Page 5 of 14
RD1.1 | Core Principles of X-ray, Fluoroscopy, CT, Ultrasound, Nuclear Medicine and MRI — SDL Guide (Part 2)
Radiation Safety — ALARA, AERB Regulation and Protection Principles
Ionising radiation at diagnostic doses causes stochastic risks (principally carcinogenesis and hereditary effects), for which there is no proven safe threshold — the risk is assumed to be proportional to dose even at low levels. This is the scientific basis of the ALARA principle (As Low As Reasonably Achievable): every ionising procedure must use the minimum dose that achieves diagnostic quality, and the procedure must be clinically justified.
In India, ionising radiation in diagnostic settings is regulated by the Atomic Energy Regulatory Board (AERB), established under the Atomic Energy Act 1962. The AERB issues licences for X-ray equipment and CT scanners, sets dose-reference levels for common procedures, and mandates that facilities have qualified medical physicists perform quality-assurance testing. This is distinct from the US Nuclear Regulatory Commission (NRC) or the ICRP (International Commission on Radiological Protection), which issues dose limits as recommendations but is NOT a national regulator for India.
Three practical protection strategies — applicable to both patients and radiology staff — are:
- Time: minimise the duration of exposure; in fluoroscopy this means limiting screening time and using pulsed rather than continuous fluoroscopy.
- Distance: radiation intensity follows the inverse-square law; doubling the distance from the source reduces dose to one-quarter. Staff step back during fluoroscopy acquisitions.
- Shielding: lead aprons (0.5 mm Pb equivalent) protect the torso; thyroid shields protect the neck; lead glass screens protect control-room personnel; gonadal shields are used in pelvic X-rays where they do not obscure the area of interest.
Special populations requiring heightened justification:
- Paediatric patients: rapidly dividing cells are more radiosensitive; 'child-size' protocols reduce dose dramatically.
- Pregnant patients: the fetus is the most vulnerable organ. The AERB and ICRP advise that if a diagnostic procedure is clinically necessary during pregnancy it may proceed with appropriate shielding and technique optimisation; the theoretical fetal risk from diagnostic doses is small but must be explained to the patient.
- Reproductive-age women: the 'ten-day rule' (pelvic irradiation only in the first 10 days of the menstrual cycle) has largely been replaced by case-by-case clinical justification, but pregnancy must always be excluded before pelvic CT or fluoroscopy.
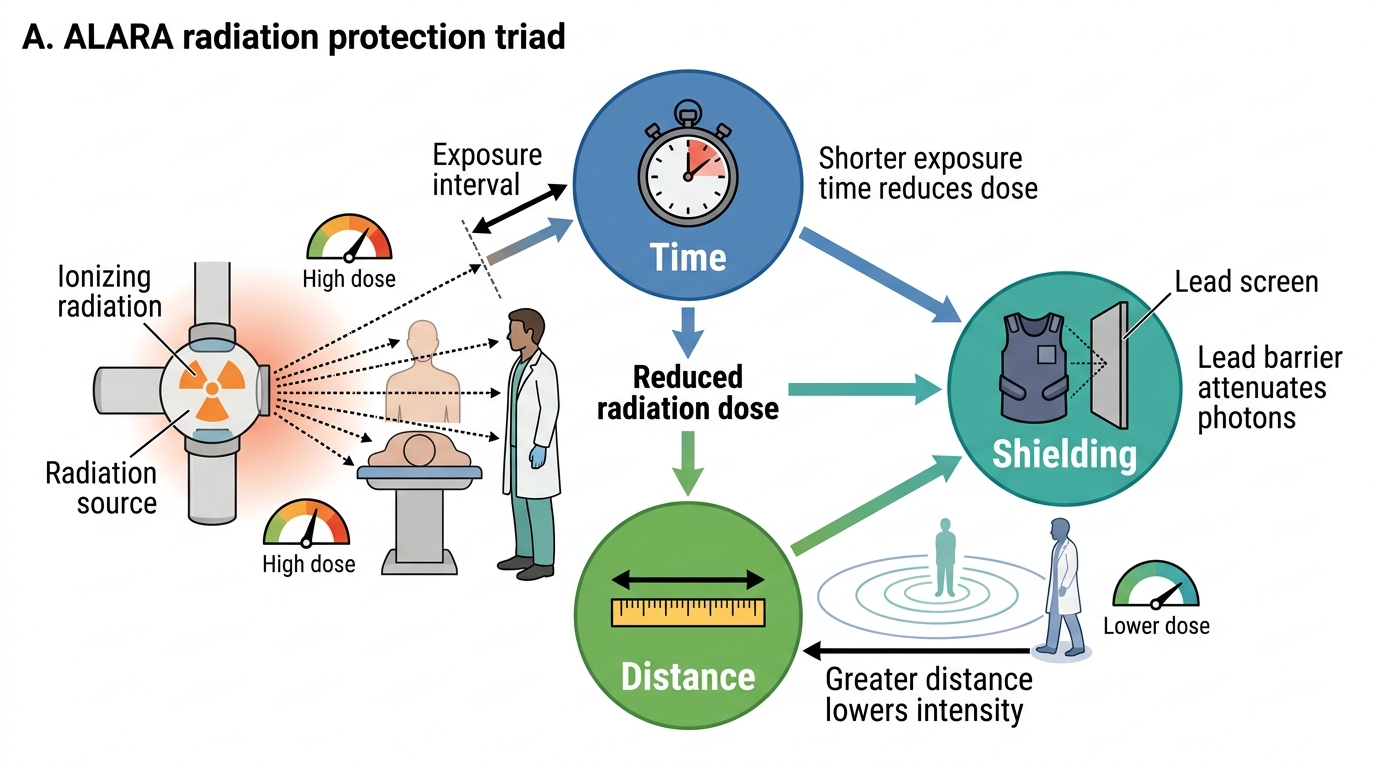
ALARA Radiation Protection Triad
Contrast Agents — Iodinated and Gadolinium: Indications, Cautions and Contraindications
Contrast enhancement is integral to many CT and MRI examinations, and the requesting clinician — not only the radiologist — must know the safety parameters before ordering a contrast study. Contrast reactions and contrast-induced renal injury are preventable harms; the pre-contrast checklist (renal function, prior reaction history, concurrent nephrotoxic drugs, and hydration status) is a mandatory pre-procedure step that falls within the clinical doctor's responsibility at the point of ordering. Two families of contrast agents are used in clinical imaging: iodinated agents for CT and fluoroscopy, and gadolinium-based agents for MRI. Their mechanisms, routes of excretion, and safety profiles differ substantially — they are not interchangeable.
Iodinated contrast agents (used in CT, fluoroscopy, and angiography) increase attenuation of X-ray photons in perfused structures (blood vessels, tumour blush, enhancing abscesses). They are hyperosmolar (ionic agents) or near-iso-osmolar (modern low-osmolality non-ionic agents such as iohexol, iopamidol), and are excreted renally.
Key safety considerations:
- Renal function: iodinated contrast can precipitate contrast-associated acute kidney injury (CA-AKI), particularly at eGFR <30 mL/min/1.73 m². At eGFR 30–44, shared-decision with the radiologist and nephrology team is warranted, weighing the diagnostic need against risk, with hydration protocols. At eGFR <30, intravenous iodinated contrast is used only when no alternative achieves the diagnostic goal.
- Metformin: there is a risk of lactic acidosis if metformin is retained in the setting of CA-AKI. Current guidance (European Society of Urogenital Radiology) advises withholding metformin from the time of contrast administration and for 48 hours afterward in patients with eGFR <60 or when large volumes of contrast are given, resuming only after renal function is confirmed stable.
- Prior contrast reaction: a previous severe (anaphylactoid) reaction to iodinated contrast requires pre-medication with corticosteroids and antihistamines, or alternative imaging. A prior mild reaction (nausea, urticaria) does not absolutely preclude contrast but warrants pre-medication and radiologist involvement.
- Thyroid disease: iodinated contrast may precipitate hyperthyroidism in susceptible patients (Jod–Basedow effect); relevant when large doses are given.
Gadolinium-based contrast agents (GBCAs) are used in MRI to shorten T1 relaxation time, producing bright enhancement on T1-weighted sequences.
- Renal risk — nephrogenic systemic fibrosis (NSF): gadolinium deposition in severe renal failure (eGFR <30) can cause NSF, a rare but debilitating fibrosing dermopathy. Linear (ionic and non-ionic) GBCAs carry higher NSF risk than macrocyclic agents. GBCAs are avoided or used with macrocyclic agents only in eGFR <30, and are absolutely contraindicated in dialysis-dependent patients unless the clinical benefit is overwhelming.
- Gadolinium does NOT contain iodine; it is safe in documented iodine/iodinated-contrast allergy.
SELF-CHECK
A 65-year-old diabetic patient on metformin is scheduled for a CT pulmonary angiogram (CTPA) with iodinated contrast. His eGFR is 38 mL/min/1.73 m². What is the MOST appropriate pre-procedure management regarding metformin?
A. Continue metformin throughout; eGFR of 38 does not require any modification
B. Withhold metformin from the time of contrast and for 48 hours after, resuming only if renal function is stable
C. Permanently discontinue metformin before any contrast administration
D. Replace metformin with insulin for 7 days before the procedure
Reveal Answer
Answer: B. Withhold metformin from the time of contrast and for 48 hours after, resuming only if renal function is stable
Current ESUR guidance advises withholding metformin at the time of iodinated contrast administration and for 48 hours afterward in patients with eGFR <60 (or when large contrast volumes are used), to avoid lactic acidosis if contrast-associated AKI occurs. Metformin is then resumed after confirming stable renal function. Permanent discontinuation is not warranted. Insulin substitution for 7 days is not standard guidance.
Clinical Significance — Choosing the Right Modality and Regulatory Framework
The clinical applied significance of understanding modality principles is the ability to construct an appropriate imaging strategy for each patient presentation without defaulting to the most powerful or most expensive option. The principle of referral optimisation — asking whether the examination will change management and whether this is the lowest-dose option that answers the clinical question — is not a bureaucratic constraint but a core clinical competency enshrined in AERB referral guidelines and supported by the ACR Appropriateness Criteria used globally. A clinician who reflexively orders CT for every abdominal presentation exposes patients to cumulative radiation they may not need, whereas a clinician who fails to order CT in acute polytrauma or suspected pulmonary embolism may cause fatal diagnostic delay. The judgment between these extremes is exercised modality by modality, case by case, and requires the foundational understanding this SDL has built.
A practical first-line modality map, grounded in RD known-trap guidance, is as follows:
| Clinical Scenario | First-Line Modality | Rationale |
|---|---|---|
| Acute trauma (abdomen, chest) | CT with contrast | Fastest definitive staging of solid-organ injury; polytrauma requires speed |
| Suspected biliary colic / gallstones | Ultrasound | No radiation; real-time assessment of gallbladder wall and bile duct |
| Obstetric dating and anomaly scan | Ultrasound | No ionising radiation; real-time fetal biometry |
| Renal/ureteric colic (non-pregnant adult) | CT KUB (non-contrast) | High sensitivity for calculi; faster than IVP |
| Renal colic in pregnancy | Ultrasound (then MRI if inconclusive) | Avoid ionising radiation to fetus |
| Suspected intracranial haemorrhage (acute) | Non-contrast CT head | Fast; very sensitive for acute blood |
| Early ischaemic stroke characterisation | MRI with DWI | DWI detects infarct within minutes–hours; CT normal in early infarct |
| Spinal cord compression | MRI spine | Superior soft-tissue and cord detail; CT myelogram if MRI contraindicated |
| Chest X-ray first-line | Plain X-ray | Pneumonia, pneumothorax, cardiomegaly — low-dose first step |
| Paediatric hip (Perthes, DDH) | Ultrasound (infants); X-ray pelvis (older child) | Avoid CT radiation; ultrasound for pre-ossification |
The AERB regulatory framework interacts with clinical practice through three instruments: (1) Referral guidelines — evidence-based recommendations on when imaging is appropriate, similar to the ACR Appropriateness Criteria; (2) Dose reference levels (DRLs) — national benchmarks per procedure that facilities must not routinely exceed; (3) Facility licensing — all diagnostic X-ray and CT equipment must be registered, and operators (radiographers, radiologists) must hold AERB-recognised qualifications.
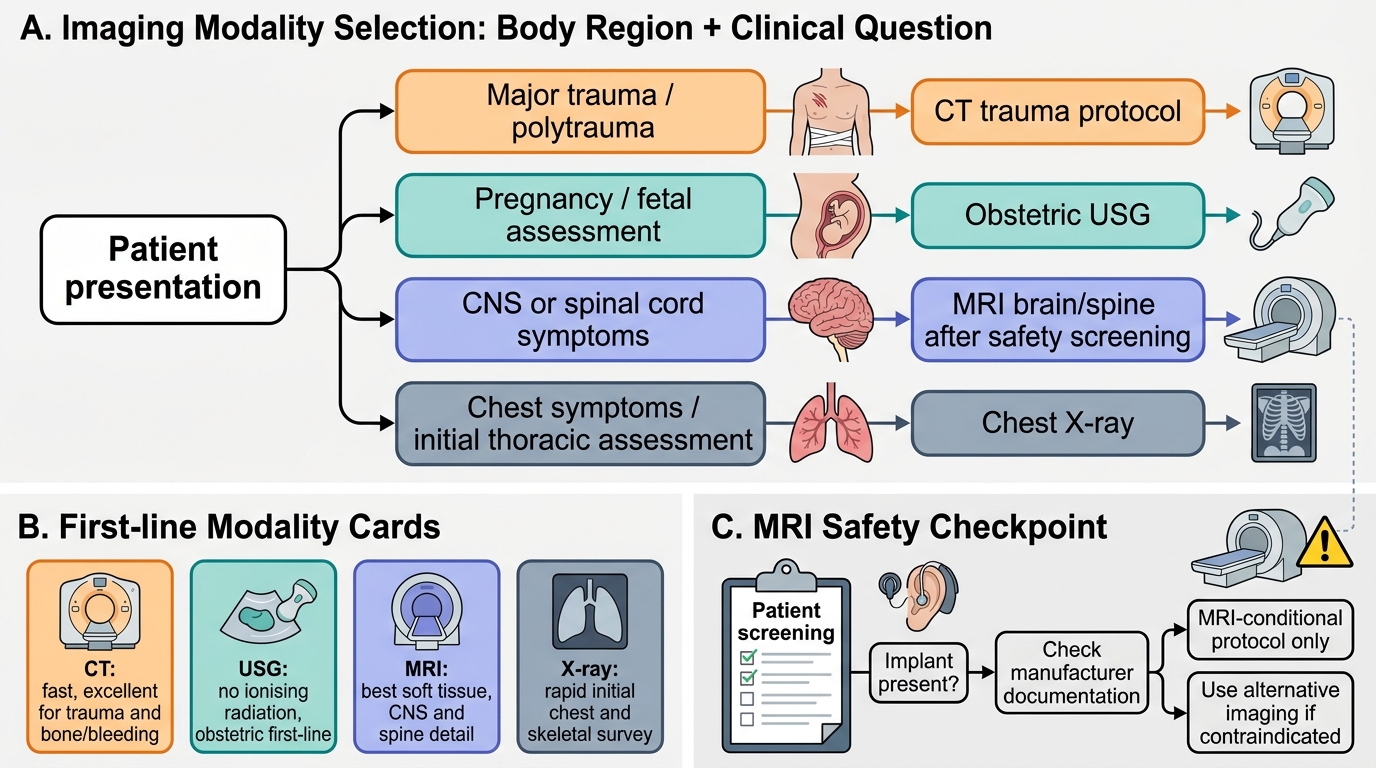
Clinical Imaging Modality Selection Flowchart
SELF-CHECK
A 35-year-old woman presents with 6 weeks of progressive leg weakness and urinary urgency. MRI lumbar spine is requested. On screening, she reports having a cochlear implant placed 3 years ago. What is the correct course of action?
A. Proceed with MRI as cochlear implants are generally MRI-safe
B. Request the implant manufacturer's documentation to determine if the specific device is MRI-conditional before proceeding
C. Perform MRI at 3 Tesla rather than 1.5 Tesla to reduce the magnetic risk
D. Switch to CT myelogram as the alternative without restriction
Reveal Answer
Answer: B. Request the implant manufacturer's documentation to determine if the specific device is MRI-conditional before proceeding
Cochlear implants are a recognised MRI contraindication UNLESS the specific device is certified as MRI-conditional and the manufacturer's protocol is followed (specific field strength, head orientation, magnet management). Assuming all cochlear implants are MRI-safe is dangerous. Higher field strength does not reduce ferromagnetic risk — it typically increases it. CT myelogram is a reasonable fallback if the implant is a true contraindication, but the first step is always to identify the specific device and check its MRI status.
CLINICAL PEARL
Pearl 1 — AERB vs NRC: Indian students frequently confuse the regulatory authority. For India, the AERB (Atomic Energy Regulatory Board) is the radiation regulator under the Atomic Energy Act 1962. The US NRC and ICRP are international bodies; do not cite them as the Indian authority in examinations or clinical practice.
Pearl 2 — 'MRI has no contraindications' is always wrong. A standard examination question and a genuine patient-safety trap. Always screen for pacemakers/ICDs, cochlear implants, ferromagnetic intra-ocular foreign bodies, and aneurysm clips before sending a patient into the MRI suite.
Pearl 3 — CT dose perspective: A CT abdomen delivers roughly 400–500× the dose of a chest X-ray (~8–10 mSv vs ~0.02 mSv). This does not make CT dangerous in isolation, but it makes the question 'is CT the right first step?' clinically important — especially in young patients and children.
Self-Assessment — Principles and Appropriateness
Use these scenario questions to test your grasp of modality principles and appropriateness. Write your answer before reading the discussion.
Scenario A: A 45-year-old male sheet-metal worker presents with left temporal headache and early morning visual blurring. Neurological examination is normal. The ophthalmologist asks for an MRI brain to exclude a space-occupying lesion. What safety step is mandatory before booking the MRI?
Discussion: Screen for ferromagnetic intra-ocular foreign bodies — an occupational hazard in metal workers. An orbital X-ray (two views) to exclude metallic fragments is mandatory before MRI in any patient with a history of metal-grinding, cutting, or welding. If metal is identified, MRI is contraindicated; CT head is the alternative.
Scenario B: A 22-year-old woman at 30 weeks of gestation is admitted after a fall at home. She has right-lower-quadrant tenderness and mild haematuria. The surgical registrar wants a CT abdomen-pelvis with contrast. What is the most defensible imaging sequence?
Discussion: Begin with ultrasound (FAST / detailed abdominal USG): it identifies free fluid, hepatic and splenic lacerations, and free intra-peritoneal fluid without fetal radiation. If USG is inconclusive and haemodynamic instability demands a definitive answer, maternal life takes priority and CT is justified with appropriate fetal shielding and the lowest feasible dose. MRI abdomen is an ionising-free alternative if time and resources permit and the patient is stable.
Scenario C: A 70-year-old man with known prostate cancer presents with back pain. His PSA has risen. Bone scintigraphy is ordered. Why is this the appropriate modality rather than plain X-ray or CT?
Discussion: Bone scintigraphy uses a technetium-99m labelled diphosphonate (e.g., ^99mTc-MDP) that accumulates at sites of increased osteoblastic activity — a metabolic signal that precedes structural bone destruction visible on plain X-ray (bone scan is positive earlier). CT shows bony destruction but lacks whole-body functional sensitivity for metastasis. PET-CT (^18F-NaF or PSMA PET) has even higher sensitivity but scintigraphy remains widely available and cost-effective for initial skeletal survey.