Page 7 of 14
RD2.2 | Choosing the Appropriate Imaging Modality Across Patient Groups — SDL Guide
Learning Objectives
- Select the correct first-line imaging modality for the broad pathology types — infection, tumour, trauma and congenital/structural disease.
- Select the correct modality by body part and system — CNS, head and neck, chest, abdomen and extremities.
- Adapt the modality choice for adults, children and pregnant women, accounting for radiation, sedation and contrast considerations.
- Explain what the chosen modality is expected to demonstrate and why it answers the clinical question.
- Justify how appropriate modality selection changes diagnostic yield, time-to-treatment and patient harm.
INSTRUCTIONS
Once you know how the modalities work and whether a patient is safe to undergo them, the decisive clinical skill is choosing the RIGHT one for the problem in front of you. The correct choice is found by crossing two questions — what is the likely pathology and where is it, and who is the patient (adult, child, or pregnant) — and selecting the modality that answers the question with the least harm. This module builds that selection reasoning across pathology types, body systems and patient groups, so that 'order a scan' becomes 'order the scan that will change this patient's management.'
References
- Sutton's Textbook of Radiology, 6th edition (modality selection by region and pathology) (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition (Principles of Imaging Strategy) (textbook)
- ACR Appropriateness Criteria (modality-selection evidence base) (guideline)
- Atomic Energy Regulatory Board (AERB) referral guidelines for diagnostic imaging, India (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients arrive in casualty within an hour. A 30-year-old man is brought in after a high-speed road-traffic accident, hypotensive, with a rigid abdomen. A 4-year-old child has had three days of fever and right-iliac-fossa pain. A 28-year-old woman, 12 weeks pregnant, has sudden severe flank pain and visible haematuria. Each needs imaging — but the right modality is different for each, and choosing wrongly causes harm: a slow study delays the trauma laparotomy, an unnecessary CT irradiates the child, an ionising study endangers the fetus. The trauma patient needs the speed and sensitivity of CT; the child and the pregnant woman are better served first by ultrasound, which carries no radiation. Modality selection is not a question of which scanner is best in the abstract — it is the clinical judgement of matching the tool to the problem and the patient.
WHY THIS MATTERS
Competency RD2.2 requires you to select the correct imaging modality and procedure for the broad pathology type (infection, tumour, trauma, congenital) and the body part/system (CNS, head and neck, chest, abdomen and extremities) in adults, children and pregnant women — mindful of the unique needs of paediatric patients with respect to radiation and sedation. This is one of the most frequently tested and most clinically consequential reasoning skills in final-year medicine, because the requesting clinician makes this choice many times every day. A modality chosen by habit or availability rather than by the clinical question wastes resources at best and harms patients at worst: cumulative radiation in children, delayed diagnosis when an insensitive modality is chosen for a time-critical problem, or fetal exposure that a non-ionising study would have avoided. The selection framework you build here is examined in clinical postings and applied on every ward round that begins with 'what imaging should we order?'
RECALL
Before reading further, bring to mind the foundations this module builds on:
- Ionising vs non-ionising modalities: X-ray, fluoroscopy, CT and nuclear medicine use ionising radiation; ultrasound and MRI do not. This dichotomy drives the choice in children and pregnancy.
- Relative doses: a chest X-ray is ~0.02 mSv, a CT abdomen-pelvis ~8–10 mSv — roughly 400–500 times higher — which is why CT is not a default in the radiosensitive.
- What each modality is good at: USG for real-time soft-tissue/fluid/biliary/renal/obstetric assessment; CT for fast cross-sectional detail in trauma and acute haemorrhage; MRI for superior soft-tissue and CNS/cord contrast; X-ray for chest and bone; nuclear medicine for functional information.
- Suitability screening (RD2.1): pregnancy, renal function, allergies and implants must be screened before the chosen study.
- Paediatric considerations: children are more radiosensitive and may need sedation for MRI/CT because the studies require stillness.
If any of these feel unfamiliar, a quick review of the modality-principles and suitability-screening SDLs before continuing will make the selection logic below much clearer.
The Clinical Scenario — Two Questions That Decide Every Imaging Request
Every imaging request begins with a clinical scenario, and the correct modality is found not by ranking scanners in the abstract but by interrogating that scenario with two questions. The first question is about the clinical problem: what broad pathology type is suspected — infection, tumour, trauma, or a congenital/structural abnormality — and where is it, in which body part or system (CNS, head and neck, chest, abdomen and pelvis, or the extremities)? The second question is about the patient: is this an adult, a child, or a pregnant woman? Crossing these two axes yields the appropriate first-line modality, because the right tool for a given pathology in a given region can change once the patient group introduces a radiation or sedation constraint. This is the structure competency RD2.2 demands, and learning to ask both questions in sequence — problem first, patient second — converts modality selection from guesswork into a defensible clinical decision.
The modalities being selected among can be held in two groups, which is the lens through which the patient axis exerts its influence:
- Non-ionising modalities — ultrasound (USG) and MRI — carry no radiation risk and are therefore preferred whenever they answer the clinical question, especially in children and pregnant women.
- Ionising modalities — X-ray, fluoroscopy, CT and nuclear medicine — are chosen when their speed, sensitivity, or specific information is decisive (trauma, acute haemorrhage, chest and bone), but their use must be justified, particularly in the radiosensitive.
The governing rule that emerges is to choose the modality that answers the clinical question with the least harm: when a non-ionising study answers it as well, it is preferred; when only an ionising study will do — as in acute polytrauma or suspected intracranial haemorrhage — it is chosen deliberately and justified.
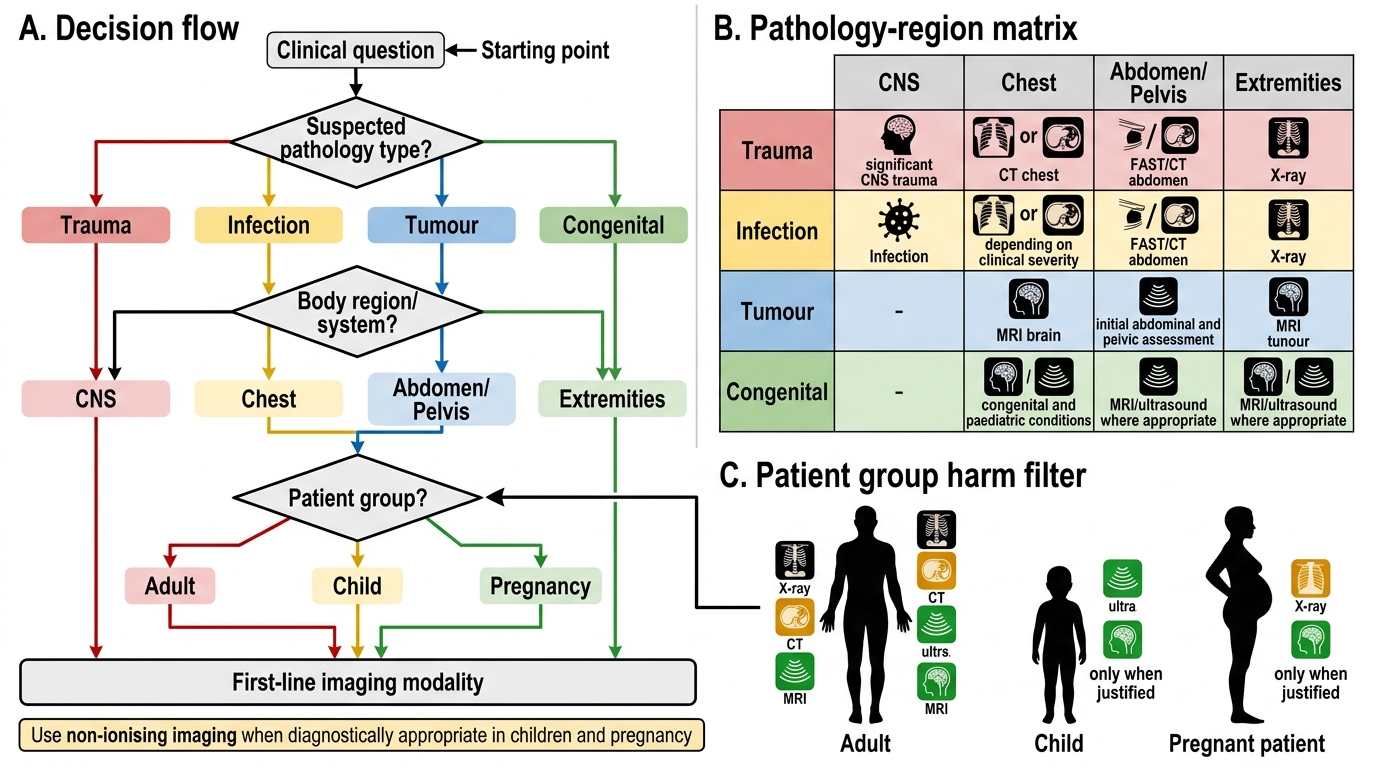
Imaging Modality Selection Flowchart
Imaging Strategy — Matching Modality to Pathology Type and Body System
With the clinical scenario framed, the imaging strategy assigns a first-line modality by matching the suspected pathology and its location to the modality whose physical strengths answer that question. The reasoning is consistent: choose the modality with the right tissue contrast, spatial or temporal resolution, and acceptable harm for the problem at hand. The patterns below are grounded in AERB referral guidance and the ACR Appropriateness Criteria, and they recur across clinical practice; they should be learned as defaults that a specific clinical context can override, not as rigid rules. Working through the broad pathology types and the major body systems in turn builds a reliable mental map that you can apply to almost any request you will encounter on the ward or in casualty.
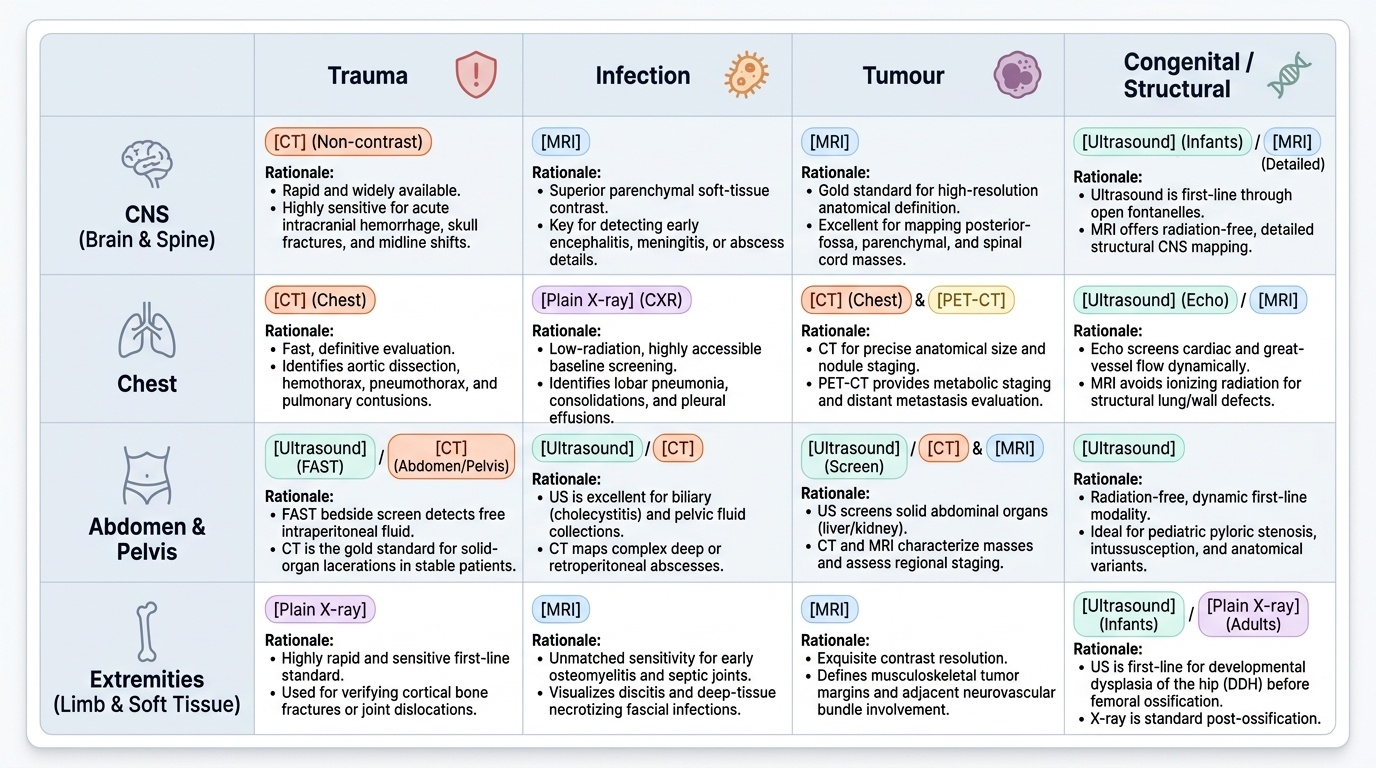
By broad pathology type:
- Trauma: CT is first-line for significant blunt trauma (head, chest, abdomen/pelvis) because it is fast and highly sensitive for haemorrhage and solid-organ injury; plain X-ray remains first-line for suspected limb fractures. Focused ultrasound (FAST) is a rapid bedside adjunct for free intraperitoneal fluid, especially in children and pregnancy.
- Infection: the modality follows the site — chest X-ray for pneumonia, ultrasound for an abdominal/pelvic collection or abscess, MRI for osteomyelitis/discitis and soft-tissue infection, and CT where deep collections need precise mapping.
- Tumour: ultrasound often screens superficial and abdominal organs; CT and MRI characterise and stage (MRI for CNS, pelvic and soft-tissue tumours; CT for chest and abdominal staging); nuclear medicine and PET-CT add functional/whole-body staging information.
- Congenital/structural: ultrasound is first-line antenatally and in infants (e.g. developmental dysplasia of the hip before ossification), with MRI for detailed CNS and soft-tissue anatomy and CT reserved for bony detail.
By body system:
- CNS: non-contrast CT first for acute haemorrhage and acute trauma; MRI for parenchymal, posterior-fossa, cord and most non-acute pathology (MRI with diffusion-weighted imaging is most sensitive for early ischaemic stroke).
- Head and neck: CT for bony/sinus/acute pathology; MRI for soft-tissue masses and skull-base/perineural detail; ultrasound for thyroid, salivary glands and neck nodes.
- Chest: plain chest X-ray first-line; CT (including CT pulmonary angiography for suspected pulmonary embolism) for further characterisation.
- Abdomen and pelvis: ultrasound first-line for biliary, renal and pelvic/obstetric assessment; CT for acute abdomen, trauma and staging; MRI for hepatobiliary, pelvic and soft-tissue characterisation.
- Extremities: plain X-ray first-line for fractures and bony pathology; MRI for soft-tissue, cartilage, marrow and occult fractures; ultrasound for tendons, effusions and superficial masses.
Provided image
SELF-CHECK
A 55-year-old man presents with sudden-onset dense right-sided weakness 40 minutes ago. The team needs to exclude intracranial haemorrhage before considering thrombolysis. What is the appropriate first-line modality?
A. MRI brain with diffusion-weighted imaging
B. Non-contrast CT head
C. Carotid Doppler ultrasound
D. Plain skull X-ray
Reveal Answer
Answer: B. Non-contrast CT head
Non-contrast CT head is the first-line modality in hyperacute stroke because it is fast, widely available, and highly sensitive for acute intracranial haemorrhage — the critical exclusion before thrombolysis. MRI with DWI is more sensitive for the early ischaemic infarct itself but is slower and less accessible in the hyperacute thrombolysis window; it is used to characterise the infarct, not to make the initial haemorrhage-exclusion decision. Carotid Doppler and skull X-ray do not answer the acute question.
Modality Choice Across Patient Groups — Adults, Children and Pregnancy
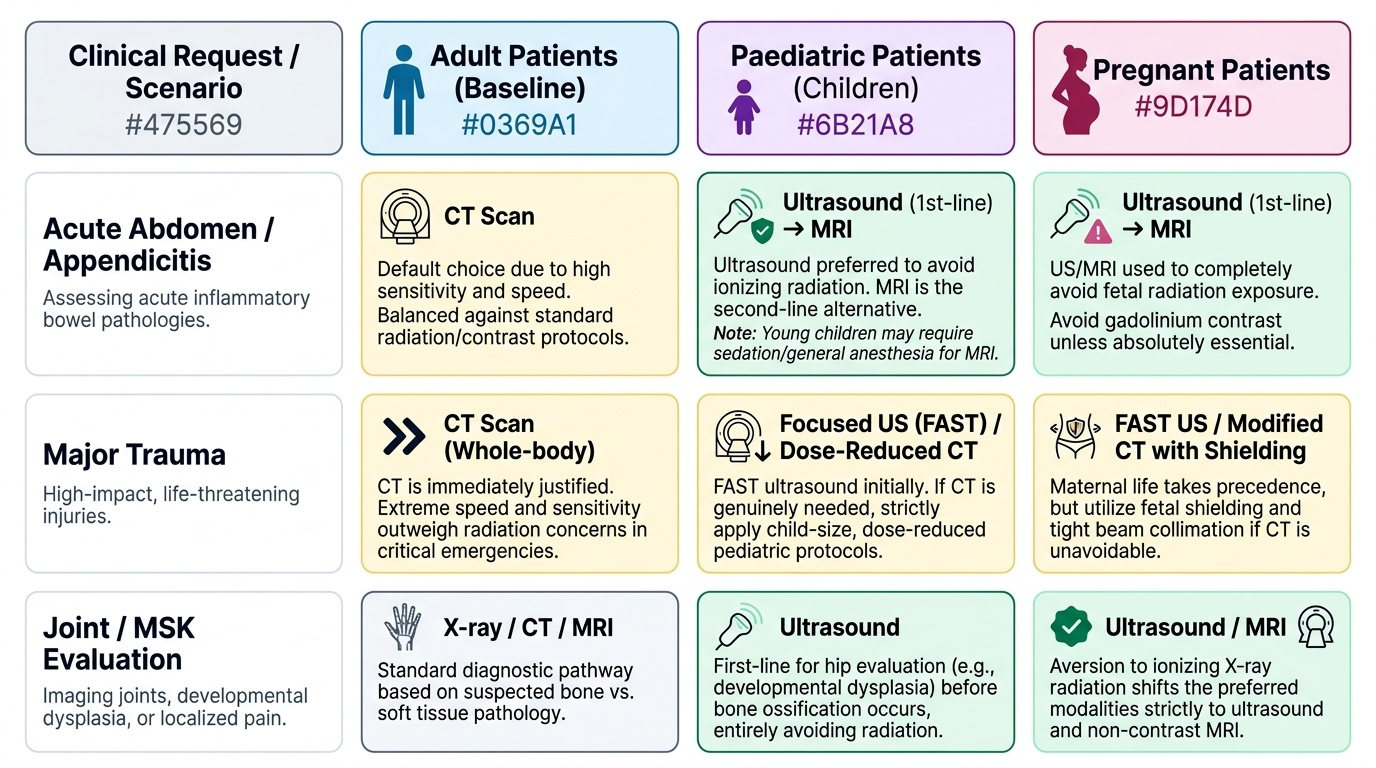
The patient axis can override the default modality, and competency RD2.2 specifically requires you to be mindful of the unique needs of paediatric patients with respect to radiation and sedation, as well as the constraints of imaging in pregnancy. The reasoning is that the same pathology in a child or a pregnant woman carries an added cost on the ionising side of the ledger — greater radiosensitivity in the child, fetal exposure in pregnancy — so the threshold to choose a non-ionising modality is lower and the justification for an ionising one must be stronger. The selection logic does not change (problem first, patient second), but the patient group shifts the preferred answer toward ultrasound and MRI wherever they can answer the question. The considerations for each group are set out below.
- Adults: the default modality maps directly from pathology and region, balanced against the radiation and contrast screen; speed and sensitivity (e.g. CT in polytrauma) often justify ionising studies when clinically decisive.
- Children: children are more radiosensitive (rapidly dividing tissues; a long lifetime over which a radiation-induced cancer may manifest), so ultrasound and MRI are preferred wherever feasible — ultrasound is first-line for paediatric appendicitis, intussusception, hip (developmental dysplasia before ossification) and many abdominal problems. When CT is genuinely needed, child-size dose-reduced protocols are used. Sedation is a distinct paediatric consideration: MRI and (less often) CT require the child to stay still, so young children may need sedation or general anaesthesia, which carries its own risk and influences whether and when the study is done.
- Pregnant women: the fetus is the most radiosensitive subject, so non-ionising modalities are strongly preferred — ultrasound first, then MRI (avoiding gadolinium where possible) for further characterisation. If an ionising study is genuinely necessary for the mother's care, it proceeds with the lowest feasible dose and shielding after weighing maternal benefit against the small fetal risk; imaging remote from the fetus (e.g. a shielded chest X-ray) delivers a negligible fetal dose and should not be withheld when needed.
Provided image
SELF-CHECK
A 4-year-old child presents with 48 hours of fever and right-iliac-fossa pain; appendicitis is suspected clinically. Which first-line modality best fits the pathology, body region and patient group?
A. Contrast-enhanced CT abdomen
B. Abdominal ultrasound
C. Plain abdominal X-ray
D. MRI abdomen under general anaesthesia
Reveal Answer
Answer: B. Abdominal ultrasound
Ultrasound is the appropriate first-line modality for suspected paediatric appendicitis: it carries no ionising radiation (decisive in a radiosensitive child), needs no sedation, and can demonstrate a non-compressible, inflamed appendix and secondary signs. CT delivers significant radiation and is reserved for equivocal cases. Plain X-ray has poor sensitivity for appendicitis. MRI is an option in equivocal cases but is slower, less accessible, and may require sedation in a young child — making ultrasound the correct initial step.