Page 4 of 11
RD7.2 | Imaging in Sensorineural Hearing Loss — SDL Guide
Learning Objectives
- Distinguish sensorineural from conductive hearing loss and identify which patterns of sensorineural hearing loss (SNHL) mandate imaging — asymmetric/unilateral, sudden, paediatric/congenital and vertiginous presentations.
- Justify MRI of the internal auditory meatus (IAM) and cerebellopontine angle (CPA) — with gadolinium and heavily T2-weighted sequences — as the modality of choice for retrocochlear SNHL, with vestibular schwannoma as the prototype.
- Justify HRCT temporal bone for bony and congenital causes of SNHL — cochlear malformations, enlarged vestibular aqueduct (EVA) and otosclerosis.
- Recognise the key imaging appearances of a vestibular schwannoma, an enlarged vestibular aqueduct, and cochlear nerve aplasia/hypoplasia.
- Integrate provided imaging findings into the management of SNHL — schwannoma surveillance versus treatment, congenital-cause counselling, and pre-cochlear-implant assessment.
INSTRUCTIONS
A patient who cannot hear in one ear, or a child who fails the newborn hearing screen, both have sensorineural hearing loss — but they need completely different scans. RD7.2 asks you to integrate imaging findings into the evaluation of SNHL, and the single most useful idea is this: image the nerve with MRI and the bone with CT, and let the clinical pattern tell you which. This module shows you when to image SNHL at all, how to choose between MRI and HRCT, the appearances you must recognise, and how each finding redirects management — from watching a small tumour to deciding whether a deaf child can receive a cochlear implant.
References
- Sutton's Textbook of Radiology and Imaging, 8th edition, Chapter on the Temporal Bone, IAM and Cerebellopontine Angle (textbook)
- Grainger & Allison's Diagnostic Radiology, 7th edition, Chapter on the Temporal Bone and Hearing Loss (textbook)
- AERB (Atomic Energy Regulatory Board, India) Safety Code and ALARA principles; MRI safety screening standards (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 48-year-old man notices over a year that he can no longer hear on the telephone with his right ear, and lately the room seems to spin when he turns quickly. His audiogram shows a unilateral high-frequency sensorineural loss with poor speech discrimination. His GP reassures him it is 'just age'. But age-related hearing loss is symmetrical — a one-sided sensorineural loss is a red flag until proven otherwise, and the question it raises cannot be answered by any examination of the ear. It needs a picture of the nerve. A gadolinium-enhanced MRI of the internal auditory meatus shows a small avidly enhancing mass growing out of the canal — a vestibular schwannoma. Caught early, it can be watched or treated with hearing-preserving surgery; missed, it grows to compress the brainstem. Knowing that an asymmetric SNHL means 'scan the nerve', and being able to read that scan, is the applied skill this module builds.
WHY THIS MATTERS
Hearing loss is one of the most common sensory disabilities worldwide, and sensorineural loss — from the cochlea, the cochlear nerve, or the central pathway — accounts for the majority of permanent hearing impairment. The NMC competency RD7.2 asks you to integrate provided imaging findings into the evaluation of sensorineural hearing loss — a knows-how (KH) skill. For the adult with an asymmetric or sudden SNHL, imaging is what excludes a treatable vestibular schwannoma before it endangers the brainstem; for the deaf child, imaging is what tells the surgeon whether a cochlear implant is even possible. Whether you become a physician who must decide when to refer, a paediatrician evaluating a child who fails newborn screening, or a surgeon planning an implant, the ability to match the pattern of hearing loss to the right scan — and to read it — is a recurring, high-stakes clinical skill.
RECALL
Before reading further, recall the anatomy and audiology the imaging depends on:
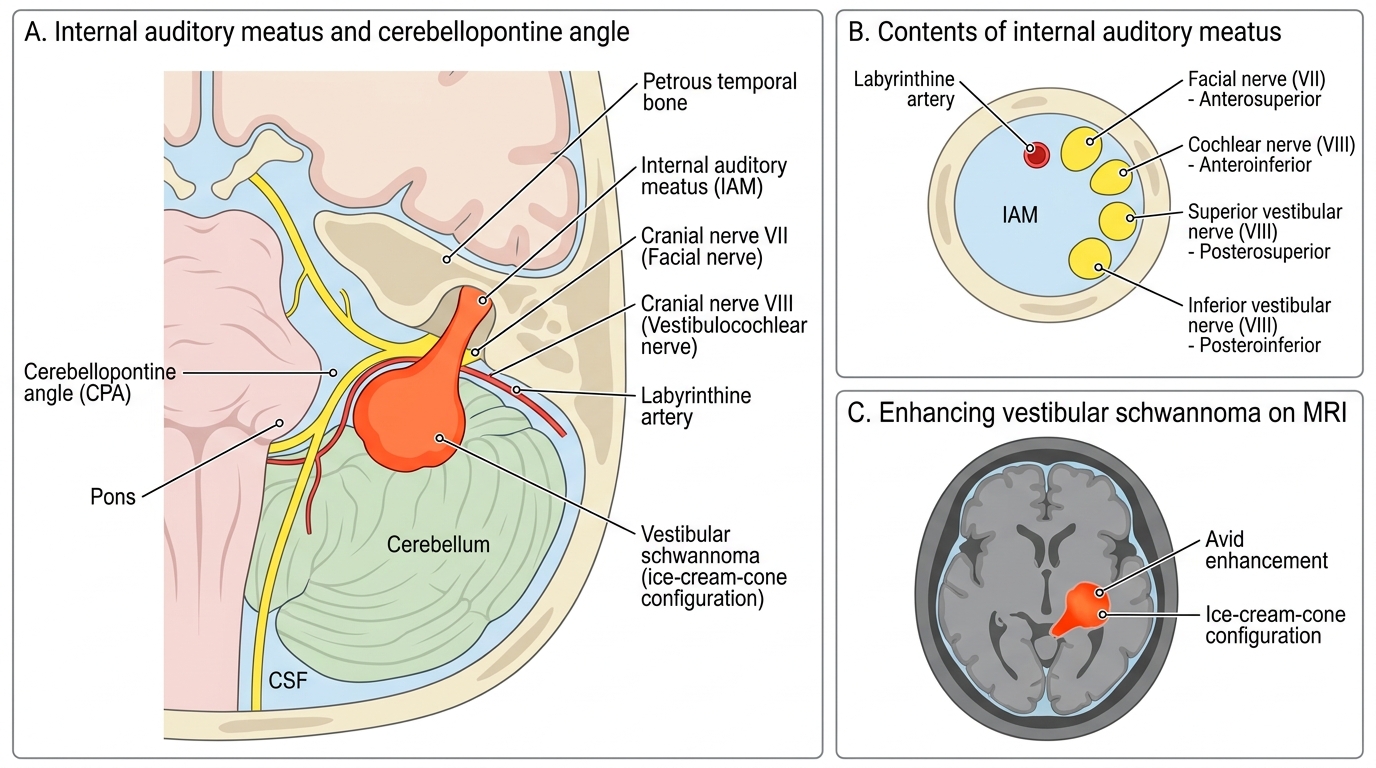
- The auditory pathway (from Anatomy/Physiology): sound is transduced in the cochlea (sensory), carried by the cochlear (auditory) division of the vestibulocochlear nerve, CN VIII, through the internal auditory meatus (IAM) and across the cerebellopontine angle (CPA) to the brainstem and central pathways. A lesion anywhere from the cochlea to the cortex causes sensorineural loss.
- Sensorineural vs conductive loss (from ENT): conductive loss arises in the external or middle ear (wax, perforation, ossicular disease) — Rinne negative, Weber lateralising to the affected ear; sensorineural (SNHL) arises in the cochlea or neural pathway — Rinne positive, Weber lateralising to the better ear. Pure-tone audiometry confirms the type and configuration.
- Retrocochlear vs cochlear: a cochlear (sensory) lesion is in the cochlea itself; a retrocochlear lesion is in the cochlear nerve or central pathway (e.g. vestibular schwannoma). Poor speech discrimination out of proportion to the pure-tone loss and an asymmetric pattern suggest a retrocochlear cause.
- CT density and MRI signal: bone is bright on CT (ideal for the bony labyrinth, cochlear malformations and the vestibular aqueduct); soft-tissue lesions and the fluid-filled inner ear and nerves are best shown on MRI — heavily T2-weighted sequences make the cochlea, semicircular canals and the nerves within the IAM stand out, and gadolinium reveals enhancing tumours.
Clinical Scenario — Which Patient with SNHL Gets a Scan
The first decision in sensorineural hearing loss is not which scan to order but whether to image at all, and that decision turns on the clinical pattern. The commonest SNHL by far is age-related (presbycusis), which is bilateral and broadly symmetrical; like most symmetrical SNHL of clear cause, it does not usually require imaging because a scan would not change management. Imaging in SNHL is targeted at the presentations where a structural lesion — a tumour, a malformation or a treatable abnormality — is plausible and would alter the patient's management. The clinician's task is therefore to recognise the SNHL 'red flags' that justify exposing the patient to imaging, and to know which red flag points to which modality. Getting this triage right avoids both missing a vestibular schwannoma and scanning every patient with ordinary age-related loss.
The SNHL presentations that mandate imaging are:
- Asymmetric or unilateral SNHL — the classic indication to exclude a vestibular schwannoma or other retrocochlear lesion; this is the single most important pattern to recognise.
- Sudden sensorineural hearing loss (SSNHL) — rapid (often overnight) loss; MRI is recommended to exclude a CPA/IAM lesion and central causes even though most cases are idiopathic.
- SNHL with vertigo, imbalance or other cranial-nerve signs — suggesting a CPA lesion compressing CN VIII/VII and the brainstem.
- Paediatric/congenital SNHL — a child failing newborn hearing screening or with progressive/fluctuating loss needs imaging to find a congenital cochlear malformation, an enlarged vestibular aqueduct (EVA) or cochlear nerve deficiency, and to plan rehabilitation.
- Pre-cochlear-implant assessment — any candidate for an implant is imaged to confirm a patent cochlea and an intact cochlear nerve.
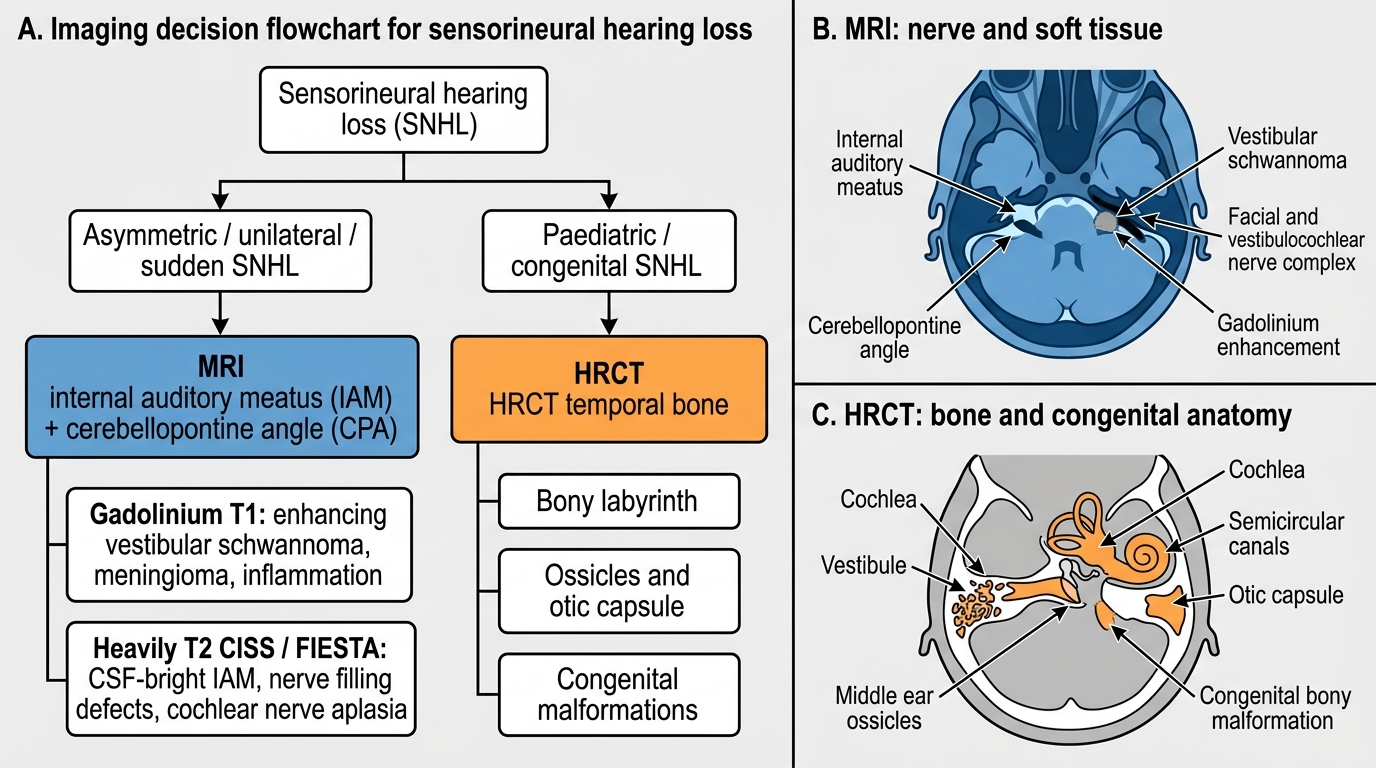
The key triage principle is simple and worth memorising: a retrocochlear or soft-tissue cause is suspected → MRI of the IAM/CPA; a bony or congenital cause is suspected → HRCT temporal bone. Asymmetric or sudden adult SNHL leans to MRI first; paediatric/congenital loss usually starts with HRCT (often complemented by MRI for the cochlear nerve).
Imaging Strategy in Sensorineural Hearing Loss
Imaging Strategy — MRI for the Nerve, HRCT for the Bone
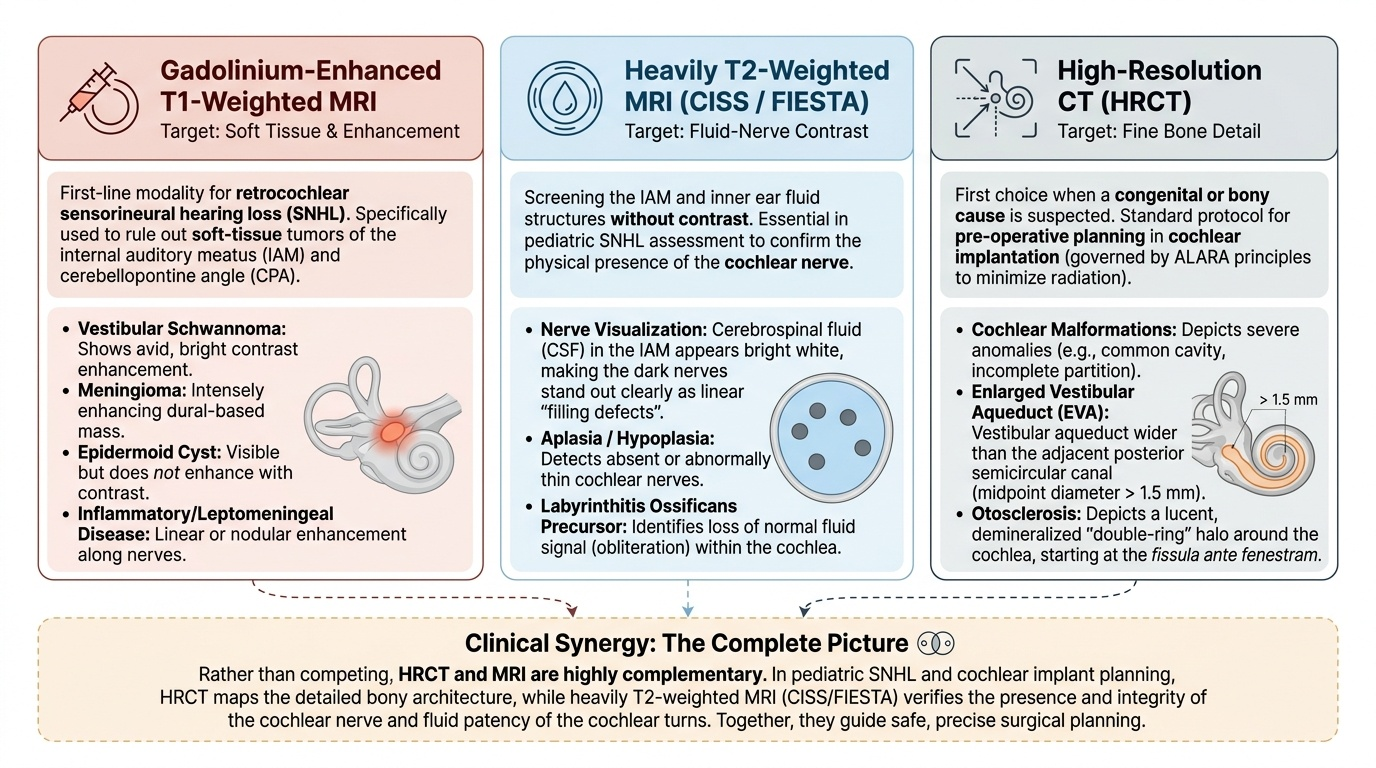
Modality choice in SNHL follows the same physical logic seen throughout temporal-bone imaging: MRI characterises soft tissue, nerves and fluid; CT characterises bone. Because the commonest serious, treatable cause of asymmetric SNHL is a soft-tissue tumour on a nerve, MRI of the internal auditory meatus and cerebellopontine angle is the modality of choice for retrocochlear SNHL. Two MRI components do the work. Gadolinium-enhanced T1 imaging is the reference standard for detecting a vestibular schwannoma, which enhances avidly; it also shows meningioma, the rare epidermoid (which does not enhance) and inflammatory or leptomeningeal disease. Heavily T2-weighted high-resolution sequences (CISS or FIESTA) make the cerebrospinal-fluid-filled IAM bright so that the cochlear and vestibular nerves stand out as dark filling structures; these sequences screen the IAM for a filling defect (a small schwannoma) without contrast and are essential for assessing cochlear nerve aplasia or hypoplasia in children. The fluid signal also outlines the membranous labyrinth, revealing obliteration (labyrinthitis ossificans precursor) or malformation.
HRCT temporal bone is the modality of choice when a bony or congenital cause is suspected. Its sub-millimetre bone-algorithm images resolve the bony labyrinth and reveal: cochlear malformations (from the severe common-cavity and incomplete-partition anomalies to a normal-looking cochlea); the enlarged vestibular aqueduct (EVA), the commonest imaging-detectable congenital cause of childhood SNHL, defined as a vestibular aqueduct wider than the adjacent posterior semicircular canal (midpoint diameter greater than about 1.5 mm); and otosclerosis, where otospongiotic foci produce a pericochlear lucent halo around the basal turn of the cochlea (the 'double-ring' sign), the primary focus lying at the fissula ante fenestram just anterior to the oval window, which can cause a sensorineural or mixed component. HRCT also maps the bony anatomy and cochlear patency needed before a cochlear implant.
The two modalities are complementary rather than competing: in paediatric SNHL, HRCT shows the bone and MRI (CISS/FIESTA) confirms the presence of the cochlear nerve, and the two together give the complete picture for implant planning. ALARA governs CT use — temporal-bone protocols are dose-optimised and CT is avoided when it will not change management, an especially important consideration in children — while MRI requires its own safety screening for contraindications such as non-MR-conditional pacemakers, certain cochlear implants and intra-ocular metallic foreign bodies. What MRI cannot do is resolve fine cortical bone (so it can miss subtle otosclerosis or a bony EVA edge); what CT cannot do is characterise the nerve or a small enhancing tumour — which is exactly why the clinical pattern drives the choice.
Provided image
SELF-CHECK
A 52-year-old woman reports two years of progressive hearing loss in the left ear only, with poor speech discrimination and occasional unsteadiness. Pure-tone audiometry confirms a unilateral sensorineural loss. The right ear is normal. What is the single most appropriate first imaging investigation?
A. HRCT temporal bone, to look for otosclerosis as the cause of the asymmetric loss
B. Gadolinium-enhanced MRI of the internal auditory meatus and cerebellopontine angle to exclude a vestibular schwannoma
C. Plain mastoid X-ray (Stenvers view) to screen the internal auditory meatus
D. No imaging; asymmetric sensorineural loss in this age group is almost always age-related
Reveal Answer
Answer: B. Gadolinium-enhanced MRI of the internal auditory meatus and cerebellopontine angle to exclude a vestibular schwannoma
Unilateral/asymmetric sensorineural hearing loss, especially with poor speech discrimination and imbalance, is the classic indication to exclude a retrocochlear lesion — most importantly a vestibular schwannoma at the IAM/CPA. Gadolinium-enhanced MRI of the IAM/CPA (with heavily T2 CISS/FIESTA) is the modality of choice. HRCT is for bony/congenital causes, not a nerve tumour; plain X-ray is obsolete and cannot resolve the IAM; and age-related loss is symmetrical, so a one-sided loss must not be dismissed as ageing.
Image Findings and Interpretation — Schwannoma, Malformations and the Vestibular Aqueduct
Interpreting SNHL imaging means matching the clinical pattern to a specific appearance, and recognising the few findings that actually change management rather than simply describing every structure. As with all temporal-bone work, the reading separates the soft-tissue and neural information from MRI from the bony information from HRCT, and the clinician must know what each modality shows for each cause before deciding what to do next. The findings cluster into retrocochlear masses (seen on MRI) and bony or congenital abnormalities (seen on HRCT), and a structured search — the internal auditory meatus and cerebellopontine angle first on MRI, then the cochlea, vestibule, semicircular canals and vestibular aqueduct on CT — ensures that nothing important is missed in a patient whose only complaint is that they cannot hear. Reading in this fixed sequence, every time, is what prevents a small intracanalicular tumour or a subtle aqueduct from being overlooked.
Retrocochlear causes — what MRI shows:
- Vestibular schwannoma (acoustic neuroma): the prototype. On gadolinium-enhanced T1 it is an avidly enhancing mass centred on the IAM; when it extends into the CPA it has the classic 'ice-cream-cone' shape (the cone in the canal, the scoop in the angle). On heavily T2 (CISS/FIESTA) it appears as a filling defect within the bright CSF of the IAM. Larger tumours widen the porus acusticus and indent the brainstem.
- Other CPA lesions: a meningioma enhances avidly too but is centred on the dura with a broad base and a dural tail, and is usually eccentric to the IAM; an epidermoid follows CSF on T1/T2, does not enhance, and characteristically restricts on DWI (distinguishing it from an arachnoid cyst).
Cochlear and bony/congenital causes — what HRCT (± MRI) shows:
- Cochlear malformations: a spectrum from the severe (common cavity, incomplete partition) to subtle dysplasias; HRCT shows the bony cochlear turns and any deficiency.
- Enlarged vestibular aqueduct (EVA): the commonest imaging-detectable congenital cause of paediatric SNHL — the vestibular aqueduct is wider than the adjacent posterior semicircular canal (midpoint diameter greater than about 1.5 mm) on HRCT; often associated with an enlarged endolymphatic sac on MRI and with fluctuating/progressive loss.
- Cochlear nerve aplasia/hypoplasia: assessed on heavily T2 (CISS/FIESTA) oblique-sagittal images through the IAM — an absent or small cochlear nerve in the anteroinferior quadrant.
- Otosclerosis: pericochlear lucency (otospongiotic foci) classically around the basal turn of the cochlea on HRCT — the 'double-ring' sign — with the primary focus at the fissula ante fenestram, which can produce a sensorineural or mixed loss (cochlear otosclerosis).
- Labyrinthitis ossificans: loss of the normal fluid signal in the cochlea on T2 with bony in-filling on CT, important to detect before it obliterates the cochlea in a potential implant candidate.
Vestibular Schwannoma at the Internal Auditory Meatus and Cerebellopontine Angle
SELF-CHECK
A 3-year-old who failed newborn hearing screening and has fluctuating, progressive bilateral sensorineural hearing loss undergoes HRCT temporal bone. The report describes the vestibular aqueduct as wider than the adjacent posterior semicircular canal, with a midpoint diameter of about 2 mm. What is the diagnosis and one important piece of counselling that follows?
A. Vestibular schwannoma; arrange urgent gadolinium MRI and neurosurgical referral
B. Enlarged vestibular aqueduct; advise avoidance of head trauma and contact sports as these can precipitate sudden hearing drops, and plan audiological rehabilitation/implant if loss progresses
C. Otosclerosis; start sodium fluoride and plan stapedectomy
D. Normal variant of no clinical significance; no follow-up required
Reveal Answer
Answer: B. Enlarged vestibular aqueduct; advise avoidance of head trauma and contact sports as these can precipitate sudden hearing drops, and plan audiological rehabilitation/implant if loss progresses
A vestibular aqueduct wider than the posterior semicircular canal (or midpoint >~1.5 mm) on HRCT defines an enlarged vestibular aqueduct (EVA) — the commonest imaging-detectable congenital cause of paediatric SNHL, typically causing fluctuating/progressive loss. Counselling includes avoiding head trauma and contact sports (minor head injury can precipitate sudden hearing deterioration) and planning audiological rehabilitation, with cochlear implantation if loss becomes severe. It is not a schwannoma (a retrocochlear tumour on MRI) or otosclerosis, and it is clinically significant, not a benign variant.