (Part 2)
Impact on Diagnosis and Management — How the Report Changes the Operation
The reason RD7.2 sits at the knows-how level is that imaging in otitis media is never an end in itself — every finding must be integrated into a management decision, and the report literally changes what the surgeon does and how cautiously they do it. The clinician who can read the temporal-bone scan can anticipate the operation, warn the patient of specific risks, and recognise when an emergency has replaced an elective plan. Three management pathways flow directly from the imaging, and understanding this chain of finding-to-decision is the applied core of this competency.
Pathway 1 — Complicated ASOM (emergency drainage and brain protection):
When HRCT shows coalescent mastoiditis or a subperiosteal abscess, the management escalates from intravenous antibiotics alone to cortical mastoidectomy and abscess drainage. When contrast MRI shows an intracranial complication — meningitis, intracranial abscess or sigmoid sinus thrombosis — management becomes a neurosurgical/ENT emergency with intravenous antibiotics, surgical drainage of the source and the abscess, and anticoagulation considered for sinus thrombosis. Here imaging does not merely confirm the diagnosis; it dictates the urgency and the theatre.
Pathway 2 — Unsafe CSOM with cholesteatoma (choosing and planning the mastoidectomy):
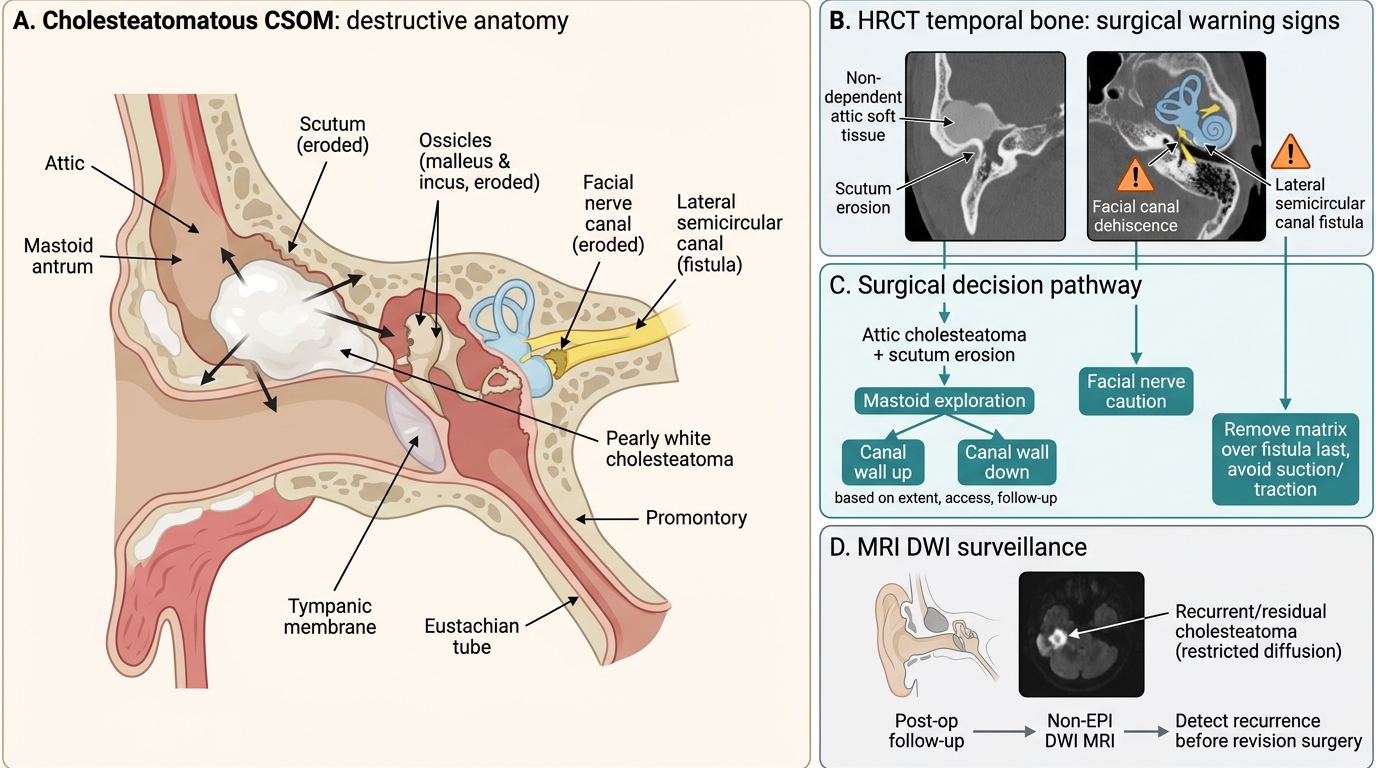
The HRCT map decides the type of surgery and the cautions during it. The presence and extent of cholesteatoma, the degree of mastoid pneumatisation and the integrity of the posterior canal wall guide the choice between a canal-wall-up and a canal-wall-down (modified radical) mastoidectomy. Each critical erosion translates into a specific intra-operative warning:
- Facial canal erosion → the surgeon is forewarned that the facial nerve is exposed and must be protected; this changes consent and operative technique.
- Lateral semicircular canal fistula → alerts the surgeon to a labyrinthine breach risk, so disease over the fistula is removed last and with great care to preserve hearing and avoid a dead ear.
- Tegmen dehiscence → warns of dural exposure, CSF-leak risk and a route for intracranial spread.
- Ossicular erosion → informs the plan for ossicular reconstruction (ossiculoplasty) to restore hearing.
Pathway 3 — Safe CSOM and post-operative surveillance:
In quiescent mucosal CSOM without erosion, imaging may confirm that surgery can be limited (e.g. tympanoplasty without extensive mastoid work). After cholesteatoma surgery, non-EPI DWI MRI has transformed follow-up: a restricting focus signals residual or recurrent cholesteatoma, allowing targeted re-operation, while a negative DWI spares the patient a routine 'second-look' operation. This single application — imaging replacing diagnostic surgery — is a clear demonstration of how the right modality, correctly interpreted, improves care while reducing harm.
Imaging Findings in CSOM and Surgical Decisions
SELF-CHECK
A 25-year-old with cholesteatomatous CSOM is listed for mastoidectomy. The pre-operative HRCT temporal bone report states: 'non-dependent attic soft tissue with scutum erosion; dehiscence of the tympanic segment of the facial nerve canal; fistula of the lateral semicircular canal.' How should these findings change the surgical approach?
A. They are incidental; proceed with routine tympanoplasty alone without mastoid exploration
B. They warn that the facial nerve is exposed and that there is a labyrinthine fistula — the surgeon must protect the nerve and remove disease over the fistula last and with great care to avoid facial palsy and a dead ear
C. They mandate immediate IV thrombolysis before any surgery
D. They indicate the disease is purely mucosal 'safe' CSOM, so no special precautions are needed
Reveal Answer
Answer: B. They warn that the facial nerve is exposed and that there is a labyrinthine fistula — the surgeon must protect the nerve and remove disease over the fistula last and with great care to avoid facial palsy and a dead ear
Facial-canal dehiscence and a lateral semicircular canal fistula are the surgically critical erosions: they tell the surgeon the facial nerve is exposed (risk of intra-operative injury and facial palsy) and that the labyrinth is breached (risk of vertigo, sensorineural hearing loss and a dead ear). The disease over the fistula is removed last and with great care, and the consent and technique change accordingly. These are features of unsafe cholesteatomatous CSOM, not safe mucosal disease, and thrombolysis has no role here.
CLINICAL PEARL
Pearl 1 — Image the complication, not the infection. ASOM and quiescent safe CSOM are clinical diagnoses; reach for the scanner only when a red flag appears — post-auricular swelling (mastoiditis), facial palsy, vertigo (labyrinthitis) or any sign of intracranial spread. Reflex scanning of every discharging ear wastes radiation and money.
Pearl 2 — CT for bone, MRI (DWI) for the keratin. HRCT temporal bone answers 'what is eroded?' and gives the surgical roadmap; it cannot tell cholesteatoma from granulation because all soft tissue looks the same on CT. Non-echo-planar DWI MRI answers 'is this cholesteatoma?' — cholesteatoma restricts (bright DWI, low ADC), granulation does not.
Pearl 3 — Three erosions the surgeon dreads. When you read a CSOM HRCT, deliberately check the tegmen (intracranial route), the facial nerve canal (palsy/injury risk) and the lateral semicircular canal (fistula → dead-ear risk). Mentioning these three in your report is what makes it surgically useful.
Pearl 4 — DWI can replace the second-look operation. A negative non-EPI DWI after cholesteatoma surgery spares the patient a routine diagnostic re-operation; a restricting focus localises recurrence for targeted surgery.
Self-Assessment — Integrating Imaging into ASOM/CSOM Decisions
Work through these scenarios as if you are the clinician responsible for the imaging request and its interpretation. Write your reasoning before reading the discussion, and in each case state explicitly which modality you would use and how the findings would change management. This deliberate practice of linking the clinical picture to the scan and then to the decision is the exact skill RD7.2 assesses, and it rewards reasoning rather than rote recall.
Scenario A: A 6-year-old on day 6 of acute otitis media develops a tender, red post-auricular swelling that pushes the pinna forward, with persistent high fever despite oral antibiotics. What imaging, and why, and what would coalescent mastoiditis on the scan change?
Discussion: This is suspected acute (coalescent) mastoiditis — a complication of ASOM, and therefore now an indication for imaging. HRCT temporal bone is the first investigation; it would show opacified mastoid air cells with loss of their bony septa (coalescence) and any subperiosteal abscess, and contrast MRI/CT is added if intracranial spread is suspected (drowsiness, neck stiffness, focal signs). Coalescent mastoiditis or a subperiosteal abscess on the scan escalates management from intravenous antibiotics alone to cortical mastoidectomy with abscess drainage.
Scenario B: A 35-year-old with years of foul right-ear discharge and an attic perforation has an HRCT showing non-dependent soft tissue in Prussak's space, scutum erosion and erosion of the long process of the incus. The ENT surgeon asks whether this is cholesteatoma and whether the facial nerve is at risk. What do you advise?
Discussion: The HRCT pattern — non-dependent attic soft tissue, scutum erosion and ossicular erosion — is characteristic of attic (unsafe) cholesteatoma, but because CT cannot distinguish cholesteatoma from granulation, non-EPI DWI MRI is used to confirm it (cholesteatoma restricts: bright DWI, low ADC). The report must specifically comment on the facial nerve canal, the tegmen and the lateral semicircular canal; any dehiscence or fistula changes the operative caution and consent. The findings point to a mastoidectomy (canal-wall-up or canal-wall-down depending on extent and pneumatisation) with ossicular reconstruction for the eroded incus.
Scenario C: Two years after a canal-wall-up mastoidectomy for cholesteatoma, a patient is asymptomatic but due for surveillance. The clinic wants to know whether residual or recurrent disease is present without re-operating. What is the best investigation and how does the result direct management?
Discussion: Non-echo-planar (non-EPI) DWI MRI is the surveillance investigation of choice. A focus that restricts diffusion (bright on DWI, low ADC) indicates residual or recurrent cholesteatoma and directs targeted re-exploration; a negative DWI study spares the patient a routine 'second-look' operation. This is a clear example of imaging replacing diagnostic surgery — a recurring theme in how the correct modality, correctly read, improves care and reduces harm.