Page 1 of 14
RD7.5 | Imaging in Pediatric Chest Infection — SDL Guide
Learning Objectives
- State when a child with a suspected respiratory infection does, and does not, need chest imaging, applying the principle that uncomplicated clinical community-acquired pneumonia usually requires no routine radiograph.
- Justify the paediatric imaging hierarchy — chest radiograph first-line, ultrasound for pleural fluid, CT reserved for complications — on the basis of ALARA and paediatric radiosensitivity.
- Recognise and interpret the expected imaging appearances of consolidation, bronchopneumonia, pleural effusion, empyema, necrotising pneumonia and round pneumonia.
- Integrate provided imaging findings into a management decision for a child with a chest infection, including when to drain a pleural collection and when to escalate.
- Apply 'image gently' practice — weight/size-adjusted technique and avoidance of unnecessary ionising imaging — in every paediatric chest imaging decision.
INSTRUCTIONS
Respiratory infection is one of the commonest reasons a child is brought to hospital, and one of the leading causes of childhood death worldwide. The temptation to 'just get a chest X-ray' is strong — but children are more radiosensitive than adults and carry a longer lifetime to express any radiation-induced harm, so every ionising study must earn its place. This module teaches you to decide WHEN imaging is needed, WHICH modality answers the clinical question with the least harm, HOW to read the expected findings, and HOW those findings change management. Work through it as the clinician who will order (or wisely withhold) these investigations.
References
- Sutton's Textbook of Radiology and Imaging, Chapter on Paediatric Chest (textbook)
- Grainger & Allison's Diagnostic Radiology, Chapter on Imaging of the Paediatric Chest (textbook)
- WHO Integrated Management of Childhood Illness (IMCI) and BTS guidelines for community-acquired pneumonia in children (guideline)
- AERB safety guidance and the Image Gently / ALARA principle for paediatric radiology (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 3-year-old is carried into the paediatric casualty at midnight — fever for two days, fast breathing, and a cough his mother describes as 'rattling'. The intern's reflex is to write 'CXR'. But pause: this child has classic clinical pneumonia, he is feeding, he is not hypoxic, and his chest signs are localised. Will an X-ray change anything you do? In most such children the answer is no — the diagnosis is clinical and the treatment is oral antibiotics. Yet two beds away lies an 8-year-old, three days into 'pneumonia', now spiking again, with a dull, silent base on the left. For her, imaging is not optional — it will reveal whether pus has collected in the pleura and needs a drain. The skill of paediatric chest imaging is not knowing how to order a film; it is knowing which child needs one, which child needs an ultrasound, and which child you can safely treat without any radiation at all.
WHY THIS MATTERS
Pneumonia remains a leading killer of children under five, and chest infection fills paediatric wards in every Indian hospital. Imaging sits at the centre of two opposing pressures. On one side, over-imaging exposes a radiosensitive child to ionising radiation that confirms what the clinician already knew. On the other side, under-imaging misses the empyema, the necrotising pneumonia, or the inhaled foreign body masquerading as infection. The NMC competency RD7.5 asks you to integrate imaging findings into the management of paediatric chest infection — not to memorise a list of pictures, but to reason from the clinical question to the right modality and from the image back to the bedside decision. Every paediatric posting and every casualty night will test exactly this judgement, and getting it right protects the child both from the disease and from the investigation.
RECALL
Before reading further, recall the foundations this module builds on:
- Paediatric radiation sensitivity (from RD-foundation): children have more actively dividing cells and a longer remaining lifespan in which a radiation-induced malignancy can manifest, so a given radiation dose carries greater lifetime risk than in an adult. This underpins the ALARA ('As Low As Reasonably Achievable') principle and the 'Image Gently' campaign — use non-ionising modalities where they answer the question, and size-/weight-adjust technique when ionising imaging is necessary.
- Patterns of pneumonia (from pathology): lobar pneumonia is confluent consolidation of a whole lobe or segment, classically pneumococcal; bronchopneumonia is patchy, multifocal, often peribronchial consolidation, common in younger children and with staphylococcal or viral-bacterial disease.
- Consolidation on X-ray: alveoli fill with inflammatory exudate, replacing air; this raises the density of lung so it appears white (opaque), and air remaining in the bronchi running through it produces dark branching air bronchograms.
- The pleural space: a potential space between visceral and parietal pleura; fluid (effusion or pus/empyema) collects here dependently and blunts the costophrenic angle on an erect film, or layers on a decubitus film or ultrasound.
Clinical Scenario — The Febrile, Coughing Child and When Imaging Helps
The first and most important decision in imaging a child with a chest infection is whether to image at all. For the great majority of children with community-acquired pneumonia (CAP), the diagnosis is clinical — fever, cough, tachypnoea (using age-specific respiratory-rate thresholds), chest indrawing, and focal auscultatory signs — and a child who is feeding, not hypoxic, and improving on oral antibiotics does not need a radiograph to confirm what the bedside has already established. WHO and most paediatric guidance are explicit on this point: a routine chest radiograph is not required to diagnose or to manage uncomplicated clinical pneumonia in a child. Ordering one anyway adds ionising radiation to a radiosensitive patient without changing the treatment, and a normal early film can even falsely reassure. The clinician's instinct to 'get a film for completeness' is precisely the instinct that ALARA exists to restrain.
Imaging earns its place when the clinical picture is complicated, atypical, or failing to follow the expected course. The indications that mandate a chest radiograph in a child with suspected or proven chest infection include:
- Severe disease or respiratory distress — hypoxia (low SpO2), marked tachypnoea, grunting, severe indrawing, or a child sick enough to need admission and oxygen.
- Suspected complication — persistent or recurrent fever after 48–72 hours of appropriate antibiotics, a dull, silent lung base (suggesting effusion or empyema), or clinical deterioration.
- Diagnostic uncertainty — to distinguish pneumonia from other causes of respiratory distress (cardiac failure, foreign body, mass) when the clinical picture is unclear.
- Non-resolving or recurrent infection — pneumonia that fails to clear, or repeated infection in the same location, raising suspicion of an underlying structural lesion, sequestration, or retained foreign body.
- Suspected inhaled foreign body — where indirect signs are sought (covered in the companion module).
In each of these the radiograph is being used not to label 'pneumonia' but to answer a specific further question — is there a drainable collection? a complication? an alternative diagnosis? That clarity of purpose is what separates justified imaging from reflex imaging.
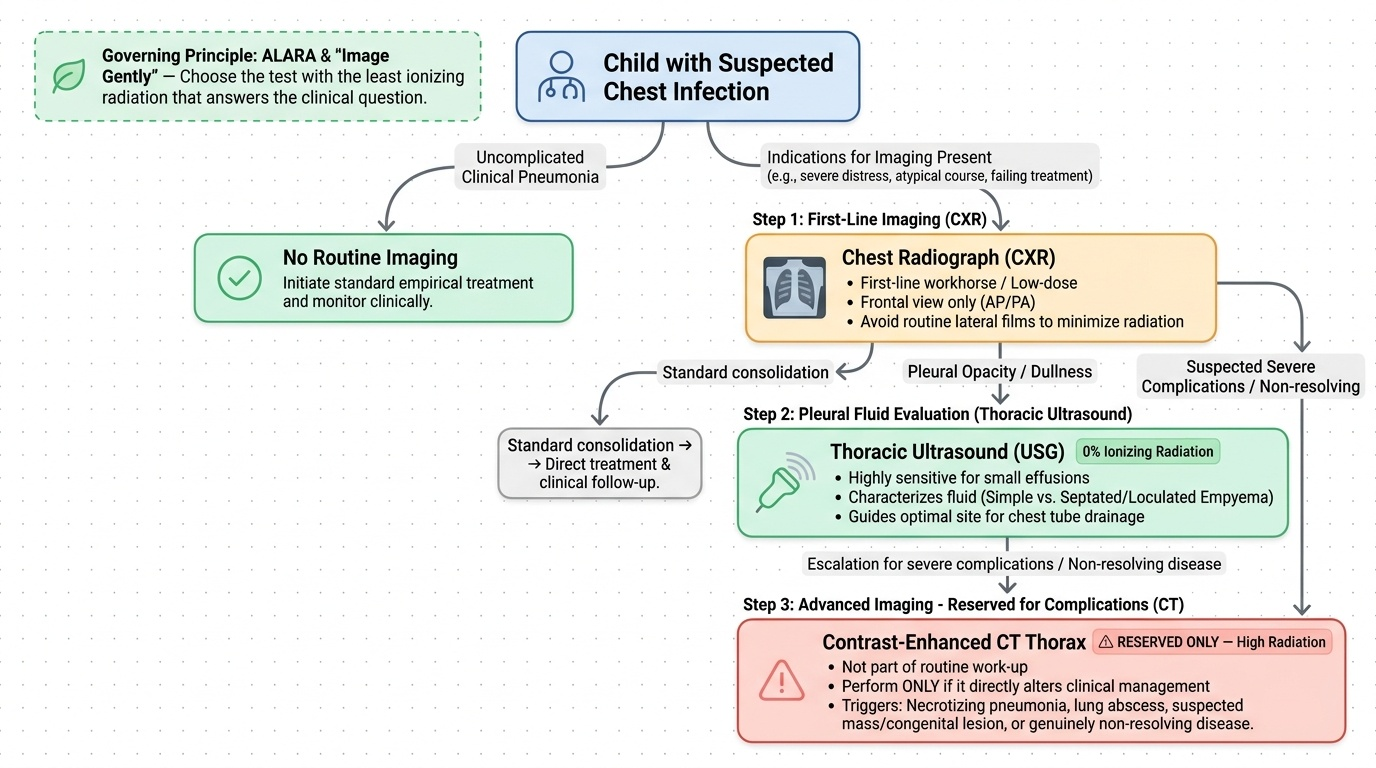
Imaging Strategy — CXR First, Ultrasound for Fluid, CT Only for Complications
Once imaging is indicated, the choice of modality follows a deliberate hierarchy built around a single governing principle: in children, prefer the test that answers the clinical question with the least ionising radiation. Because the paediatric patient is more radiosensitive and has decades in which any harm may manifest, the strategy deliberately front-loads the lowest-dose useful test and reserves high-dose imaging for situations where it genuinely changes management. This is the clinical embodiment of ALARA and the 'Image Gently' philosophy, and it should shape every order you write.
Chest radiograph (CXR) — the first-line and mainstay. A frontal chest film is fast, cheap, universally available, and low-dose, and it answers most of the questions that justify imaging in the first place: is there consolidation, where, and is there a pleural collection or a complication? A single frontal (AP in infants, PA in older cooperative children) film is usually sufficient; a routine lateral film is generally not needed and adds dose. The CXR is the workhorse and the default whenever imaging is required for a chest infection.
Thoracic ultrasound (USG) — for pleural fluid, no radiation. When the radiograph shows a pleural opacity or a base that is dull clinically, ultrasound is the next step — and it carries no ionising radiation at all, which makes it especially attractive in children. USG is more sensitive than the plain film for small effusions and, crucially, it characterises the fluid: it distinguishes a simple, free-flowing effusion from a septated, loculated empyema, and it can guide the optimal site for drainage. It is operator-dependent, but in skilled hands it often answers the management question without any further radiation.
Contrast-enhanced CT thorax — reserved for complications. CT delivers a substantially higher radiation dose than a plain film and is therefore deliberately held back. It is not part of the routine work-up of paediatric pneumonia. CT is justified only when a serious complication or alternative diagnosis is suspected and would alter management — necrotising pneumonia, lung abscess, a suspected underlying mass or congenital lesion, or genuinely non-resolving disease despite appropriate treatment. When CT is performed in a child, it must be done with paediatric, weight-/size-adjusted low-dose protocols.
Provided image
SELF-CHECK
A 2-year-old has a 2-day history of fever and cough, respiratory rate appropriately raised for age, is feeding well, SpO2 98% in room air, and has focal crackles in the right lower zone. The clinical diagnosis is uncomplicated community-acquired pneumonia. What is the most appropriate imaging step?
A. Routine frontal chest radiograph to confirm the diagnosis before starting antibiotics
B. No routine imaging; treat clinically with oral antibiotics and image only if the child deteriorates or fails to improve
C. CT thorax to define the extent of consolidation accurately
D. Both frontal and lateral chest radiographs as a baseline for future comparison
Reveal Answer
Answer: B. No routine imaging; treat clinically with oral antibiotics and image only if the child deteriorates or fails to improve
Uncomplicated clinical community-acquired pneumonia in a child does NOT require a routine chest radiograph — the diagnosis is clinical and a film will not change management. Adding ionising radiation to a radiosensitive child without altering treatment violates ALARA. Imaging (starting with a frontal CXR) is reserved for severe disease, suspected complications, diagnostic uncertainty, or failure to improve. A lateral film and CT are both unnecessary and add dose here.
Imaging Findings and Their Interpretation — Consolidation, Effusion, Complications
When a chest film or ultrasound is obtained in a child with infection, the value lies in reading it accurately and translating the appearance into a clinical meaning. The findings in paediatric chest infection range from the straightforward (a lobar opacity that confirms uncomplicated pneumonia) to the management-changing (a loculated empyema or a necrotising lung), and the same density on a film can mean very different things. Interpreting these appearances correctly — and recognising when a finding signals a complication rather than simple infection — is the core interpretive skill this competency demands. Reason from the underlying pathology to the image and back again, rather than treating each picture as an isolated pattern to be matched.
Consolidation and its patterns. Consolidation is alveolar filling by exudate; it appears as an area of increased opacity (whiteness) that may contain dark branching air bronchograms — the hallmark that the opacity is alveolar (lung) rather than pleural fluid. Lobar consolidation is a confluent, segment- or lobe-shaped opacity, classically pneumococcal, and often confirms an uncomplicated CAP. Bronchopneumonia is patchy, bilateral, peribronchial opacity, common in infants and with staphylococcal or viral-bacterial infection. A peculiarly paediatric pattern is round pneumonia — a well-circumscribed, mass-like rounded opacity (usually a single focus, often posterior lower lobe) seen in young children because their collateral air-drift pathways are immature; it is benign infection but can be mistaken for a tumour, so recognising its typical age and appearance avoids unnecessary alarm and further imaging.
Pleural effusion and empyema. A simple parapneumonic effusion blunts the costophrenic angle on an erect film and layers freely; an empyema is infected, often septated and loculated pleural fluid. The plain film may only show 'an opaque hemithorax' or a blunted angle and cannot reliably tell simple fluid from pus — this is exactly where ultrasound is decisive, demonstrating internal septations, loculations and echogenic fluid that indicate empyema and guiding drainage.
Necrotising pneumonia and abscess. When consolidated lung breaks down, the film may show lucencies within the opacity; contrast-enhanced CT confirms necrotising pneumonia (non-enhancing, breaking-down lung) or a discrete lung abscess (a thick-walled, often fluid-containing cavity). These are the complications that justify the higher dose of CT because they change management.
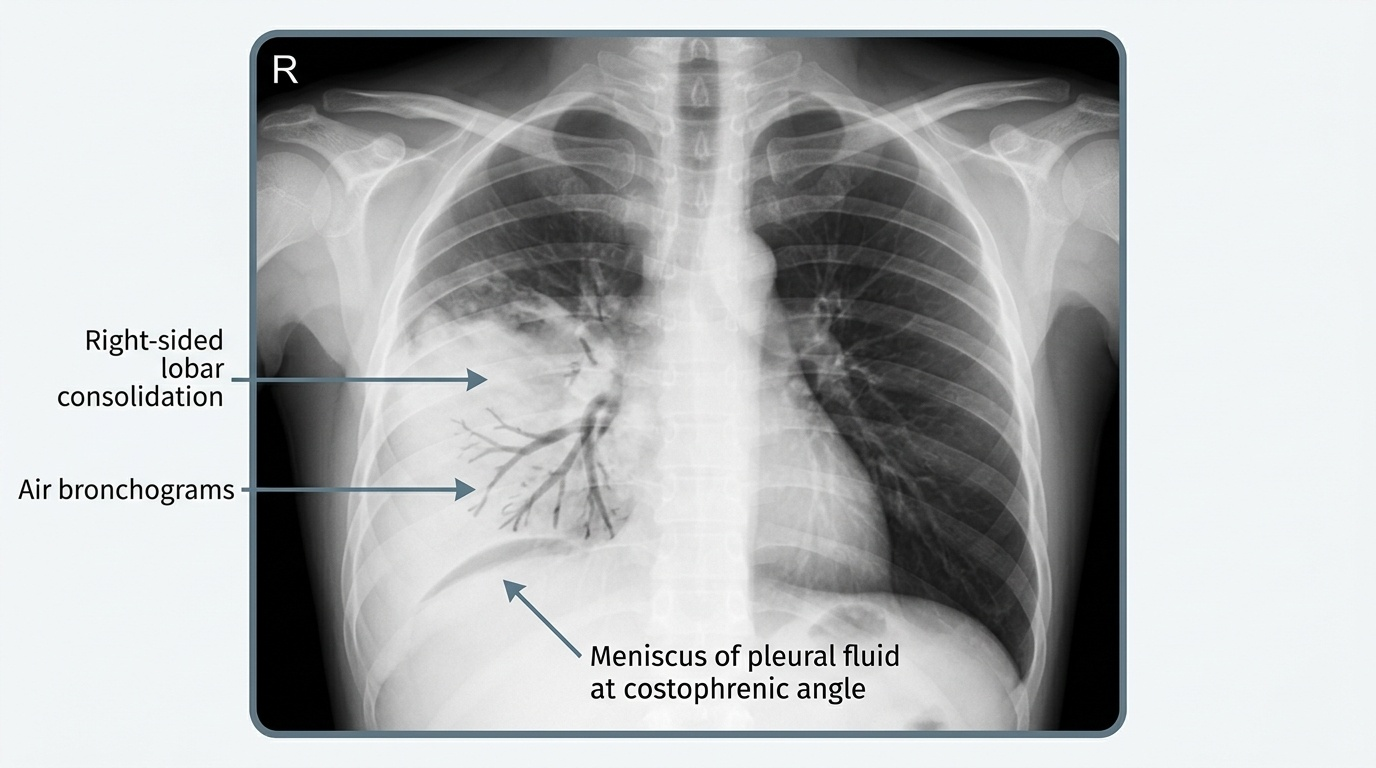
Provided image
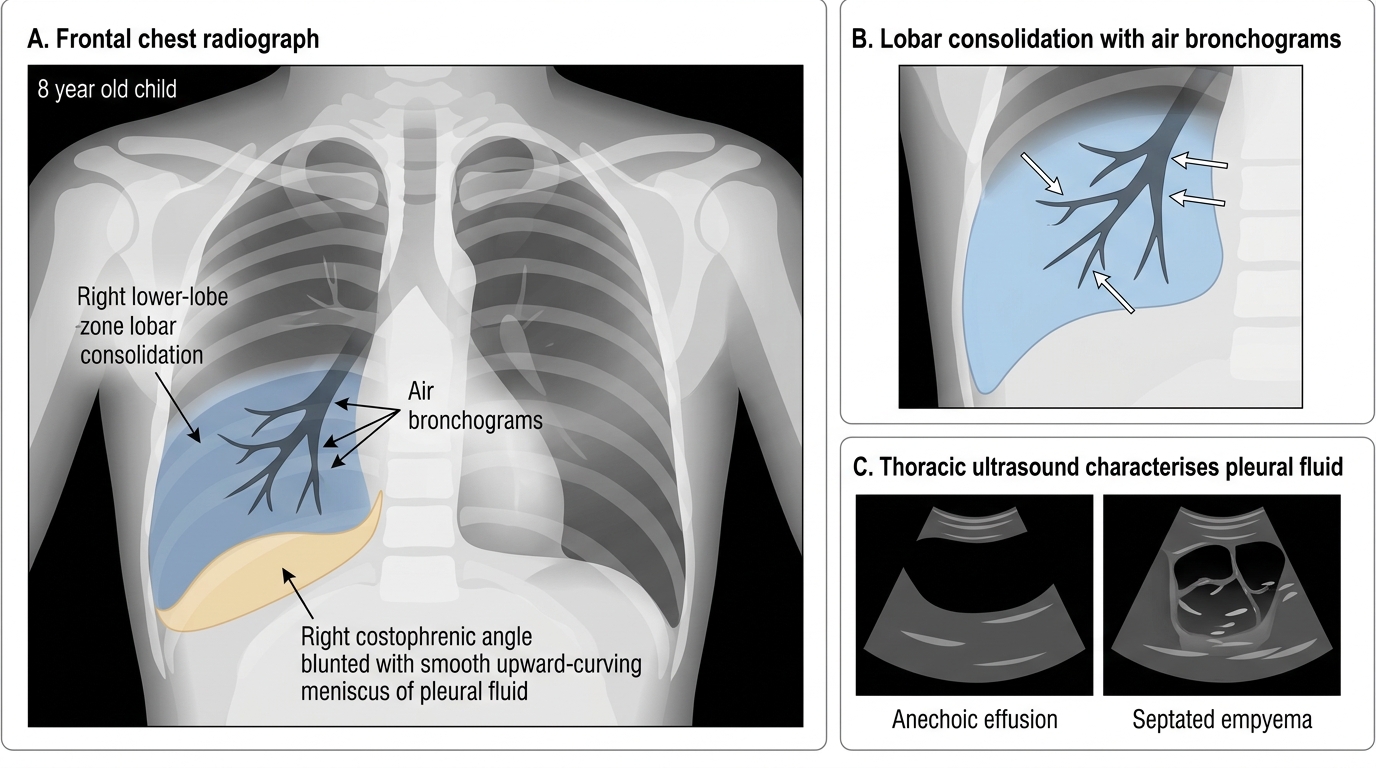
Paediatric Lobar Pneumonia with Pleural Effusion
SELF-CHECK
An 8-year-old with treated pneumonia has a persistent fever and a left lower-zone opacity on chest radiograph that does not clearly show air bronchograms; the left costophrenic angle is blunted. What is the most appropriate next imaging investigation?
A. CT thorax with contrast as the first step to characterise the opacity
B. Thoracic ultrasound to determine whether the pleural collection is a simple effusion or a septated empyema
C. Repeat chest radiograph in one week to look for change
D. MRI chest to assess the pleura without radiation
Reveal Answer
Answer: B. Thoracic ultrasound to determine whether the pleural collection is a simple effusion or a septated empyema
A blunted costophrenic angle with an opacity in a child failing treatment suggests a pleural collection. Thoracic ultrasound is the appropriate next step: it uses no ionising radiation, is more sensitive than the plain film for fluid, distinguishes a simple effusion from a septated/loculated empyema, and can guide drainage. CT is reserved for complications such as necrotising pneumonia or abscess and delivers a much higher dose. A one-week delay is inappropriate in a child failing treatment, and MRI is not the practical first tool for pleural fluid here.