Page 4 of 14
RD7.5 | Imaging in Foreign Body Aspiration — SDL Guide
Learning Objectives
- Recognise the clinical scenario of foreign body aspiration in a child and appreciate that clinical suspicion, not the radiograph, drives the pathway.
- Justify the imaging strategy — frontal chest radiograph first-line, expiratory and lateral-decubitus views and fluoroscopy to unmask air-trapping, CT in selected cases — applying ALARA.
- Distinguish the direct visualisation of a radio-opaque foreign body from the indirect signs of a radiolucent foreign body (unilateral hyperinflation/air-trapping, atelectasis, mediastinal shift, obstructive pneumonia).
- State the central rule that a normal chest radiograph does NOT exclude an inhaled foreign body.
- Integrate imaging findings into management, recognising that bronchoscopy is the definitive diagnostic and therapeutic step when suspicion is high.
INSTRUCTIONS
Foreign body aspiration is a true paediatric emergency that hides in plain sight: the choking episode may be unwitnessed, the child may look well an hour later, and — because most inhaled objects in children are organic and radiolucent — the chest X-ray may be entirely normal. The most dangerous error in this topic is to be falsely reassured by a normal film. This module teaches you to suspect aspiration clinically, to use plain radiography and its special views intelligently while respecting a child's radiosensitivity, to read the indirect signs that betray a hidden foreign body, and to understand why bronchoscopy — not imaging — is the final arbiter.
References
- Sutton's Textbook of Radiology and Imaging, Chapter on Paediatric Chest (textbook)
- Grainger & Allison's Diagnostic Radiology, Chapter on Airway and Paediatric Chest Imaging (textbook)
- Paediatric airway foreign body management guidance (ERS/ESPR and national paediatric protocols) (guideline)
- AERB safety guidance and the Image Gently / ALARA principle for paediatric radiology (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 14-month-old was eating peanuts when she suddenly coughed, choked, and went briefly blue. By the time she reaches casualty twenty minutes later she is pink, alert, and playing — and the anxious team is tempted to relax. A chest radiograph is taken and reported as normal. Is she safe to send home? Absolutely not. Most objects that children inhale are organic — a peanut, a piece of seed, a bit of food — and these are radiolucent: they cast no shadow on an X-ray. The film can look perfectly normal while a peanut sits lodged in a bronchus, slowly setting up obstruction, infection, and inflammation. The single most important lesson of this module is the one that runs against instinct: a normal chest X-ray does not exclude an inhaled foreign body. The history of a choking episode, not the radiograph, is what determines whether this child needs a bronchoscopy.
WHY THIS MATTERS
Foreign body aspiration is among the commonest causes of accidental death in toddlers and a frequent paediatric emergency in every Indian hospital, where groundnuts and seeds are widely available to small children. The diagnosis is treacherous precisely because the most reliable imaging tool — the plain chest film — is so often normal, and because the acute choking episode may be brief or unwitnessed. The NMC competency RD7.5 requires you to integrate imaging findings into the management of foreign body aspiration: that means knowing what the film can and cannot show, how to coax out the indirect signs of a hidden radiolucent object, and when to escalate to bronchoscopy regardless of the radiograph. Misreading 'normal film' as 'no foreign body' is a classic, dangerous, and entirely avoidable clinical error — this module exists to prevent it.
RECALL
Before reading further, recall the foundations this module builds on:
- Ball-valve obstruction (from respiratory physiology): a partially obstructing bronchial foreign body often lets air IN on inspiration (when bronchi widen) but traps it on expiration (when bronchi narrow) — a 'ball-valve' effect. The result is air-trapping: the affected lung stays hyperinflated and empties poorly, which is the mechanism behind the key indirect sign.
- Paediatric radiation sensitivity (from RD-foundation): children are more radiosensitive with a longer latency, so plain films (and especially fluoroscopy and CT) must be justified and dose-minimised — the ALARA / 'Image Gently' principle.
- Bronchial anatomy: the right main bronchus is shorter, wider and more vertical than the left, so inhaled objects lodge in the right side more often, though either side (and the trachea) can be involved.
- Atelectasis: when a foreign body completely obstructs a bronchus, the trapped air distal to it is absorbed and the lung segment collapses — producing volume loss, opacity, and shift of structures TOWARDS the collapsed side.
Clinical Scenario — Sudden Choking, Then a Deceptively Quiet Child
The clinical scenario of foreign body aspiration is defined far more by its history than by any imaging finding, and recognising the pattern is the first and most decisive step. The classic presentation is a toddler — typically between six months and three years — who has a sudden choking episode while eating or playing with a small object: an abrupt bout of coughing, gagging, or transient cyanosis, often witnessed by a parent. This acute event may be followed by a deceptively quiet interval in which the child appears well, because the object has settled into a bronchus and the immediate irritation has subsided. It is this asymptomatic interval that lulls the unwary into discharging the child. Later, if the object remains, the child may develop a persistent cough, unilateral wheeze, recurrent or non-resolving pneumonia in the same location, or stridor if the foreign body sits in the larynx or trachea.
The cardinal principle of the clinical assessment is that a convincing history of a choking episode is itself an indication to investigate definitively, regardless of how well the child looks or what the X-ray shows. Key features that raise or confirm suspicion include:
- A witnessed choking/coughing episode, especially with a small food item (groundnut, seed) or toy.
- Asymmetric chest findings — unilateral reduced air entry, a localised wheeze, or a 'monophonic' wheeze that does not move.
- Recurrent or non-resolving pneumonia confined to one lung region, which should always prompt the question 'could this be a retained foreign body?'
- Sudden stridor or respiratory distress suggesting a laryngeal or tracheal object — a more immediate emergency.
Imaging in this scenario is an adjunct that supports the clinical suspicion and helps localise the problem; it is not the test that rules the diagnosis in or out. Holding that hierarchy clearly in mind — history first, imaging second, bronchoscopy as the arbiter — is what keeps a hidden peanut from being sent home.
Imaging Strategy — Plain Film First, Special Views to Unmask Air-Trapping
When foreign body aspiration is suspected, imaging begins with the lowest-dose useful test and escalates only as far as the clinical question requires — the same ALARA logic that governs all paediatric imaging, applied to a child who may need several films. The aim of imaging here is not to 'prove' aspiration (the plain film frequently cannot) but to look for a directly visible object and, far more often, to unmask the indirect signs of a radiolucent one. Used thoughtfully, a few well-chosen views answer most of the practical questions while keeping dose low.
Frontal chest radiograph (CXR) — first-line. A standard frontal film is the starting investigation. A radio-opaque foreign body (metal, dense plastic, bone fragment) is seen directly. The much commoner radiolucent organic object is invisible, so the film is examined instead for indirect signs — particularly asymmetric lung lucency suggesting air-trapping, areas of collapse, mediastinal position, and any obstructive pneumonia.
Expiratory and lateral-decubitus films — to bring out air-trapping. Because ball-valve air-trapping may be subtle on a routine inspiratory film, additional views help: an expiratory film exaggerates the difference — the normal lung deflates and becomes denser while the obstructed, air-trapped lung stays hyperinflated and lucent, and the mediastinum shifts away from the obstructed side on expiration. In an uncooperative young child who cannot perform a forced expiration, a lateral-decubitus film (child lying on one side) is used: the dependent normal lung deflates, whereas an air-trapped lung resists deflation and stays inflated.
Fluoroscopy — dynamic assessment. Fluoroscopy can show the air-trapping dynamically (the obstructed lung failing to deflate and the mediastinum swinging on respiration), but it delivers ongoing radiation and is used selectively.
CT — selected equivocal cases. CT can demonstrate an endobronchial object and its effects but adds substantial dose; it is reserved for genuinely equivocal cases where the diagnosis remains unclear and the result would change management.
Bronchoscopy — the definitive step. Critically, bronchoscopy is both diagnostic and therapeutic: it directly visualises and removes the object. When clinical suspicion is high, the pathway leads to bronchoscopy whatever the radiograph shows — imaging informs the procedure but does not replace it.
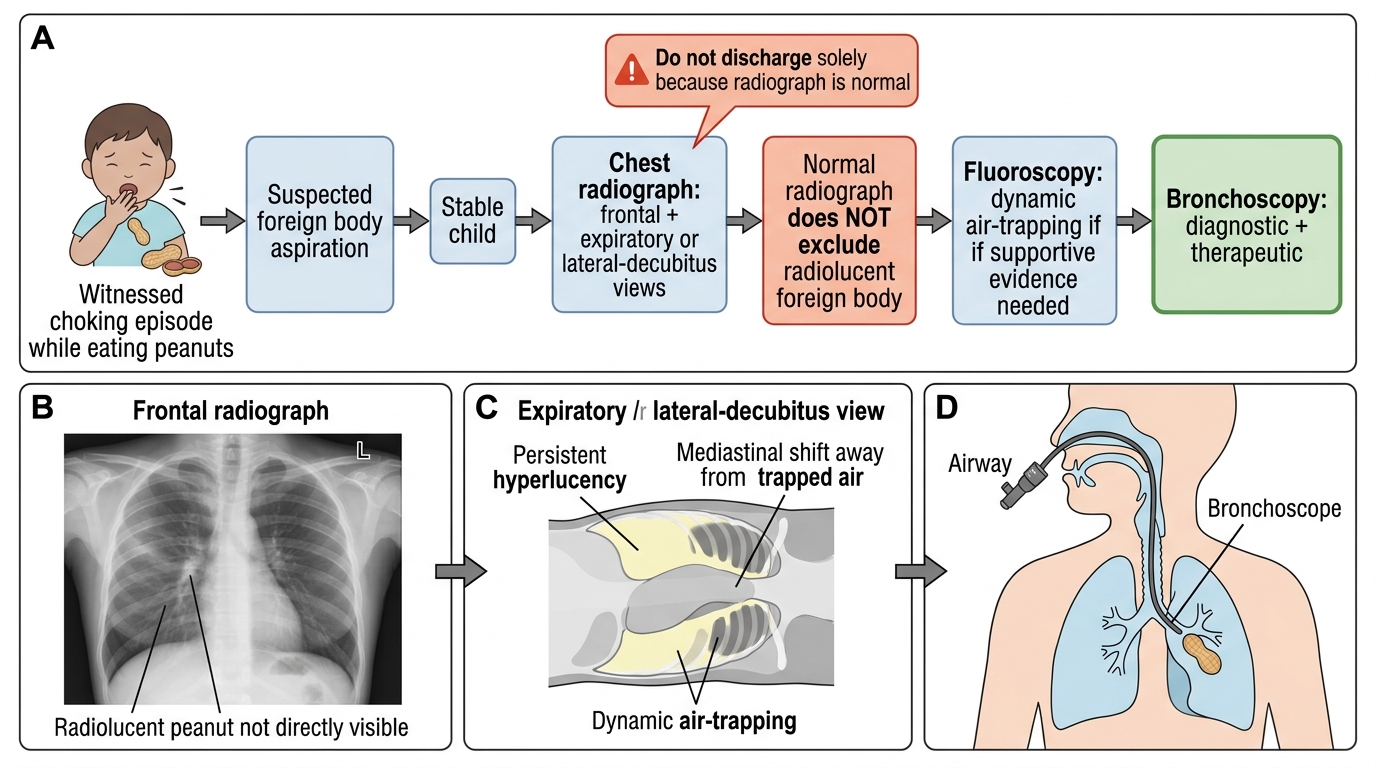
Suspected Foreign Body Aspiration in a Child
SELF-CHECK
A 2-year-old had a witnessed choking episode while eating peanuts. He is now stable. The frontal chest radiograph is reported as normal. What is the correct interpretation and next step?
A. A normal radiograph excludes aspiration; reassure and discharge
B. A normal radiograph does NOT exclude a radiolucent foreign body; given the convincing history, proceed to bronchoscopy (consider expiratory/decubitus views to support the case)
C. Start broad-spectrum antibiotics and review in one week with a repeat film
D. Obtain an MRI chest to detect the radiolucent peanut directly
Reveal Answer
Answer: B. A normal radiograph does NOT exclude a radiolucent foreign body; given the convincing history, proceed to bronchoscopy (consider expiratory/decubitus views to support the case)
Most aspirated objects in children are organic and radiolucent, so a normal chest radiograph is common and does NOT exclude a foreign body. A convincing history of choking is itself an indication for definitive evaluation. The appropriate next step is bronchoscopy, which is both diagnostic and therapeutic; expiratory or lateral-decubitus views may add supportive indirect signs but a normal film must never be used to discharge a child with a convincing history. MRI is not the tool for an inhaled peanut.
Imaging Findings and Their Interpretation — Direct and Indirect Signs
Interpreting the radiograph in suspected aspiration means reading two quite different stories: the rare, easy one of an object you can see, and the common, subtle one of an object you cannot. Because the majority of inhaled foreign bodies in children are radiolucent, the skilled reader spends most effort hunting for the indirect, mechanism-based signs rather than the object itself. Each indirect sign is a downstream consequence of bronchial obstruction, so understanding the mechanism lets you predict and recognise the finding rather than memorising a disconnected list. Reason from the obstruction to its effect on air movement, lung volume, and the position of the mediastinum.
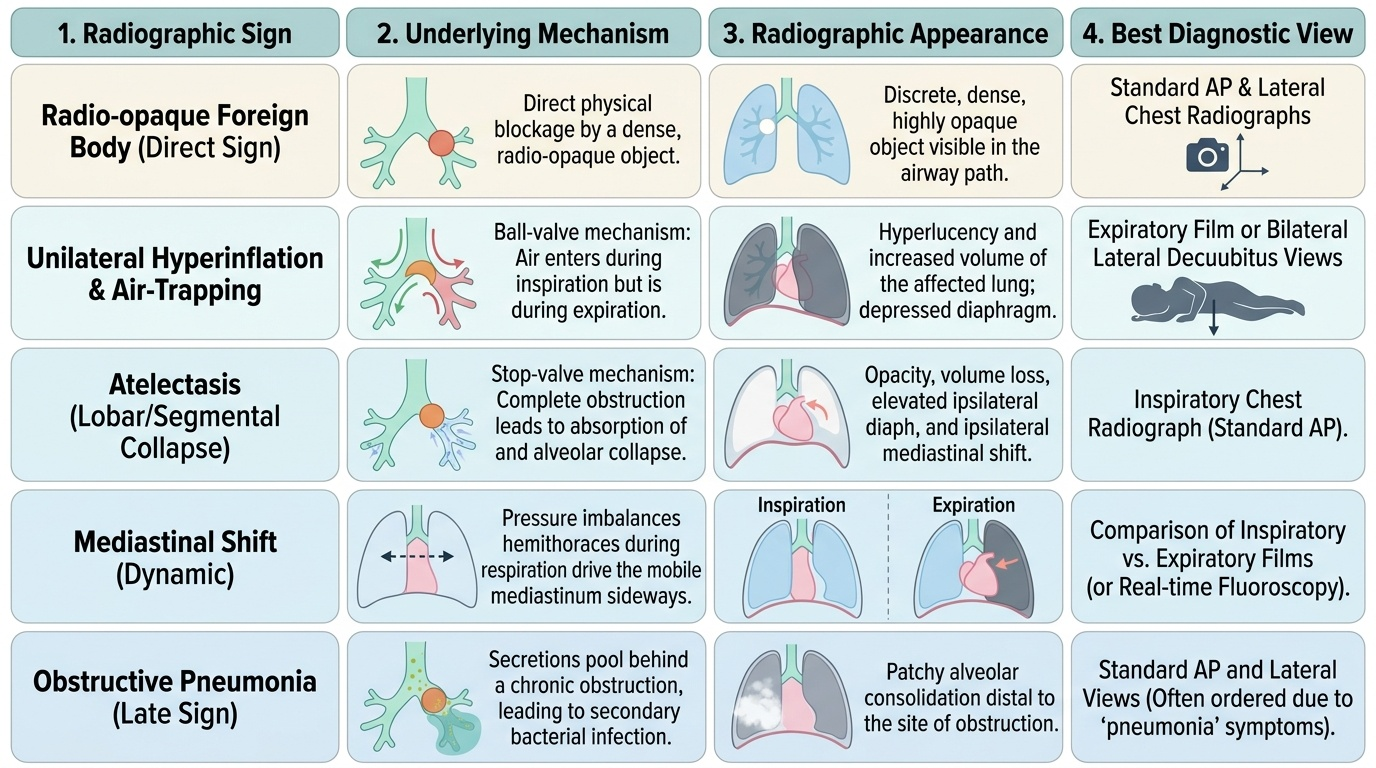
Direct sign — the radio-opaque object. A metallic or otherwise dense foreign body is seen directly on the film as a discrete opaque object in the airway, and its position can be localised. This is the straightforward minority.
Indirect signs — the radiolucent object's footprint:
- Unilateral hyperinflation / air-trapping (the classic sign): a partial, ball-valve obstruction lets air in but not out, so the affected lung is hyperinflated and abnormally lucent, and this is exaggerated on the expiratory or lateral-decubitus film. On expiration the mediastinum shifts AWAY from the obstructed (hyperinflated) side, because that lung cannot empty.
- Atelectasis (collapse): if the object completely obstructs a bronchus, distal air is absorbed and the segment collapses — producing opacity, volume loss, and mediastinal shift TOWARDS the collapsed side. Note the opposite directions of shift in air-trapping versus collapse.
- Obstructive (post-obstructive) pneumonia: a retained object predisposes to infection beyond it, producing consolidation that is often persistent or recurrent in the same location.
The over-arching interpretive rule: the plain film is frequently completely normal in the early hours after aspiration of a radiolucent object. A normal film therefore never excludes the diagnosis — it only fails to confirm it. When the history is convincing, the negative film is set aside and the child proceeds to bronchoscopy.
Provided image
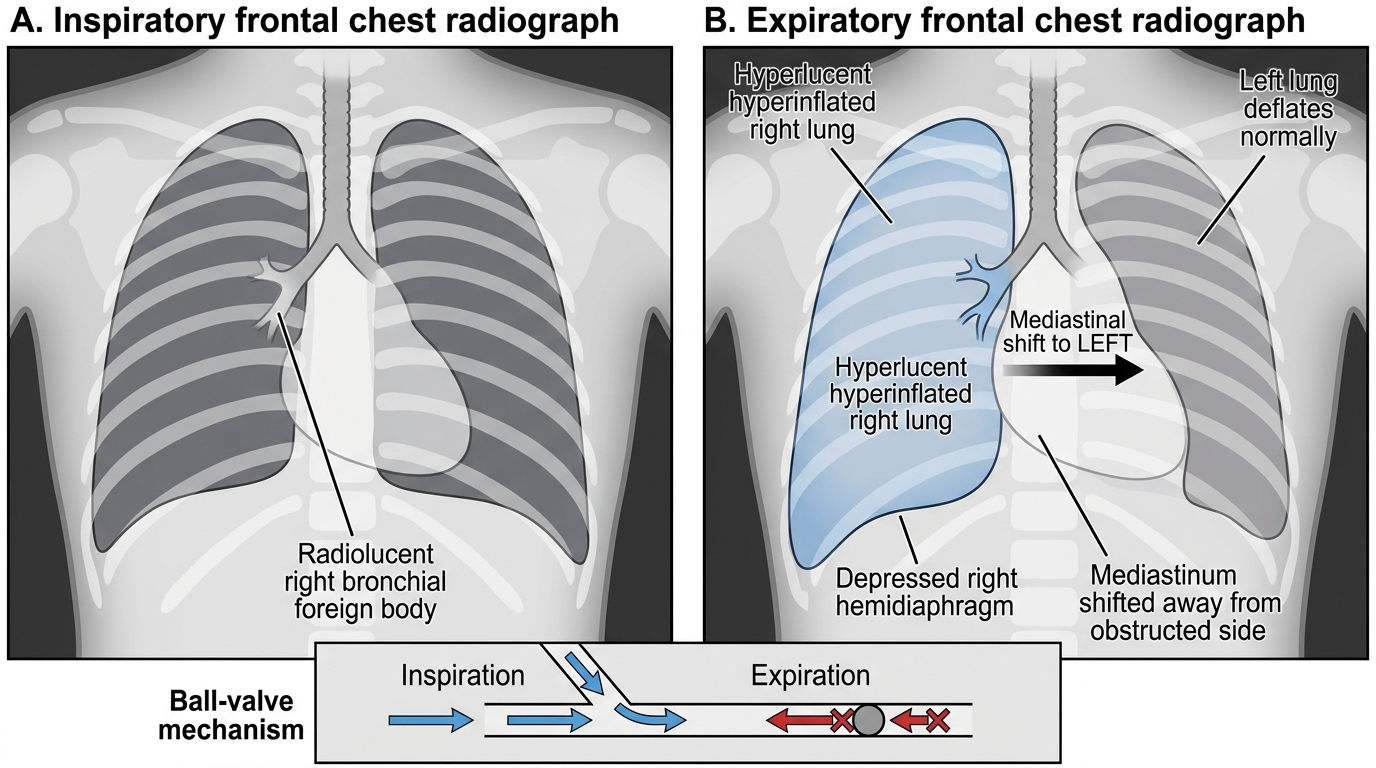
Right Bronchial Foreign Body: Expiratory Air-Trapping
SELF-CHECK
On an expiratory chest film of a child with suspected aspiration, the right lung remains lucent and hyperinflated while the left deflates normally, and the mediastinum is shifted to the LEFT. What does this indicate?
A. Complete obstruction with collapse of the right lung
B. Ball-valve obstruction with air-trapping in the right lung; the mediastinum shifts away from the obstructed (hyperinflated) side on expiration
C. A normal expiratory film with no significant findings
D. A large right pleural effusion pushing the mediastinum to the left
Reveal Answer
Answer: B. Ball-valve obstruction with air-trapping in the right lung; the mediastinum shifts away from the obstructed (hyperinflated) side on expiration
A lung that stays lucent and hyperinflated on expiration while the other deflates is classic ball-valve air-trapping: air enters but cannot leave the obstructed side. On expiration the trapped lung cannot empty, so the mediastinum is pushed AWAY from the obstructed side (here, to the left). Complete obstruction would instead cause collapse with the mediastinum shifting TOWARDS the affected side. The pattern is the footprint of a radiolucent foreign body, not a normal film or a pleural effusion.