Page 2 of 17
RD7.1 | Imaging in PCOD — SDL Guide (Part 2)
Impact on Diagnosis and Management — Integrating the Scan into Patient Care
The value of the ultrasound in PCOD lies in how it is integrated into the whole clinical picture, not in the image itself. Once you have an ultrasound report, the task is to place it correctly within the Rotterdam framework, to use it to exclude mimics, and to let it inform — but never dictate — management. This integration is precisely what competency RD7.1 asks of the final-year student: the learner takes the provided imaging findings and the description of appearances and folds them into the diagnosis and management of the patient, rather than performing or formally reporting the scan. The discipline is to ask, at every step, what the scan adds to the decision in front of you.
Integrating the scan into the diagnosis:
- If the patient already has both oligo/anovulation AND hyperandrogenism, she meets Rotterdam with two criteria; the ultrasound is confirmatory and not strictly required for diagnosis.
- If she has only one clinical/biochemical feature, a scan showing PCOM provides the second criterion and completes the diagnosis — provided mimics have been excluded.
- If the scan shows PCOM but there are no clinical or biochemical features, this is an incidental polycystic-appearing ovary and does NOT constitute PCOS.
Using imaging to exclude mimics and complications:
- Marked or rapidly progressive virilisation, or a very high testosterone, should prompt imaging (pelvic ultrasound and, if needed, MRI or adrenal CT) to exclude an androgen-secreting ovarian or adrenal tumour — a different and more urgent diagnosis.
- In women with prolonged amenorrhoea and unopposed oestrogen, transvaginal ultrasound also assesses endometrial thickness; a thickened endometrium raises concern for endometrial hyperplasia and warrants further evaluation, an important long-term risk in PCOS.
Informing management (imaging supports, does not drive):
- The cornerstone of management is lifestyle modification (weight reduction, exercise) for the metabolic dimension, regardless of the scan.
- Cycle regulation with combined oral contraceptives addresses menstrual irregularity and hyperandrogenism.
- For subfertility, ovulation induction (e.g. letrozole as first-line) is monitored with follicular-tracking ultrasound — here imaging has an active, ongoing role in counting and sizing the developing dominant follicle and timing intercourse or trigger.
The imaging finding, then, is supportive evidence at diagnosis and an active monitoring tool during fertility treatment, but the management of PCOD is fundamentally clinical and metabolic.
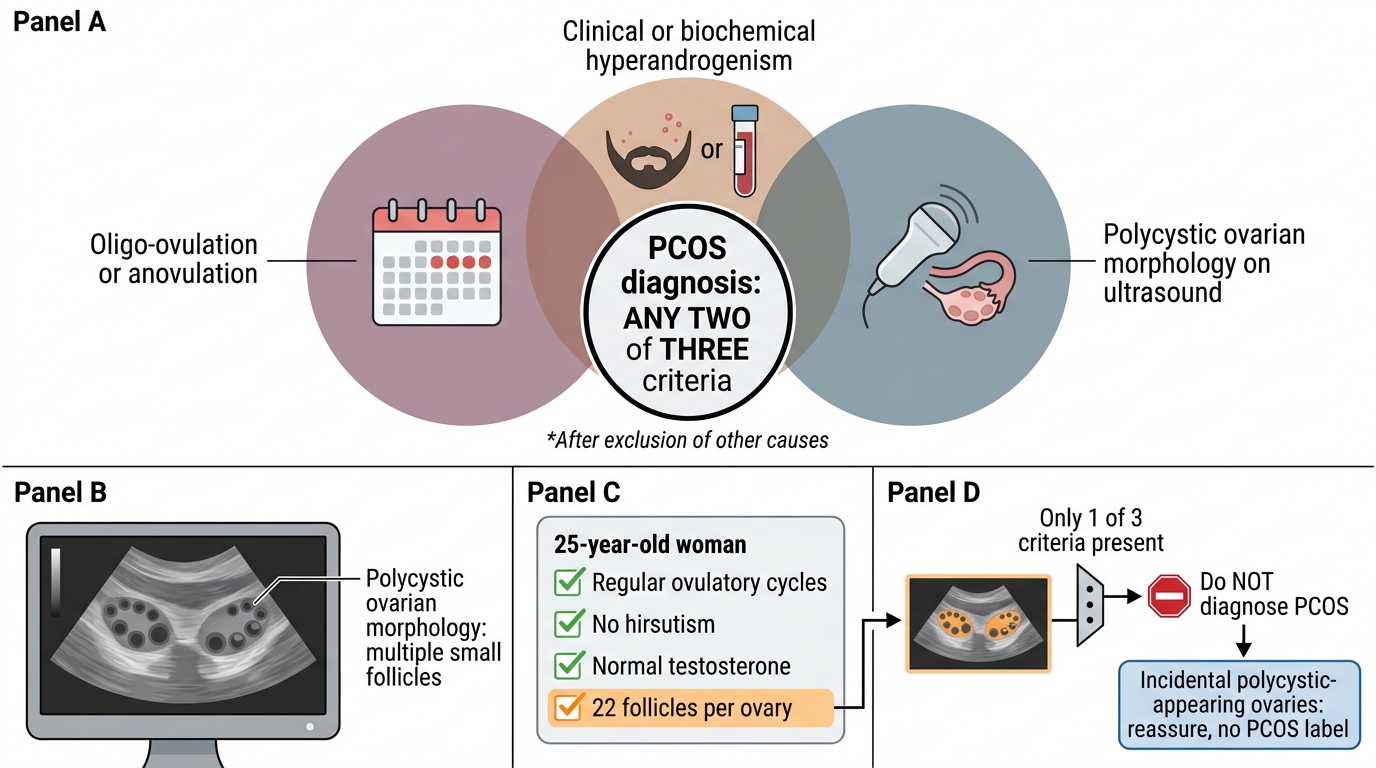
Rotterdam Criteria for PCOS: Any Two of Three
SELF-CHECK
A 25-year-old woman has regular ovulatory cycles, no hirsutism, normal testosterone, and presents only for a routine pelvic scan for a minor unrelated complaint. The transvaginal ultrasound incidentally reports 'both ovaries show polycystic morphology with 22 follicles each'. What is the correct interpretation and action?
A. Diagnose PCOS, as the ultrasound shows clear polycystic ovarian morphology in both ovaries
B. This is an incidental polycystic-appearing ovary; she does not meet Rotterdam criteria as she has no oligo-ovulation and no hyperandrogenism, so no PCOS label is applied
C. Start combined oral contraceptives immediately to prevent progression to PCOS
D. Repeat the scan monthly for a year to watch for the development of PCOS
Reveal Answer
Answer: B. This is an incidental polycystic-appearing ovary; she does not meet Rotterdam criteria as she has no oligo-ovulation and no hyperandrogenism, so no PCOS label is applied
PCOS requires any TWO of three Rotterdam criteria (oligo/anovulation, hyperandrogenism, polycystic ovarian morphology). This woman has only the ultrasound morphology and no clinical or biochemical features — so she has an incidental polycystic-appearing ovary, NOT PCOS. Ultrasound morphology alone never diagnoses the syndrome. Labelling her or starting treatment would be incorrect over-diagnosis; reassurance is appropriate.
CLINICAL PEARL
Pearl 1 — The scan does not diagnose PCOS by itself. Polycystic ovarian morphology is ONE of three Rotterdam criteria; the diagnosis needs any two, after excluding mimics. A polycystic-appearing ovary in a woman with regular cycles and no androgen excess is an incidental finding, not a disease.
Pearl 2 — Know which follicle threshold goes with which probe. With a modern high-frequency transvaginal transducer the threshold is ≥20 follicles of 2-9 mm per ovary (2018 guideline); the older ≥12 threshold applies only to lower-frequency equipment. Ovarian volume >10 mL is the fallback criterion when follicles cannot be counted, as on transabdominal scanning.
Pearl 3 — Do not use ovarian morphology to diagnose PCOS in adolescents. Within 8 years of menarche multifollicular ovaries are physiologically common; in this group the diagnosis rests on clinical and biochemical criteria, and the scan is unreliable for the morphological criterion.
Self-Assessment — Imaging Decisions in Suspected PCOD
Work through these scenarios as if you are the clinician in the gynaecology clinic. Decide on the modality, interpret the findings, and place them within the diagnostic framework before reading the discussion. The aim is to integrate the imaging into a complete clinical decision, which is exactly what RD7.1 expects of you.
Scenario A: A 28-year-old sexually active woman has had periods only three times in the past year and has clear hirsutism with a raised free androgen index. The clinician asks whether an ultrasound is necessary to make the diagnosis.
Discussion: She already meets TWO Rotterdam criteria — oligo-ovulation and hyperandrogenism — so PCOS can be diagnosed without the scan, provided mimics (thyroid disease, hyperprolactinaemia, non-classical CAH) are excluded. A transvaginal ultrasound is reasonable to assess the ovaries and endometrium and to exclude other pelvic pathology, but it is confirmatory, not required for the diagnosis. The imaging here adds completeness, not the diagnosis itself.
Scenario B: A 17-year-old, two years post-menarche and not sexually active, has irregular cycles and mild acne. A transabdominal ultrasound reports 'bulky ovaries with multiple small follicles'. Should she be diagnosed with PCOS on this basis?
Discussion: No. She is within 8 years of menarche, when multifollicular ovaries are physiologically common, so ultrasound morphology must NOT be used to diagnose PCOS in her age group. The transabdominal route also limits reliable follicle counting, so ovarian volume would be the only usable morphological measure. Her diagnosis should rest on clinical and biochemical criteria with follow-up; an early PCOS label based on her scan would be over-diagnosis.
Scenario C: A 30-year-old woman with a six-month history of rapidly worsening hirsutism, deepening voice and clitoromegaly has a markedly raised serum testosterone. The clinician orders a transvaginal ultrasound. What are you most concerned to exclude, and what is the next step if the ovaries look unremarkable?
Discussion: Rapidly progressive virilisation with a very high testosterone is a red flag for an androgen-secreting tumour (ovarian or adrenal), not simple PCOS. The transvaginal scan looks for an ovarian mass; if the ovaries are unremarkable, the next step is dedicated cross-sectional imaging — MRI of the pelvis and/or CT of the adrenals — to find an adrenal source. The tempo and severity of the presentation, not the PCOM appearance, drive this pathway.