Page 2 of 17
RD5.1 | Normal X-ray Anatomy in Adults, Neonates and Children — SDL Guide (Part 2)
Interpreting the Normal Neonatal and Paediatric Film — Thymus, Epiphyses and Growth Plates
Paediatric radiographs carry two normal appearances that are so commonly misread as pathology that the competency names them explicitly, and recognising them is a defined interpretation skill in its own right. The first is the normal thymus. In neonates and infants the thymus is large relative to the chest and is a normal mediastinal soft-tissue structure. On the frontal chest film it classically produces the thymic 'sail sign' — a triangular density projecting from the (usually right) mediastinal border like a sail — and the 'thymic wave sign', a gently undulating lateral margin caused by the overlying ribs. The key discriminators that mark it as the normal thymus rather than a mass or consolidation are: it has a sharp, often wavy border; it does not contain air bronchograms; it does not displace the trachea or other structures; it merges smoothly with the cardiac silhouette; and it changes shape with respiration and may shrink with stress or steroids. A confident reader who recognises these features avoids the unnecessary CT that the hook's resident triggered.
The second is the normal paediatric joint. A child's long bone has distinct regions — the diaphysis (shaft), the metaphysis (flared end), the radiolucent physis (the growth plate, made of cartilage), and the epiphysis (the secondary ossification centre beyond the physis). Because cartilage is radiolucent, the physis appears as a clean lucent LINE between the metaphysis and the ossified epiphysis — and this is exactly why it is mistaken for a fracture by the unwary. The discriminating features are: a growth plate is at the EXPECTED anatomical site, has smooth well-corticated (sclerotic) margins on both sides, and is symmetrical with the opposite limb; a fracture line is irregular, may not be at a physeal site, lacks corticated margins, and is usually accompanied by soft-tissue swelling and sometimes a step in the cortex. Comparison with a film of the contralateral normal limb is the single most useful tool when in doubt. Ossification centres also appear and fuse at PREDICTABLE ages, which is the normal-standard basis that the next SDL uses for age estimation.
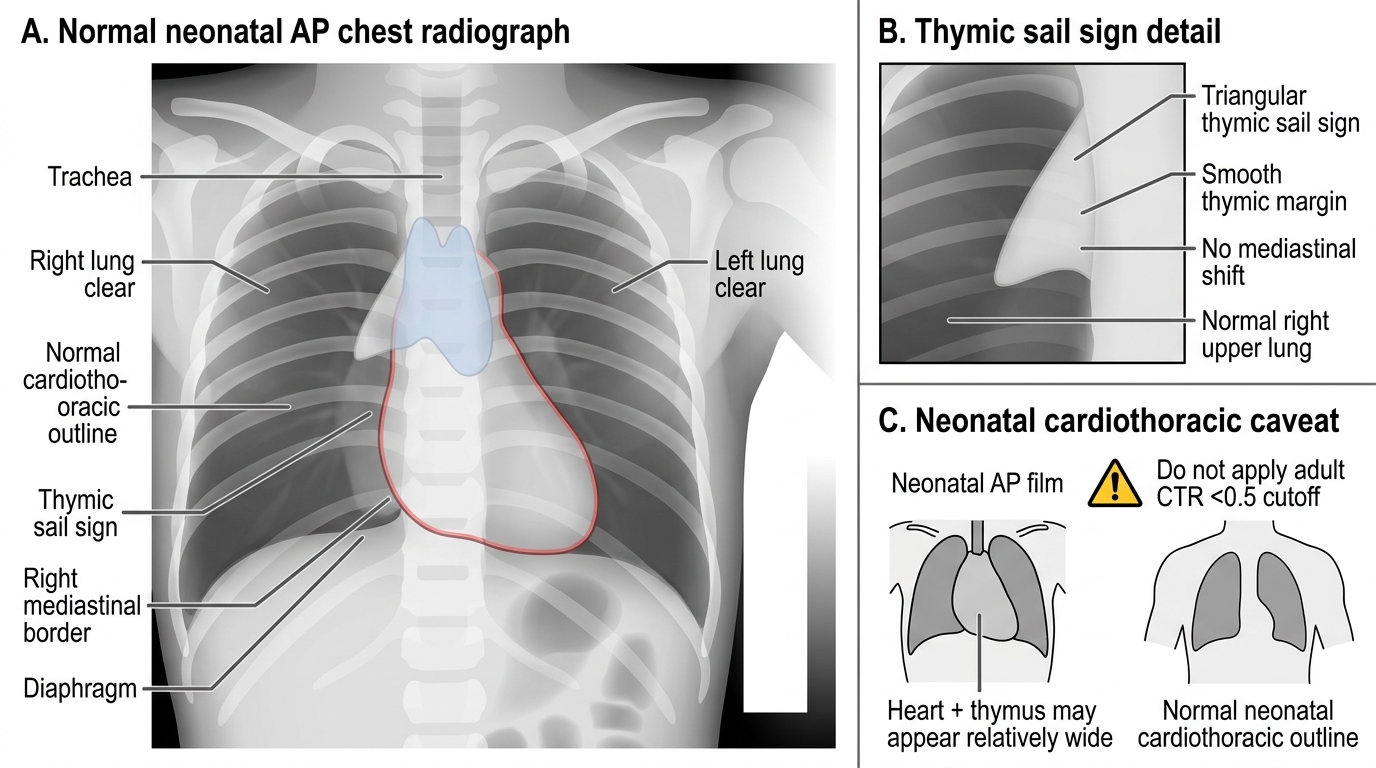
Normal Neonatal Chest Radiograph with Thymic Sail Sign
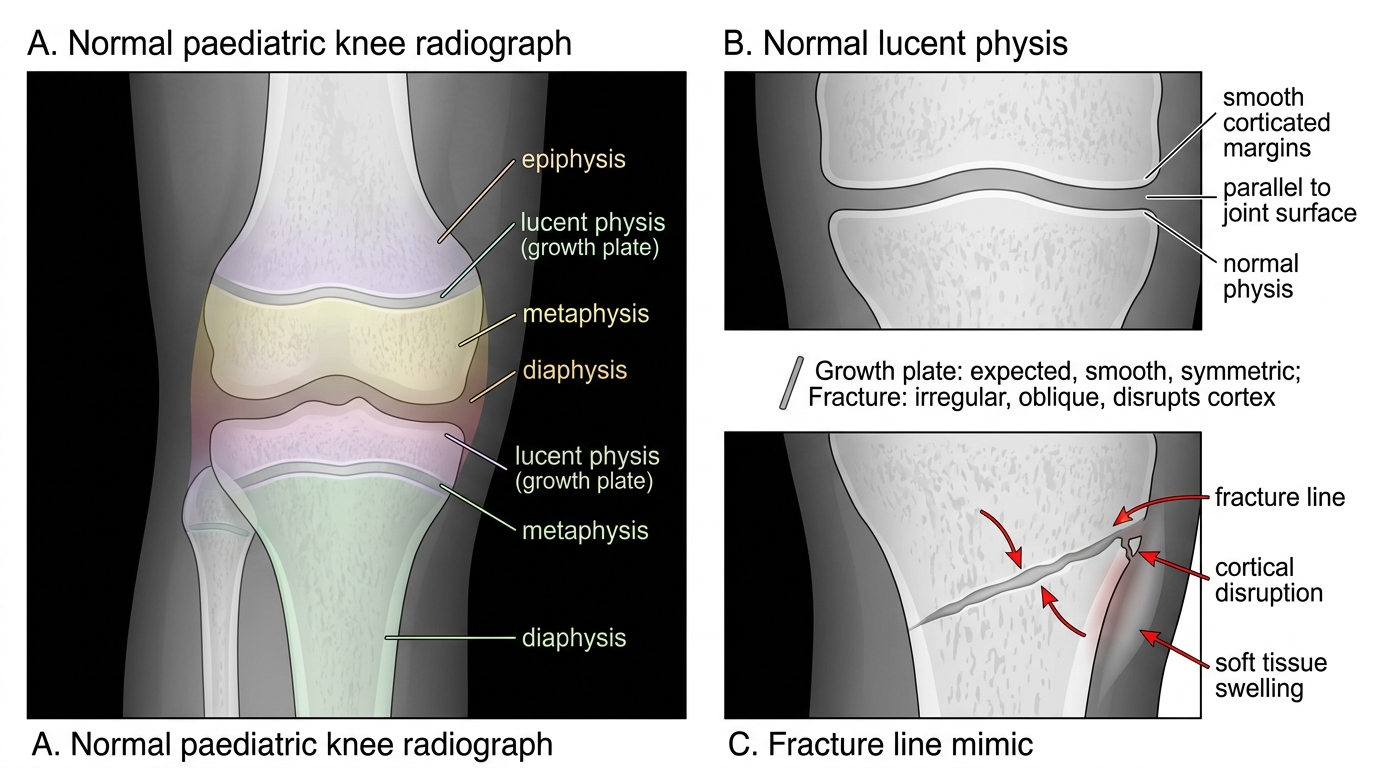
Normal Paediatric Knee: Growth Plate Versus Fracture Line
A final paediatric caveat: the infant cardiothoracic ratio is normally larger than the adult <0.5 figure (the neonatal heart and thymus together occupy a relatively wider mediastinum), and AP technique is the norm in this age group — so the adult cardiothoracic cut-off must not be transplanted onto a neonatal film.
Applied Practice — Reading and Reporting a Set of Normal Studies
Applied practice means walking the systematic read end to end and producing a clear normal report, because a structured normal report is itself a clinical skill that documents that every zone was examined. Work through these as if reporting at the viewing console. For a normal adult PA chest: 'PA erect chest radiograph, adequate inspiration and no rotation. Trachea central. Mediastinum and hila normal. Lungs clear with no focal opacity, effusion or pneumothorax. Heart size normal, cardiothoracic ratio less than 0.5. Both hemidiaphragms and costophrenic angles are clear. Visualised bones and soft tissues are unremarkable. Conclusion: normal chest radiograph.' Notice that the report mirrors the search pattern — naming each zone is the evidence that it was checked.
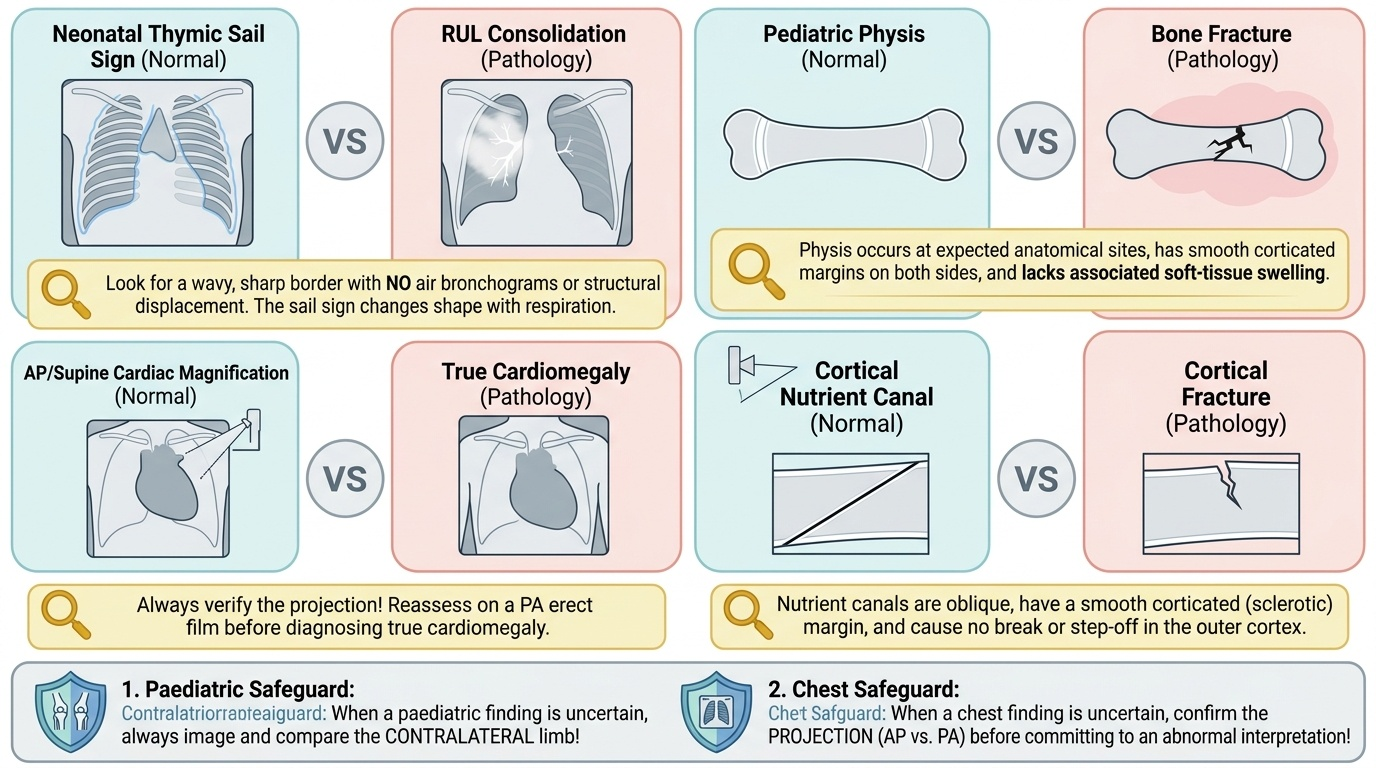
The value of applied practice is in pre-empting the recurring false-positive traps. The table below pairs each normal feature with the pathology it is most often mistaken for and the discriminating rule:
Provided image
| Normal feature | Mistaken for | Discriminating rule |
|---|---|---|
| Neonatal thymic sail sign | Mediastinal mass / RUL consolidation | Wavy sharp border, no air bronchograms, no structure displacement, changes with respiration |
| Paediatric physis (growth plate) | Fracture | Expected site, smooth corticated margins both sides, symmetrical with other limb, no soft-tissue swelling |
| AP/supine cardiac magnification | Cardiomegaly | Projection note — reassess on a PA erect film before diagnosing |
| Cortical nutrient canal | Cortical fracture | Oblique lucency with a corticated (sclerotic) margin, no break in cortex, constant site |
| Ossification centre (e.g. elbow) | Avulsion fragment | Appears at predicted age, smooth margin, symmetrical with contralateral limb |
The two governing safeguards across all of these are: (1) when a paediatric finding is uncertain, image and compare the CONTRALATERAL limb; and (2) when a chest finding is uncertain, confirm the PROJECTION before committing to an abnormal interpretation.
SELF-CHECK
A 5-year-old falls and injures the knee. The radiograph shows a lucent line running transversely across the distal femur between the ossified shaft-end and a separate ossified segment at the joint end. The margins of the lucent line are smooth and corticated, there is no soft-tissue swelling, and the appearance is symmetrical with the other knee. What does this most likely represent?
A. A Salter-Harris type I fracture through the growth plate
B. The normal physis (growth plate), a radiolucent cartilage line between metaphysis and epiphysis
C. Osteomyelitis of the distal femur
D. An avulsion fracture of the epiphysis
Reveal Answer
Answer: B. The normal physis (growth plate), a radiolucent cartilage line between metaphysis and epiphysis
A normal growth plate (physis) is a radiolucent cartilage line lying between the metaphysis and the epiphysis. Features that mark it as normal rather than a fracture are: it is at the expected anatomical site, has smooth corticated margins on both sides, is symmetrical with the contralateral limb, and is not accompanied by soft-tissue swelling. A Salter-Harris fracture would typically show an irregular line, cortical disruption, asymmetry with the other side, or associated swelling. Comparison with the contralateral normal limb resolves most such uncertainties.
SELF-CHECK
A triangular soft-tissue density is seen at the right upper mediastinal border on the chest radiograph of a healthy 3-week-old infant. It has a wavy lateral margin, contains no air bronchograms, does not displace the trachea, and blends with the cardiac silhouette. What is the correct interpretation?
A. An anterior mediastinal mass requiring urgent CT
B. Right upper lobe consolidation
C. The normal thymus producing the 'sail sign' — a normal finding
D. A loculated pleural effusion
Reveal Answer
Answer: C. The normal thymus producing the 'sail sign' — a normal finding
This is the normal neonatal/infant thymus producing the classic 'sail sign'. The discriminating features of a normal thymus are: a sharp, often wavy ('thymic wave') border, absence of air bronchograms, no displacement of the trachea or other structures, blending with the cardiac silhouette, and variability with respiration. Recognising it avoids an unnecessary CT. A true mass would tend to displace structures; consolidation would show air bronchograms; an effusion would layer or loculate differently.
CLINICAL PEARL
Pearl 1 — Always confirm the projection before calling cardiomegaly. The cardiothoracic ratio <0.5 rule is valid only on a PA erect film. On any AP, supine or portable film the heart is magnified — never diagnose an enlarged heart from such a film without correlation.
Pearl 2 — The contralateral limb is the paediatric radiologist's best friend. When unsure whether a lucent line in a child is a growth plate or a fracture, an ossification centre or an avulsion, image and compare the OPPOSITE side. Growth plates and ossification centres are symmetrical; fractures are not.
Pearl 3 — 'Normal' is a diagnosis you must earn. Only call a film normal after a complete, fixed search pattern. 'Satisfaction of search' — stopping at the first reassuring or abnormal feature — is a leading cause of missed second findings. The structured normal report (naming each zone) is your proof that you looked everywhere.
Self-Assessment — Confirming the Normal Template
Use these scenarios to test whether your normal template and search discipline are secure. Decide your answer before reading the discussion, exactly as you would at the viewing console.
Scenario A: A medical officer at a peripheral centre reviews the chest film of a 1-month-old with mild tachypnoea and notes a 'widened upper mediastinum.' She is about to refer for CT to exclude a mass. What should she check first?
Discussion: In an infant a relatively wide upper mediastinum is most often the normal thymus. Before any referral she should look for the discriminating features of a normal thymus — a sharp/wavy border, no air bronchograms, no tracheal displacement, blending with the cardiac shadow — and remember that the neonatal cardiothoracic ratio is normally larger than the adult <0.5 figure and that the film is likely AP. If those normal features are present and the trachea is central and undisplaced, the appearance is the normal thymus and CT is not indicated.
Scenario B: A 7-year-old has a wrist injury. The AP film shows a lucent line across the distal radius. How do you decide whether this is the growth plate or a fracture?
Discussion: Apply the discriminators systematically. A normal physis lies at the expected metaphyseal–epiphyseal junction, has smooth corticated margins on both sides, is symmetrical with the other wrist, and has no associated soft-tissue swelling. A fracture line is irregular, may breach the cortex, is asymmetrical, and is usually accompanied by soft-tissue swelling. Obtain two orthogonal views and, if still uncertain, an image of the contralateral normal wrist for comparison.
Scenario C: A reporting checklist asks you to confirm a Water's view is technically adequate before reading the sinuses. What is the key technical landmark, and why does the normal appearance matter?
Discussion: In a correctly angled Water's (occipitomental) view the petrous ridges are projected BELOW the floor of the maxillary antra, clearing them so the maxillary sinuses can be assessed; the normal sinuses are symmetrically LUCENT (air-filled). Reading against this normal baseline, an opaque antrum or an air–fluid level then stands out as pathological. Without the normal template — symmetrical lucency, petrous ridges cleared — you cannot reliably call a sinus abnormal.