Page 8 of 17
RD7.3 | Imaging Findings in Cardiac Failure — SDL Guide (Part 2)
Impact on Management — From Imaging to Treatment of Heart Failure
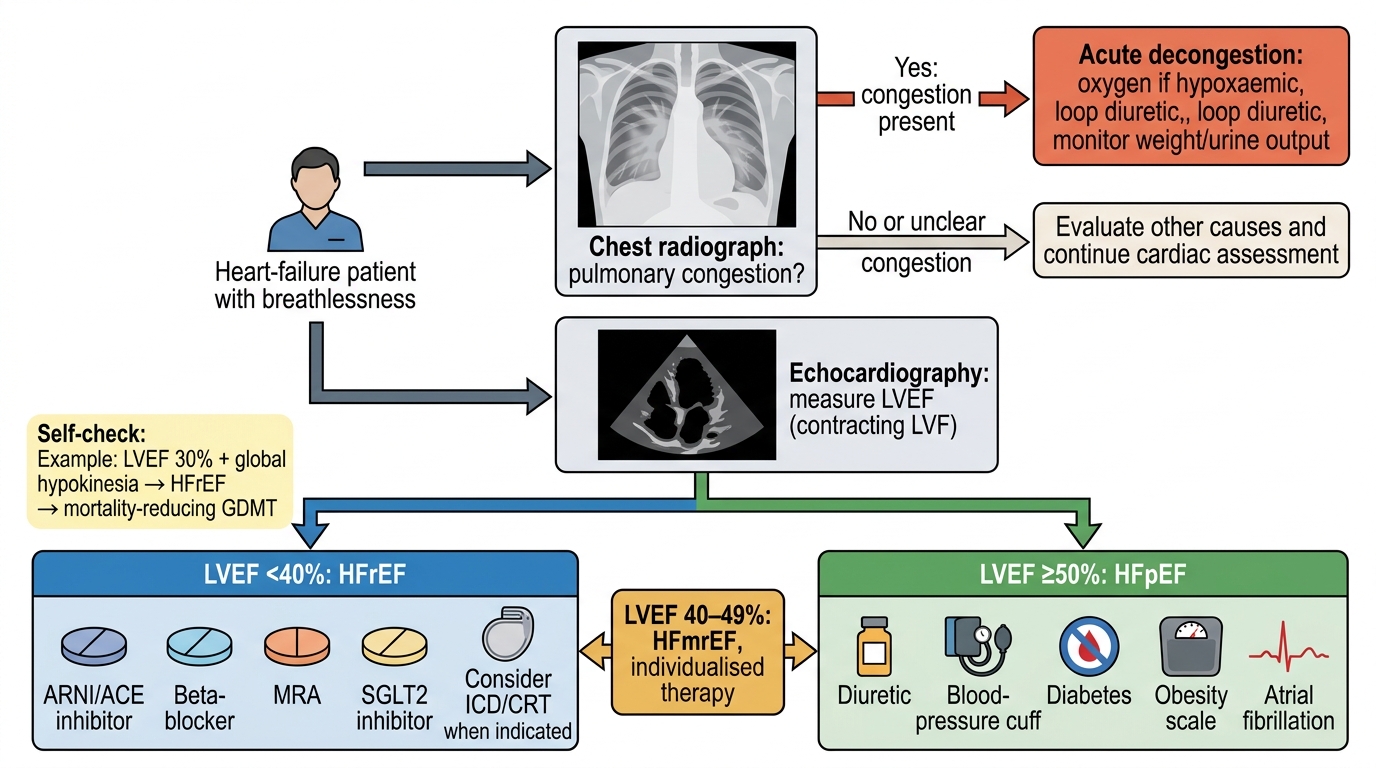
The imaging findings in heart failure are clinically powerful precisely because each one maps onto an immediate or long-term management decision, and integrating the radiographic and echocardiographic picture is what converts a diagnosis into a treatment plan. The chest radiograph drives the acute response to congestion, while the echocardiographic ejection fraction dictates the architecture of chronic, prognosis-modifying therapy. No element of heart-failure imaging is an end in itself: the cardiomegaly and oedema on the film, and the EF and structural findings on the echo, exist to be translated into diuresis, the correct guideline-directed drugs, device decisions and aetiology-specific treatment. Performing that translation — fusing the imaging with the clinical state to select therapy — is the core integrative skill that competency RD7.3 is assessing.
Acute congestion on the chest radiograph → decongestion:
When the radiograph shows alveolar oedema and the patient is congested, treatment begins immediately with loop diuretics, oxygen, sitting the patient up, and vasodilators (and ventilatory support such as CPAP) where appropriate. Serial radiographs or bedside lung ultrasound (clearing B-lines) help confirm that decongestion is occurring.
Ejection fraction on echocardiography → guideline-directed therapy:
The EF category determines the long-term drug strategy.
- HFrEF (LVEF <40%) has the strongest evidence base: the four foundational drug classes (an ARNI or ACE inhibitor, a beta-blocker, a mineralocorticoid-receptor antagonist, and an SGLT2 inhibitor) reduce mortality and admissions. A severely reduced EF also raises consideration of device therapy (ICD/CRT).
- HFpEF (LVEF ≥50%) is managed by treating congestion (diuretics), controlling blood pressure and comorbidities, with SGLT2 inhibitors now showing benefit. The echo here also looks for the diastolic dysfunction and elevated filling pressures that explain failure despite a normal EF.
Structural/aetiological findings → targeted treatment:
A regional wall-motion abnormality prompts evaluation for coronary disease and revascularisation; significant valvular disease prompts surgical or transcatheter intervention; cardiac MRI tissue characterisation (e.g. myocarditis, infiltration) guides aetiology-specific therapy.
Distinguishing cardiogenic from non-cardiogenic oedema:
Imaging helps separate cardiogenic pulmonary oedema (cardiomegaly, upper-lobe diversion, effusions, raised filling pressures on echo) from non-cardiogenic oedema/ARDS (normal heart size, more peripheral patchy opacities, normal EF) — a distinction that completely changes management.
Imaging-Based Pathway in Heart Failure
SELF-CHECK
A 65-year-old man with breathlessness has an echocardiogram showing a left-ventricular ejection fraction of 30% with global hypokinesia. How is his heart failure classified, and what is the main implication for management?
A. HFpEF; management is limited to diuretics and blood-pressure control
B. HFrEF; he is eligible for the four foundational mortality-reducing drug classes and possible device therapy
C. Non-cardiogenic pulmonary oedema; no cardiac medication is required
D. HFmrEF; no specific disease-modifying therapy is indicated
Reveal Answer
Answer: B. HFrEF; he is eligible for the four foundational mortality-reducing drug classes and possible device therapy
A left-ventricular ejection fraction of 30% defines heart failure with reduced ejection fraction (HFrEF, LVEF <40%). This category has the strongest evidence base for disease-modifying therapy: the four foundational drug classes (ARNI/ACE inhibitor, beta-blocker, mineralocorticoid-receptor antagonist, and SGLT2 inhibitor) reduce mortality and hospitalisation, and a severely reduced EF also raises consideration of device therapy (ICD/CRT). HFpEF (≥50%) is managed mainly by treating congestion and comorbidities, and the echo here clearly shows reduced — not preserved — function.
CLINICAL PEARL
Pearl 1 — Read the chest X-ray as a pressure gauge. The radiographic signs of heart failure appear in a predictable order as pulmonary venous pressure climbs: cardiomegaly and upper-lobe diversion first, then interstitial Kerley B lines and peribronchial cuffing, then alveolar (bat-wing) oedema and effusions. Naming where a patient sits on this cascade lets you estimate the severity of congestion from the film alone.
Pearl 2 — The ejection fraction is the fork in the road. Always anchor heart-failure management on the echocardiographic EF: HFrEF (<40%) unlocks the four foundational mortality-reducing drugs and device therapy, whereas HFpEF (≥50%) is treated by decongestion and comorbidity control. Without the EF you cannot choose the right therapy — which is why the echo is indispensable, not optional.
Pearl 3 — Cardiogenic versus non-cardiogenic oedema. When the lungs are 'white-out', use the heart size and distribution: cardiomegaly with upper-lobe diversion, effusions and a low EF points to cardiogenic oedema (diurese), whereas a normal-sized heart with peripheral patchy opacities and a normal EF points to ARDS/non-cardiogenic oedema (treat the underlying cause, not just diuresis).
Self-Assessment — Heart Failure Imaging Decisions
Work through these scenarios as if you are the clinician on call, deciding which imaging to obtain and how to act on it before reading each discussion. The aim is to rehearse the full integrative chain — clinical question, the right modality, the imaging finding, and the management decision it triggers — which is the precise competence that RD7.3 is testing in the internal-medicine setting. Pay attention to how the chest radiograph guides the acute response while the echocardiogram shapes the long-term plan, and to the situations where imaging changes the diagnosis entirely. Commit to a decision for each scenario before checking your reasoning against the discussion.
Scenario A: A 70-year-old man arrives in extremis with acute pulmonary oedema. His portable chest radiograph shows cardiomegaly, bilateral perihilar bat-wing opacification and small pleural effusions. What does the radiograph tell you, and what is your immediate action?
Discussion: The radiograph shows severe cardiogenic pulmonary oedema — cardiomegaly indicates an enlarged heart, and the bat-wing alveolar pattern with effusions indicates that pulmonary venous pressure has risen high enough to flood the alveoli. The immediate action is decongestion: sit the patient up, give oxygen and a loop diuretic, add vasodilators and consider CPAP. The radiograph does not give the ejection fraction, so an echocardiogram is arranged once he is stabilised to classify the failure and guide long-term therapy.
Scenario B: A 60-year-old hypertensive woman has exertional breathlessness. Her echocardiogram shows a left-ventricular ejection fraction of 58% but evidence of diastolic dysfunction and raised filling pressures. How is her heart failure classified, and how does this change management compared with a patient who has an EF of 25%?
Discussion: An EF of 58% with symptoms and signs of failure plus diastolic dysfunction is heart failure with preserved ejection fraction (HFpEF). Management focuses on treating congestion with diuretics, rigorous control of blood pressure and comorbidities, and an SGLT2 inhibitor; the four-pillar mortality-reducing regimen proven in HFrEF does not apply in the same way. A patient with an EF of 25% has HFrEF and is eligible for that full foundational regimen and possible device therapy — illustrating why measuring the EF is the decisive step.
Scenario C: A 45-year-old man with sepsis develops bilateral lung opacities. The chest radiograph shows widespread patchy peripheral opacities but a normal cardiothoracic ratio, and the echocardiogram shows a normal ejection fraction with normal filling pressures. Is this cardiogenic pulmonary oedema?
Discussion: No. A normal heart size, peripheral (rather than perihilar bat-wing) opacities, and a normal EF with normal filling pressures point away from cardiogenic oedema and toward non-cardiogenic oedema / acute respiratory distress syndrome (ARDS) in the context of sepsis. Recognising this prevents inappropriate aggressive diuresis and directs treatment toward the underlying cause and supportive ventilation — a distinction that imaging is central to making.