Page 11 of 17
RD7.3 | Imaging in Liver Parenchymal Disease — SDL Guide (Part 2)
Impact on Management — From Imaging to Decision in Liver Disease
The imaging findings in liver parenchymal disease are clinically decisive because each appearance directs a specific management response, and integrating the imaging with the clinical picture is what turns a description of the liver into a plan of care. A bright liver, a nodular cirrhotic liver, the signs of portal hypertension, and an arterially enhancing nodule each lead to a different pathway — from lifestyle modification, through structured surveillance and complication screening, to cancer staging and treatment. None of these findings is an end in itself: they exist to be translated into action, and performing that translation — fusing the imaging with the patient's history and bloods to choose the next step — is the integrative skill that competency RD7.3 is assessing in the internal-medicine setting.
Fatty liver (steatosis) → metabolic and lifestyle management:
A bright liver on ultrasound in a patient with metabolic risk factors prompts weight loss, control of diabetes and dyslipidaemia, reduction of alcohol, and assessment of fibrosis (often by elastography) to identify those at risk of progression. The imaging finding triggers risk-factor modification and stratifies the need for follow-up.
Cirrhosis → surveillance and complication screening:
Ultrasound evidence of cirrhosis commits the patient to a structured programme: 6-monthly ultrasound (± AFP) surveillance for hepatocellular carcinoma, endoscopic screening for oesophageal varices, and monitoring for decompensation (ascites, encephalopathy, jaundice). The imaging diagnosis of cirrhosis is therefore a gateway to a whole care pathway.
Portal hypertension findings → targeted intervention:
Imaging signs of portal hypertension (splenomegaly, ascites, collaterals, reversed portal flow) prompt upper GI endoscopy to look for and treat varices (banding, prophylaxis), management of ascites, and consideration of interventional procedures (such as TIPS) in selected patients. The findings change both the urgency and the type of intervention.
Hepatocellular carcinoma → staging and treatment:
A nodule with the characteristic arterial hyperenhancement and washout on multiphasic imaging establishes the diagnosis of HCC in the cirrhotic patient (often without biopsy) and triggers staging and a stage-appropriate treatment decision — resection, ablation, transplantation, transarterial therapy or systemic therapy. Early detection through surveillance is what makes curative treatment possible.
Contrast-safety as part of the decision:
The choice of cross-sectional modality must respect renal function: iodinated contrast (CT) is generally avoided when the eGFR is below 30, and gadolinium (MRI) is used cautiously in severe renal impairment — a safety consideration that directly shapes which definitive test is chosen.
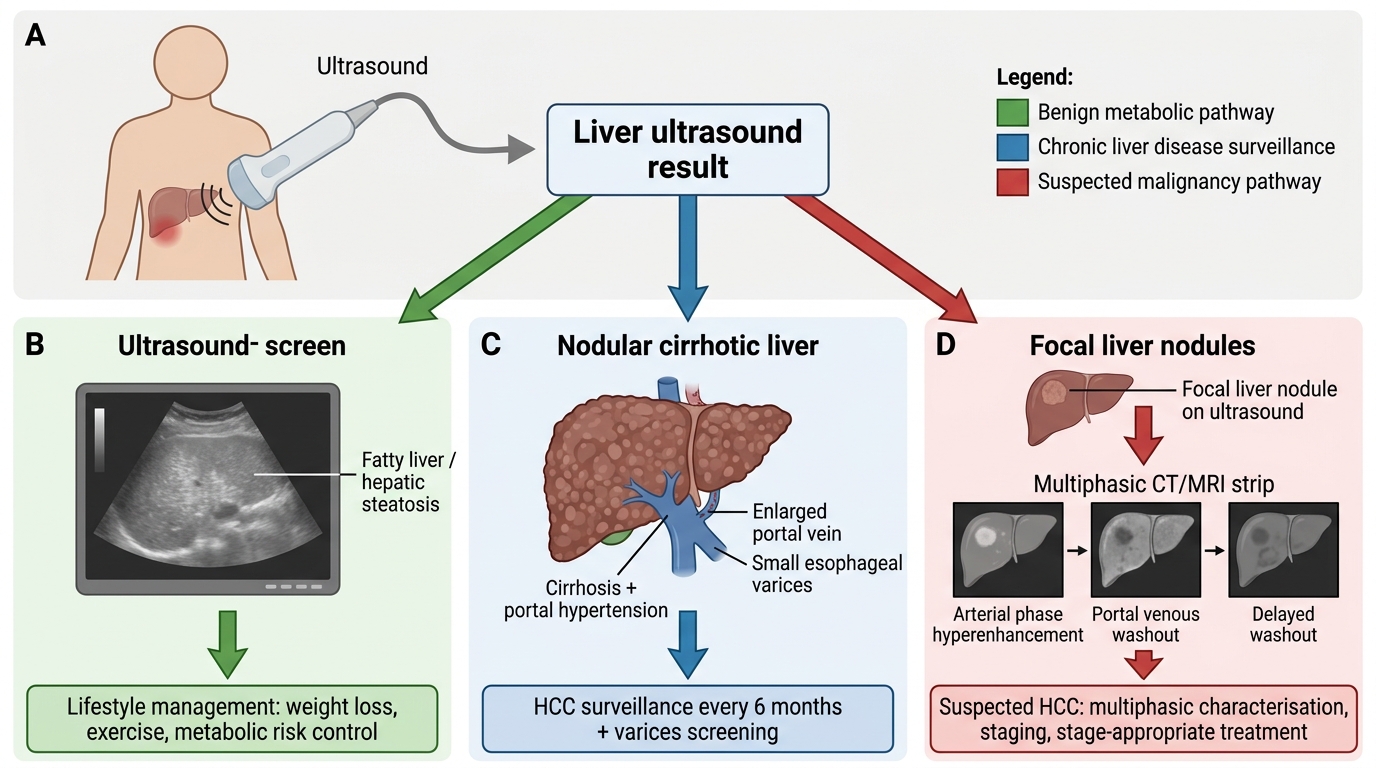
Liver Ultrasound Decision Pathway
SELF-CHECK
A patient with known cirrhosis on 6-monthly surveillance has a 3 cm liver nodule. Multiphasic CT shows the nodule enhancing avidly in the arterial phase with washout in the portal-venous and delayed phases. What does this imaging pattern indicate and what is the management implication?
A. A simple haemangioma; no further action is needed
B. Hepatocellular carcinoma; the arterial hyperenhancement with washout is diagnostic in a cirrhotic liver and triggers staging and stage-appropriate treatment
C. Fatty infiltration; advise lifestyle modification only
D. A regenerative nodule; continue routine 6-monthly surveillance with no change
Reveal Answer
Answer: B. Hepatocellular carcinoma; the arterial hyperenhancement with washout is diagnostic in a cirrhotic liver and triggers staging and stage-appropriate treatment
Arterial-phase hyperenhancement followed by washout in the portal-venous/delayed phases on multiphasic imaging is the hallmark of hepatocellular carcinoma (HCC) and, in the setting of cirrhosis, is diagnostic without the need for biopsy (the basis of the LI-RADS criteria). This finding triggers staging and a stage-appropriate treatment decision — resection, ablation, transplantation, transarterial therapy or systemic therapy — and is precisely the curable-stage cancer that 6-monthly surveillance aims to catch. A haemangioma shows peripheral nodular discontinuous enhancement with progressive fill-in, not washout, and fatty infiltration is diffuse, not a focal enhancing mass.
CLINICAL PEARL
Pearl 1 — Compare the liver with the kidney. The quickest ultrasound sign of fatty liver is loss of the normal hepatorenal echo contrast — the liver becomes brighter than the adjacent right renal cortex. Train your eye to make this side-by-side comparison; it is the single most useful 'bright liver' check.
Pearl 2 — A diagnosis of cirrhosis is a commitment to surveillance. Whenever imaging shows cirrhosis, the patient must enter a structured pathway: 6-monthly ultrasound (± AFP) for hepatocellular carcinoma and endoscopic screening for varices. Surveillance is what converts an incurable late cancer into a curable early one — never let a cirrhotic patient drift out of the programme.
Pearl 3 — Arterial hyperenhancement with washout = HCC. In a cirrhotic liver, a nodule that lights up in the arterial phase and then washes out on the delayed phase is hepatocellular carcinoma and can be diagnosed on imaging alone in the right setting. Recognising this dual-blood-supply behaviour on multiphasic CT/MRI is high-yield and clinically decisive.
Self-Assessment — Liver Imaging Decisions
Work through these scenarios as if you are the clinician in the internal-medicine clinic, deciding which imaging to request and how to act on the result before reading each discussion. The purpose is to rehearse the integrative chain — clinical trigger, first-line modality, the imaging finding, and the management decision it sets in motion — which is exactly the competence that RD7.3 is testing for hepatobiliary disease. Notice how ultrasound is almost always the starting point, how its findings determine whether you escalate to elastography or multiphasic imaging, and how a diagnosis of cirrhosis commits the patient to a surveillance pathway. Commit to a plan for each scenario before checking your reasoning against the discussion.
Scenario A: A 50-year-old obese man with type 2 diabetes has mildly raised transaminases. His ultrasound shows a bright liver with loss of hepatorenal contrast. What is the diagnosis, and what is the next step?
Discussion: The ultrasound shows fatty liver (hepatic steatosis). The diagnosis triggers metabolic management — weight loss, glycaemic and lipid control, and reduction of alcohol — and an assessment of fibrosis, commonly with transient elastography, to identify whether he is progressing toward cirrhosis. The bright liver is not a reason for reassurance alone; it is a trigger for risk-factor modification and fibrosis stratification.
Scenario B: A 60-year-old woman with chronic hepatitis-related cirrhosis attends for surveillance. Her ultrasound shows a new 2.5 cm nodule that was not present 6 months ago. What is the appropriate next imaging step and why?
Discussion: Any new nodule in a cirrhotic liver requires characterisation, because it may be hepatocellular carcinoma. The appropriate next step is multiphasic contrast CT or MRI to look for the characteristic arterial-phase hyperenhancement with portal-venous/delayed washout. If that pattern is present in a cirrhotic liver, HCC can be diagnosed on imaging alone and the patient proceeds to staging and treatment. This is exactly the situation that 6-monthly surveillance is designed to detect early.
Scenario C: A 55-year-old man with cirrhosis presents with new abdominal distension. Ultrasound shows ascites, splenomegaly, a dilated portal vein and a recanalised paraumbilical vein. What do these findings indicate, and what management do they prompt?
Discussion: These are the imaging signs of portal hypertension — ascites, splenomegaly, portal vein dilatation, and a portosystemic collateral (the recanalised paraumbilical vein). They prompt management of the ascites and, importantly, upper GI endoscopy to screen for and treat oesophageal varices before they bleed, together with consideration of further intervention (such as TIPS) in selected patients. The imaging directly changes both the urgency and the type of treatment.