Page 11 of 17
RD7.6 | Breast Cancer Screening and Imaging in Management — SDL Guide (Part 2)
Impact on Diagnosis and Management — From BI-RADS to Biopsy, Staging and Treatment Planning
The clinical value of breast imaging lies in how its findings, expressed as a BI-RADS category and read within the triple assessment, drive the management pathway — from reassurance, to follow-up, to biopsy, to staging and treatment. Integrating these findings into the patient's plan is precisely what competency RD7.6 asks of the final-year student: the learner takes the provided imaging findings and the description of appearances and folds them into the screening and management decisions, rather than performing or reporting the studies. The discipline is to translate each category into its action, to insist on triple-assessment concordance, and to recognise where imaging continues to contribute through staging and follow-up. The pathway below shows how the imaging report becomes care.
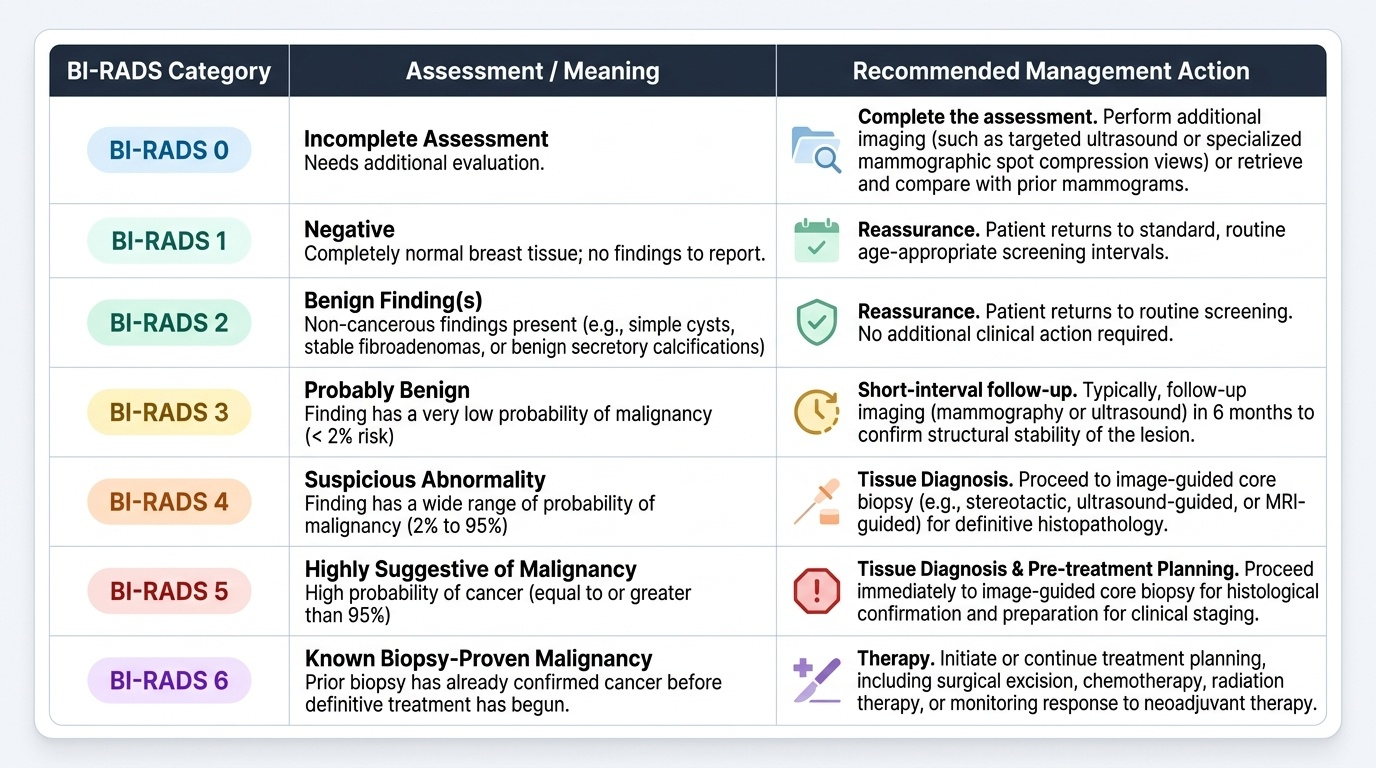
BI-RADS category to action (the core of integration):
- BI-RADS 1-2 (normal/benign): reassurance and return to routine screening.
- BI-RADS 3 (probably benign): short-interval (typically 6-month) follow-up imaging to confirm stability.
- BI-RADS 4-5 (suspicious / highly suggestive): proceed to image-guided core biopsy for tissue diagnosis.
- BI-RADS 0: complete the assessment with additional imaging before categorising.
Triple assessment and concordance:
The diagnosis of a breast lump rests on the concordance of clinical examination, imaging and pathology. When all three agree, the diagnosis is reliable; when they are discordant (e.g. a clinically suspicious lump with benign imaging or benign cytology), the lesion is investigated further — never dismissed. This is the safeguard against missing a cancer that one modality failed to detect, and it is the reason a normal mammogram alone cannot exclude cancer in a symptomatic woman.
Staging once cancer is confirmed (imaging's continuing role):
- Local-regional extent: mammography and ultrasound (and MRI in selected cases) define tumour size, multifocality and axillary nodal involvement; ultrasound-guided sampling of suspicious nodes informs surgical planning.
- Distant staging: in higher-stage or symptomatic disease, CT (chest/abdomen/pelvis), bone scan and/or PET-CT look for distant metastases (lung, liver, bone). These detect spread; they do not detect the primary.
- MRI further clarifies disease extent, the contralateral breast, and response to neoadjuvant chemotherapy.
Imaging in ongoing management: image-guided localisation assists breast-conserving surgery; surveillance imaging monitors for recurrence; and MRI assesses response during neoadjuvant treatment. Throughout, imaging informs a multidisciplinary treatment plan (surgery, radiotherapy, systemic therapy) rather than dictating it alone.
Provided image
SELF-CHECK
A 48-year-old woman has a clinically firm, irregular breast lump. Her mammogram is reported as BI-RADS 2 (benign-appearing). How should this discordance between a suspicious clinical finding and benign imaging be handled?
A. Reassure and discharge, because the mammogram is benign and mammography is the most sensitive test
B. Recognise the discordance and pursue further assessment (ultrasound and/or image-guided biopsy) — a benign mammogram does not exclude cancer in a clinically suspicious lump
C. Repeat the mammogram in 3 years at the next screening round
D. Start chemotherapy empirically without a tissue diagnosis
Reveal Answer
Answer: B. Recognise the discordance and pursue further assessment (ultrasound and/or image-guided biopsy) — a benign mammogram does not exclude cancer in a clinically suspicious lump
This is a discordant triple assessment: the clinical finding is suspicious but the imaging is benign. The rule is that discordance is always investigated, never dismissed — a normal or benign mammogram does NOT exclude cancer in a woman with a clinically suspicious lump (mammographic sensitivity is imperfect, especially in dense breasts). The correct step is further assessment with ultrasound and, as indicated, image-guided core biopsy to obtain a tissue diagnosis. Discharging her would risk missing a cancer; empiric chemotherapy without histology is never appropriate.
CLINICAL PEARL
Pearl 1 — Mammography screens; ultrasound characterises and is first-line in the young and dense breast. Use mammography for asymptomatic screening and older breasts; choose ultrasound first for a lump in a woman under about 40, in dense breasts, and in pregnancy/lactation (no ionising radiation). MRI is for high-risk screening (e.g. BRCA carriers) and staging, not routine screening.
Pearl 2 — BI-RADS is a management instruction, not just a description. Learn the actions: 1-2 routine/reassure; 3 short-interval follow-up; 4-5 biopsy; 0 needs more imaging; 6 known cancer. Translating the category into the next step is the examinable skill.
Pearl 3 — Respect triple-assessment concordance. A benign mammogram does NOT exclude cancer in a clinically suspicious lump. When clinical, imaging and pathology disagree, investigate further — discordance is pursued, never dismissed.
Self-Assessment — Imaging Decisions in Breast Screening and Management
Work through these scenarios as the clinician in the breast clinic. For each, decide on the imaging modality, interpret the findings or BI-RADS category, and determine the next step before reading the discussion. Integrating the imaging into screening and management decisions is exactly the applied competence RD7.6 sets for you.
Scenario A: A healthy, asymptomatic 53-year-old woman attends for routine breast screening. What is the screening test, what is its principal aim, and what early sign of cancer is it especially good at detecting?
Discussion: The screening test is mammography. Its aim is to detect small, impalpable breast cancers before they become symptomatic, thereby reducing breast-cancer mortality through earlier treatment. Mammography is particularly good at detecting microcalcifications, which may be the earliest sign of an in-situ or small invasive cancer. The benefits of screening are weighed against recognised harms (false positives, overdiagnosis), which is why programmes target defined age ranges.
Scenario B: A 26-year-old woman who is 20 weeks pregnant finds a breast lump. Which imaging modality is most appropriate, and why is mammography not the first choice here?
Discussion: Ultrasound is the appropriate first imaging modality. It uses no ionising radiation — important in pregnancy — and reliably characterises the lump as solid or cystic, while the dense, hormonally stimulated breast of a young pregnant woman further reduces mammographic sensitivity. If imaging or biopsy raises concern for malignancy, mammography can be performed with abdominal shielding, but ultrasound (plus triple assessment with core biopsy if needed) leads. A breast lump in pregnancy must still be fully assessed and not attributed to pregnancy changes.
Scenario C: A 40-year-old woman with a known BRCA1 mutation and a strong family history of breast cancer is being enrolled in a high-risk screening programme. Which modality is recommended for her screening in addition to mammography, and why?
Discussion: Breast MRI is recommended for screening high-risk women such as BRCA1/BRCA2 carriers, usually alongside mammography, because MRI is more sensitive than mammography for detecting cancer in this group (who often have dense breasts and earlier-onset disease). MRI uses no ionising radiation but does use gadolinium contrast, and its lower specificity means more false positives — accepted in exchange for higher sensitivity in a high-risk population where missing a cancer is especially costly.