Page 5 of 14
RD3.2 | ALARA Practice and AERB Regulatory Principles — SDL Guide (Part 2)
Clinical and Applied Significance — Applying ALARA and AERB Rules at the Bedside and in the Department
The applied test of this competency is whether you can translate the principles and tools into correct behaviour in three real settings: protecting yourself and staff, protecting patients, and meeting the institution's regulatory obligations. Radiation protection fails not because clinicians lack knowledge but because they do not apply it under the pressure of a busy ward or theatre, so the value of this competency is in building reliable habits. The same triad and the same principles map onto each setting, and the AERB framework sits behind all of them, turning good practice into a legal requirement with named accountable persons.
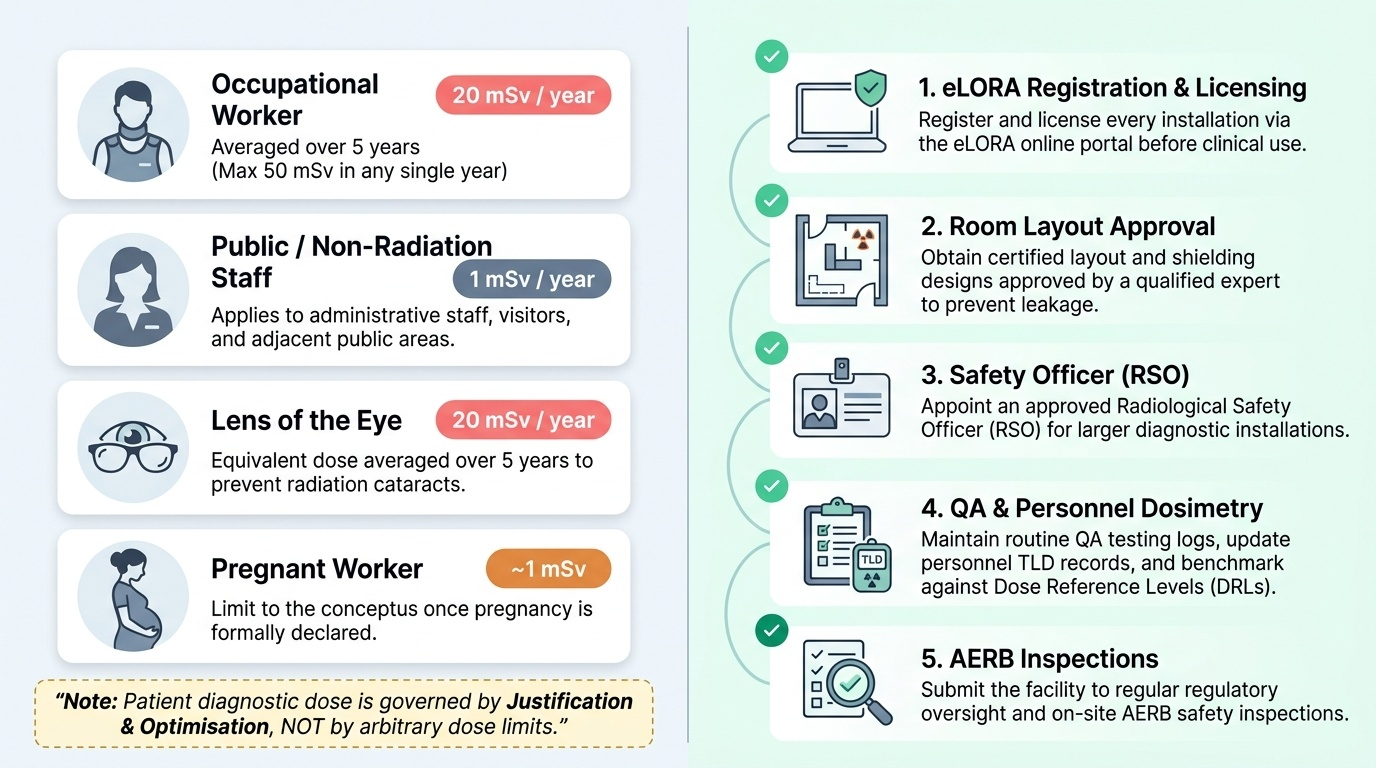
Protecting staff — apply the triad every time: minimise screening time, maximise distance (step back, use the inverse-square law), and always wear appropriate shielding (apron, thyroid shield, lead glasses for interventionalists). Wear your personal dosimeter (TLD) so cumulative dose is monitored against limits. The relevant dose limits are:
| Exposed group | Effective dose limit |
|---|---|
| Occupational (radiation worker) | 20 mSv per year, averaged over 5 years (max 50 mSv in any single year) |
| Public / non-radiation staff | 1 mSv per year |
| Lens of the eye (occupational, equivalent dose) | 20 mSv per year, averaged over 5 years |
| Pregnant worker (to the conceptus, once declared) | ~1 mSv over the declared pregnancy |
Protecting patients — apply justification ('will this change management?') and optimisation: correct collimation, lowest diagnostic-quality exposure factors, paediatric ('child-size') protocols, avoidance of unnecessary repeats, and special care in pregnancy (consider whether a non-ionising modality answers the question, and use shielding/optimised technique if an ionising study is unavoidable). Remember patient diagnostic dose is governed by justification + optimisation, NOT by a dose limit.
Meeting AERB obligations — a facility running an X-ray or CT unit must, under AERB rules:
- Register/license every installation via eLORA before use;
- Have an approved room layout and shielding design certified by a qualified expert;
- Appoint a Radiological Safety Officer (RSO) for larger installations;
- Maintain QA testing, personnel monitoring (dosimetry) records, and follow dose reference levels;
- Submit to AERB inspection and corrective action.
The ordering clinician's specific share of this is justification — never ordering an unjustified ionising study — and supporting optimisation by giving adequate clinical detail so the radiologist can tailor the lowest-dose protocol that answers the question.
Provided image
CLINICAL PEARL
Pearl 1 — Principle vs method: ALARA (optimisation) is a principle; time, distance, shielding are the methods that achieve it. Justification, optimisation (ALARA) and dose limitation are the three principles — and dose limitation does NOT apply to the patient's own diagnostic dose.
Pearl 2 — Distance is king: the inverse-square law means double the distance = quarter the dose. Stepping back is the cheapest, most powerful protection you have. Teach yourself to step back during every exposure you are not performing.
Pearl 3 — AERB, not NRC/ICRP: in India the statutory radiation regulator is the AERB (Atomic Energy Regulatory Board, under the Atomic Energy Act 1962, constituted 1983; registration via eLORA). The ICRP only recommends (advisory, international); the US NRC is American. Citing the NRC or ICRP as 'India's regulator' is a classic examination error.
Self-Assessment — Protection Principles and Regulation
Use these scenarios to test your command of the protection framework, the practical triad and the regulatory facts. Attempt each answer before reading the discussion — retrieval practice is what fixes the principle-versus-method distinction and the AERB facts in memory.
Scenario A: A surgical registrar argues that wearing a lead apron is enough protection during a long fluoroscopy list, so he need not worry about how long the beam is on or where he stands. Where is his reasoning incomplete?
Discussion: He has reduced ALARA to a single tool. The protection triad is time, distance and shielding, and all three must be applied together. A lead apron (shielding) does not protect against prolonged time under the beam, nor does it substitute for distance (the inverse-square law means stepping back is often the single most effective measure). Best practice for a long list combines short, pulsed screening time, stepping back during acquisitions, AND apron plus thyroid shield and lead glasses — the apron alone leaves the eyes and accumulated time-dose unaddressed.
Scenario B: A district hospital wants to install a new CT scanner and the administrator asks whether they can simply start scanning patients once the machine is delivered. What is the correct regulatory answer in India?
Discussion: No. Under AERB rules (the statutory regulator, Atomic Energy Act 1962) the installation must be registered/licensed through eLORA before clinical use, with an approved shielding/room-layout design, a designated Radiological Safety Officer for an installation of that size, personnel-monitoring (dosimetry) arrangements, and a quality-assurance programme. Operating an unregistered installation is a regulatory violation. The AERB — not the ICRP (advisory) or the US NRC (American) — is the body whose approval is required.
Scenario C: A medical physicist tells a worried radiographer that her annual occupational effective-dose limit is 20 mSv averaged over five years, and that a patient she imaged that morning 'must have exceeded her limit' because the CT delivered 10 mSv. Is the physicist's second statement coherent?
Discussion: No — the second statement confuses two groups. Dose limits (20 mSv/yr occupational, 1 mSv/yr public) apply to workers and the public, not to patients' own diagnostic exposure. The patient's 10 mSv CT is governed by justification and optimisation, not by an occupational limit, so it cannot 'exceed her limit' — patients have no diagnostic dose limit. The 20 mSv figure correctly describes the radiographer's occupational limit, averaged over five years (with a 50 mSv single-year ceiling).