Page 1 of 17
RD7.3 | CT Brain in Stroke — SDL Guide
Learning Objectives
- Identify the clinical indications for emergency CT brain in a patient presenting with suspected stroke.
- Describe the imaging strategy for acute stroke including the rationale for non-contrast CT as the first-line investigation.
- Recognise the CT findings of haemorrhagic stroke and early ischaemic stroke, including the hyperdense MCA sign, loss of grey-white differentiation, and insular ribbon loss.
- Explain how the CT result gates the thrombolysis decision and the role of CT angiography in thrombectomy eligibility.
- State the time windows for IV alteplase and mechanical thrombectomy and understand how imaging findings influence eligibility.
INSTRUCTIONS
Acute stroke is a time-critical emergency where 'time is brain' — approximately 1.9 million neurons are lost for every minute of untreated large-vessel occlusion. The imaging decision made in the first minutes of a stroke call determines whether a patient receives thrombolysis, mechanical thrombectomy, or only supportive care. As a final-year student and future clinician, you will be part of the team that calls this imaging. This module equips you to understand what the CT brain is telling you, how to interpret its most important findings, and how those findings translate directly into treatment decisions.
References
- Sutton's Textbook of Radiology, 6th edition, Chapter on Neuroimaging (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter on Stroke Imaging (textbook)
- AHA/ASA 2019 Guidelines for the Early Management of Patients with Acute Ischaemic Stroke (guideline)
- Nogueira RG et al. DAWN Trial, NEJM 2018; Albers GW et al. DEFUSE 3 Trial, NEJM 2018 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 2 a.m. A 62-year-old right-handed man is brought to the emergency department with sudden-onset left-sided weakness and speech difficulty that began 90 minutes ago. He is hypertensive and diabetic. Neurology is on the way, but the casualty medical officer must decide: what is the first investigation? The answer is not 'wait for neurology' — it is a non-contrast CT brain, ordered immediately. The reason is not simply protocol: thrombolysis with IV alteplase could restore blood flow and save this man's functional independence, but only if haemorrhage has been excluded by CT. Giving alteplase to a haemorrhagic stroke is lethal. The CT report you generate (or the one you hand to a radiologist) in the next 20 minutes will determine whether this patient walks out of hospital or does not.
WHY THIS MATTERS
Stroke is the second leading cause of death and the leading cause of acquired disability worldwide. In India, the incidence of stroke is rising in tandem with hypertension, diabetes, and tobacco use. Thrombolysis with IV alteplase and mechanical thrombectomy for large-vessel occlusion are the only proven treatments that reverse ischaemic stroke — but both are time-locked and imaging-gated. The NMC competency RD7.3 requires you to understand the role of imaging in acute neurological presentations; this is not an abstract learning objective — it is the difference between recognising a treatable emergency and missing the treatment window. Every casualty posting, every night shift as a resident, and every ward call will include patients where this knowledge is active.
RECALL
Before reading further, recall:
- Stroke pathophysiology (from IM): ischaemic stroke arises from thrombotic or embolic occlusion of a cerebral artery; haemorrhagic stroke arises from rupture of a vessel (hypertensive, aneurysmal, or AVM). The ischaemic penumbra is the rim of dysfunctional but viable brain surrounding the infarct core — it is salvageable if flow is restored quickly.
- CT attenuation: fresh blood (haematoma) is hyperdense (bright white) on CT because haemoglobin is protein-rich and absorbs X-ray photons strongly (~50–70 HU). Brain parenchyma is ~30–40 HU. Air is ~−1000 HU. These Hounsfield unit (HU) values are the basis of CT interpretation.
- Grey-white differentiation: on CT, grey matter (cortex, deep nuclei) is slightly denser than white matter due to higher cellularity. Ischaemia causes cytotoxic oedema, which reduces the HU of grey matter toward white matter — causing the 'loss of grey-white differentiation' that is an early CT sign of infarction.
- MRI DWI: diffusion-weighted imaging detects restriction of water diffusion in acutely infarcted (ischaemic) tissue — it becomes bright on DWI and dark on ADC (apparent diffusion coefficient) map within minutes of ischaemia, before conventional MRI sequences are abnormal.
Clinical Scenario — The Stroke Call: Who Gets CT, When, and Why
The clinical indication for emergency CT brain in acute stroke is straightforward but absolute: every patient with a sudden-onset focal neurological deficit of potential vascular aetiology must have a non-contrast CT brain performed as soon as possible — and in most hospitals, 'as soon as possible' means within 25 minutes of arrival at the emergency department for a patient who is a potential thrombolysis candidate. This target is set by international and national stroke guidelines because the treatment benefit of thrombolysis decays with every minute of delay; a treatment given one hour earlier can mean the difference between a patient who walks and one who is wheelchair-dependent. The urgency is built into the investigation itself: CT brain in stroke is not a routine order but an emergency request that bypasses the normal queue.
The clinical scenarios that mandate immediate CT brain include:
- Acute ischaemic stroke (suspected): sudden hemiplegia, hemisensory loss, aphasia, hemianopia, ataxia, or altered consciousness of acute onset — the FAST signs (Face drooping, Arm weakness, Speech difficulty, Time to call emergency services).
- Haemorrhagic stroke: sudden severe headache (thunderclap — 'worst headache of life' suggesting subarachnoid haemorrhage), or sudden hemiplegia with hypertension (intracerebral haemorrhage until proven otherwise).
- Transient ischaemic attack (TIA): neurological deficit that has fully resolved — CT is still required because early DWI-MRI or CT perfusion may show the mechanism and high short-term recurrence risk demands prompt investigation.
The single most important principle governing the acute imaging decision is this: non-contrast CT (NCCT) must be performed BEFORE any anticoagulant, antiplatelet drug is given, and absolutely before thrombolysis is administered. The reason is simple — the clinical differentiation of haemorrhagic from ischaemic stroke by symptoms and signs alone is unreliable (both can present with hemiplegia and aphasia), and the treatment for each is diametrically opposite: thrombolysis saves ischaemic brain but is lethal in haemorrhagic stroke.
Imaging Strategy — Why Non-Contrast CT First, and What Else to Order
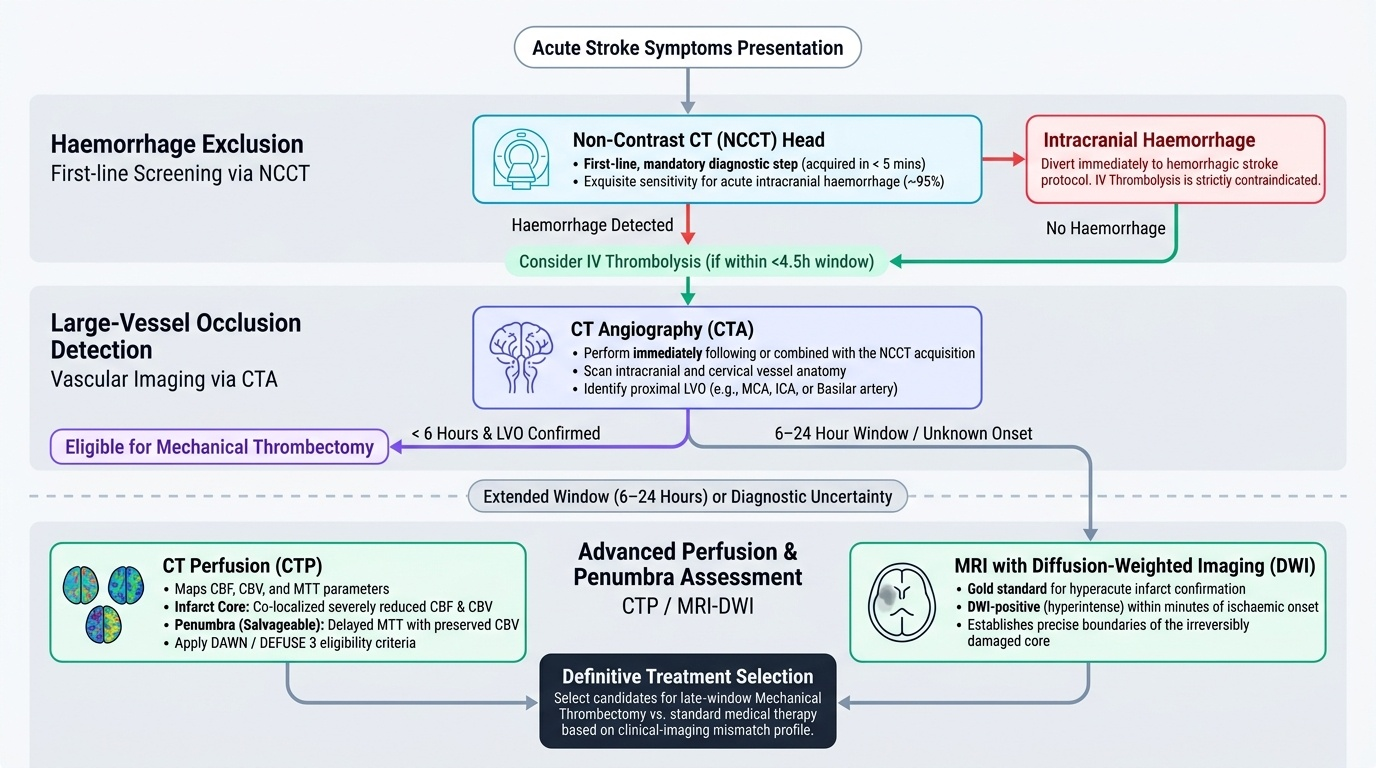
The imaging strategy for acute stroke follows a tiered logic: the first question (haemorrhage or not?) governs the immediate treatment decision, and subsequent questions (which vessel is occluded? is there salvageable brain?) govern the selection of definitive treatment. Understanding this hierarchy prevents both under-investigation (missing a treatable large-vessel occlusion) and over-investigation (obtaining advanced studies before the first critical question is answered).
Non-contrast CT (NCCT) head — first-line, mandatory:
NCCT is available in virtually every hospital with emergency facilities, takes less than 5 minutes to acquire, and is exquisitely sensitive for intracranial haemorrhage (sensitivity >95% for acute blood). It is also far faster than MRI. These two properties — speed and sensitivity for blood — make it the universal first-line investigation in acute stroke, regardless of how confident the clinician is in the ischaemic aetiology. Only after NCCT confirms the absence of haemorrhage can thrombolysis be considered.
CT angiography (CTA) — to identify large-vessel occlusion (LVO):
If NCCT shows no haemorrhage and the patient is within the treatment window, CTA of the intracranial and cervical vessels is performed immediately after (or combined in the same scanner run) to identify proximal vessel occlusion — typically middle cerebral artery (MCA), internal carotid artery (ICA), or basilar artery. LVO detection is essential for eligibility for mechanical thrombectomy, which is far more effective than thrombolysis for proximal occlusions.
CT perfusion (CTP) — to map ischaemic core vs penumbra:
CTP injects contrast and images the brain during first-pass perfusion, generating colour maps of cerebral blood flow (CBF), cerebral blood volume (CBV), and mean transit time (MTT). The infarct core (irreversibly damaged) is identified by severely reduced CBF and CBV; the penumbra (salvageable) shows delayed MTT but preserved CBV. CTP is used principally in the 6–24 hour extended window (DAWN/DEFUSE 3 criteria) to select patients who retain significant salvageable penumbra despite late presentation.
MRI with diffusion-weighted imaging (DWI) — most sensitive for early infarct:
DWI is positive (bright) within minutes of ischaemia onset and remains the gold standard for confirming early infarct. However, MRI takes 20–30 minutes or more, requires patient cooperation (no movement during acquisition), and is unavailable or delayed in many emergency settings. In the acute hyperacute window (<4.5 hours), MRI does not add information beyond NCCT for the thrombolysis decision; its superiority is in the subacute period (hours to days), in posterior-fossa stroke (CT has poor posterior fossa resolution due to beam-hardening artefact), and in young patients where TIA vs mimic is uncertain.
Provided image
SELF-CHECK
A 58-year-old man presents with sudden-onset right hemiplegia and global aphasia, onset 2 hours ago. He is haemodynamically stable. The emergency CT brain is ordered. Before receiving the report, the casualty team asks whether to start IV alteplase now. What is the correct response?
A. Proceed with alteplase immediately since onset is within 4.5 hours and the clinical picture is convincing
B. Wait for the NCCT brain report; alteplase is absolutely contraindicated if haemorrhage is present on CT
C. Order MRI-DWI first as it is more sensitive than CT for confirming ischaemia before giving thrombolysis
D. Give alteplase and arrange CT simultaneously to save time
Reveal Answer
Answer: B. Wait for the NCCT brain report; alteplase is absolutely contraindicated if haemorrhage is present on CT
Non-contrast CT must be obtained and confirmed to exclude haemorrhage BEFORE any thrombolysis. Giving alteplase in haemorrhagic stroke is lethal. The clinical picture cannot reliably distinguish haemorrhagic from ischaemic stroke. MRI-DWI is more sensitive for ischaemia but is slower and is not required before thrombolysis — NCCT to exclude haemorrhage is sufficient. Never give alteplase simultaneously with CT acquisition.
CT Findings in Stroke — Haemorrhage, Early Ischaemia and Time-Sensitive Signs
The ability to recognise the key CT appearances of both haemorrhagic and ischaemic stroke is a core interpretive skill for the final-year student. These findings must be identified in real time, often by a junior clinician overnight, and the management pathway pivots on them. The CT appearances of stroke fall into two clinically opposite categories: haemorrhagic (hyperdense, bright, blood is visible) and ischaemic (initially subtle, manifest as loss of normal grey-white contrast or arterial hyperdensity). Because these two categories have opposite treatment implications, the radiological distinction is not academic — it is the gate through which every acute stroke patient must pass before treatment is started. Understanding what the CT is showing, and why it appears as it does on the basis of Hounsfield unit physics, allows the clinician to reason through reports rather than simply accepting them as black-box outputs.
CT findings in haemorrhagic stroke:
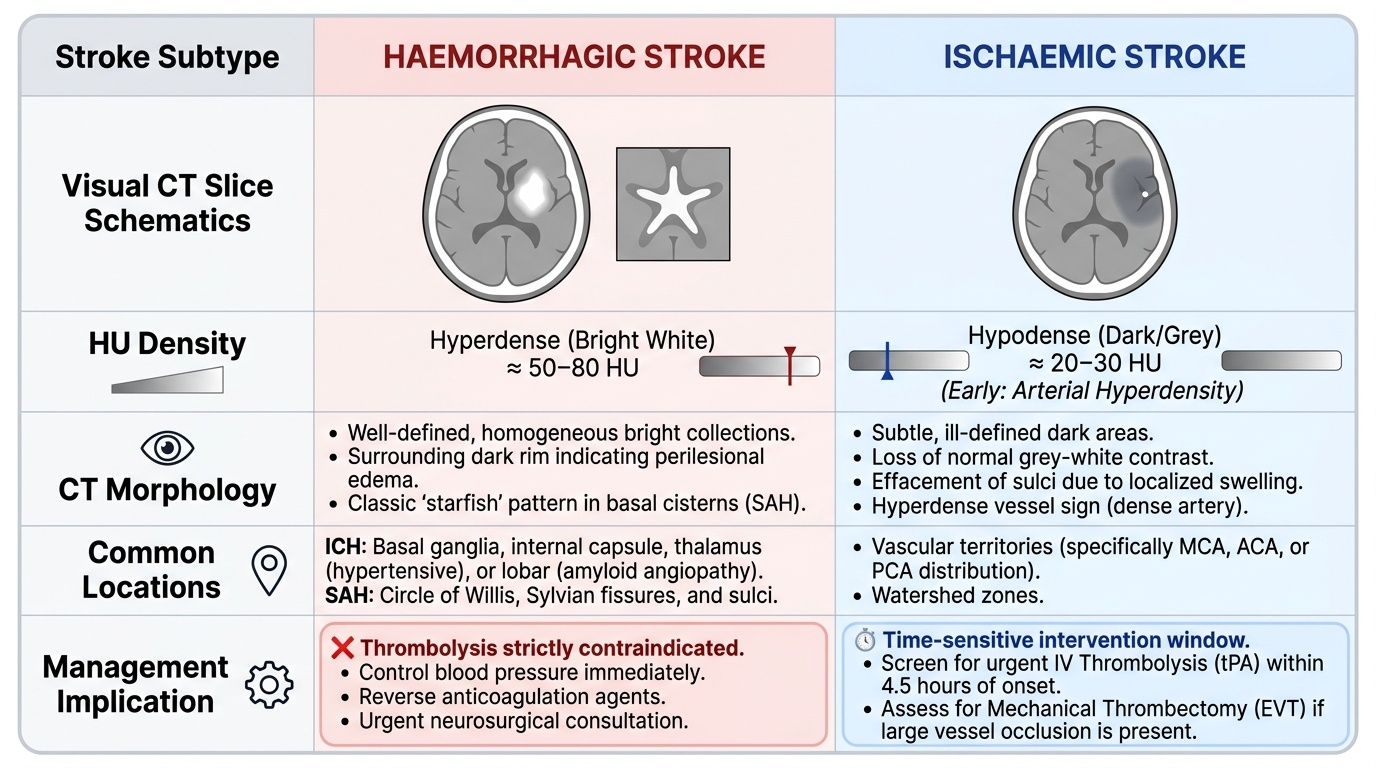
Fresh intracranial haemorrhage appears as a hyperdense (bright white, high HU ~50–80) collection on NCCT. The key appearances by location are:
- Intracerebral haemorrhage (ICH): well-defined hyperdense lesion within the brain parenchyma, classically in the basal ganglia/internal capsule (hypertensive haemorrhage) or the thalamus (hypertensive); or lobar (cortical/subcortical — consider amyloid angiopathy, underlying tumour or AVM in lobar ICH).
- Subarachnoid haemorrhage (SAH): hyperdense blood filling the basal cisterns (around the circle of Willis), Sylvian fissures, and sulci; 'starfish' appearance. CT is ~98% sensitive for SAH within 12 hours of onset but sensitivity drops thereafter — if CT is negative but SAH is strongly suspected, lumbar puncture for xanthochromia is mandatory.
- Subdural haematoma (SDH): crescentic hyperdense collection that crosses sutures and follows the inner contour of the skull; may be bilateral.
- Extradural haematoma (EDH): biconvex (lenticular) hyperdense collection, does NOT cross sutures, classically from middle meningeal artery tear at the pterion after temporal head trauma.
CT findings in ischaemic stroke — early (hyperacute) signs:
In the first 6 hours, CT may be normal — but experienced observers recognise subtle early signs that indicate irreversible infarction:
- Loss of grey-white differentiation: ischaemia causes cytotoxic oedema, reducing the HU of grey matter toward white-matter density; the cortical ribbon becomes indistinct, particularly in the insular cortex (insular ribbon sign), MCA territory cortex, and the deep grey matter (putamen, caudate).
- Hyperdense MCA sign: a thrombus in the proximal middle cerebral artery appears as a spontaneously hyperdense (bright) segment in the expected MCA location in the Sylvian fissure. Its presence predicts large-territory infarction and indicates LVO requiring thrombectomy assessment.
- ASPECTS (Alberta Stroke Program Early CT Score): a 10-point scoring system applied to two CT levels; 1 point is deducted for each of 10 defined MCA-territory regions showing early ischaemic change. ASPECTS ≤6 indicates established large-core infarct — these patients have a higher complication rate with reperfusion and may not be thrombectomy candidates on standard criteria.
Provided image
SELF-CHECK
On NCCT brain of a 70-year-old hypertensive woman with sudden right hemiplegia, you observe a well-defined hyperdense region (~65 HU) in the left putamen and internal capsule region. What is the most likely diagnosis and immediate management implication?
A. Ischaemic stroke; proceed with IV alteplase immediately
B. Hypertensive intracerebral haemorrhage; IV alteplase is contraindicated
C. Subarachnoid haemorrhage; arrange lumbar puncture to confirm
D. Normal variant; repeat CT in 24 hours to reassess
Reveal Answer
Answer: B. Hypertensive intracerebral haemorrhage; IV alteplase is contraindicated
A hyperdense lesion at ~65 HU in the putamen and internal capsule in a hypertensive patient is classic for hypertensive intracerebral haemorrhage (ICH). ICH is an absolute contraindication to thrombolysis — alteplase would expand the haematoma and is lethal. Management focuses on blood pressure control, reversal of anticoagulation if present, and neurosurgical evaluation for evacuation in selected cases. SAH appears as hyperdensity in the subarachnoid spaces (cisterns, sulci), not in the putamen.