Page 11 of 17
RD7.4 | Imaging in Intestinal Obstruction — SDL Guide (Part 2)
Impact on Management — Integrating Findings into Surgical Decisions
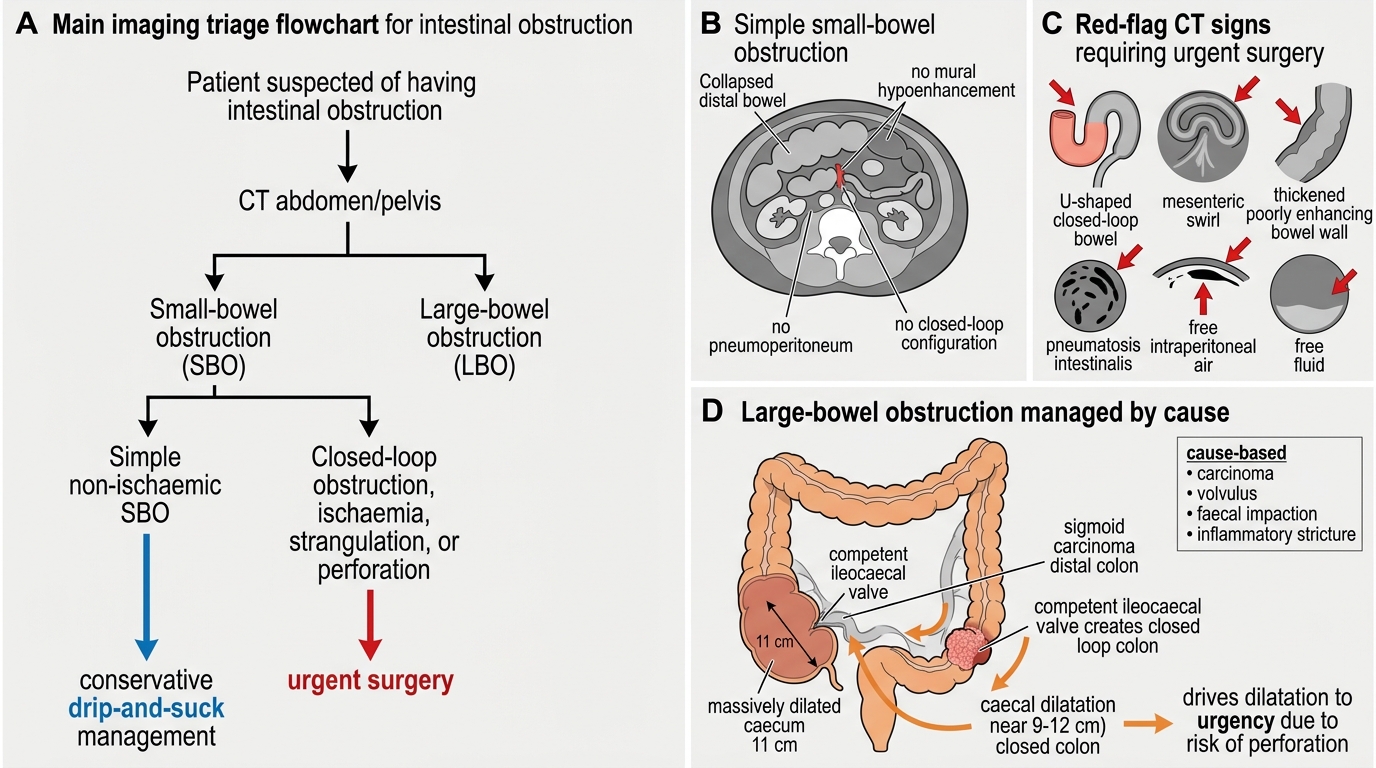
The integrate (KH) heart of RD7.4 is to convert the imaging into a management decision, and in intestinal obstruction the pivotal distinction the imaging draws is between simple obstruction (no ischaemia) that may be managed conservatively, and complicated obstruction (closed-loop, strangulation, perforation) that demands urgent surgery. The clinician reads the CT to answer the surgeon's questions — small or large bowel, what is the cause, is there a closed loop, and is the bowel alive? — and each answer routes the patient. As in the strangulated hernia, the single most decisive observation is whether the bowel wall enhances, because non-enhancing bowel is dying bowel and changes a watchful plan into an operative one. All patients begin with resuscitation, because obstruction causes large fluid and electrolyte losses.
Pathway 1 — Conservative management ('drip and suck') of simple obstruction:
A simple adhesional small-bowel obstruction with no signs of strangulation on CT (bowel that enhances normally, no closed loop, no free fluid suggestive of ischaemia) is frequently managed non-operatively: intravenous fluids and electrolyte correction (the 'drip'), a nasogastric tube to decompress the stomach and proximal bowel (the 'suck'), nil by mouth, and close clinical and radiological monitoring. Many adhesional obstructions settle, and a water-soluble contrast study can help predict which will. Imaging that shows viable bowel and no closed loop is exactly what permits this safe, non-operative course.
Pathway 2 — Urgent surgery for complicated obstruction:
Imaging signs of ischaemia (absent enhancement, wall thickening, mesenteric oedema, free fluid), a closed-loop obstruction, strangulation, or perforation (free intraperitoneal gas) mandate urgent operation — to relieve the obstruction, resect non-viable bowel and repair or address the cause. A failure of a simple obstruction to settle on conservative management, or any clinical or radiological deterioration, also triggers surgery.
Pathway 3 — Cause-directed management of large-bowel obstruction:
LBO is most often due to colorectal carcinoma; CT both confirms the obstruction and stages the tumour, and management may involve emergency resection, a defunctioning stoma, or an endoscopically placed colonic stent as a bridge to surgery. A sigmoid volvulus is often decompressed endoscopically in the first instance. Crucially, a markedly dilated caecum (approaching 9–12 cm), especially with a competent ileocaecal valve creating a closed loop, signals an imminent perforation risk and pushes toward urgent intervention regardless of the underlying cause.
Throughout, the modality choice made earlier feeds the decision: the plain film raised the alarm and suggested the level, and the CT supplied the level, cause and viability that the surgical plan is built on.
Imaging-Guided Management of Intestinal Obstruction
SELF-CHECK
A 70-year-old man with progressive constipation and distension has a CT showing large-bowel obstruction due to a sigmoid carcinoma, with a competent ileocaecal valve and a caecum measuring 11 cm. Integrating these findings, what is the key concern that drives urgency?
A. There is no urgency as large-bowel obstruction is always managed conservatively
B. The competent ileocaecal valve creates a closed loop and the grossly dilated caecum (11 cm) is at high risk of perforation, mandating urgent intervention
C. The priority is to start a barium enema immediately to define the tumour
D. The caecal diameter is irrelevant; only the small bowel can perforate
Reveal Answer
Answer: B. The competent ileocaecal valve creates a closed loop and the grossly dilated caecum (11 cm) is at high risk of perforation, mandating urgent intervention
In large-bowel obstruction with a competent ileocaecal valve, the colon between the valve and the obstruction becomes a closed loop that progressively dilates; a caecum approaching 9-12 cm is at high risk of perforation (Laplace's law — wall tension rises with diameter), which drives urgent intervention. Large-bowel obstruction is not always conservative. Barium is contraindicated where perforation is a risk, and the caecum is in fact the colonic segment most prone to perforation in distal LBO.
CLINICAL PEARL
Pearl 1 — Valvulae conniventes vs haustra: Small-bowel folds (valvulae conniventes) cross the FULL width of the lumen; large-bowel folds (haustra) do NOT. With loop position (central vs peripheral) and calibre (SB >3 cm; colon >6 cm, caecum >9 cm), this is the high-yield, examinable way to call small- vs large-bowel obstruction on a plain film.
Pearl 2 — Plain film opens, CT decides: The abdominal X-ray confirms obstruction and suggests the level, but it cannot assess viability. CT supplies the level, cause and — via bowel-wall enhancement — the answer to the question that changes management: is the bowel ischaemic?
Pearl 3 — Closed-loop and absent enhancement = surgery: A closed-loop configuration with non-enhancing, thickened bowel, mesenteric oedema and free fluid signals strangulation. Like the strangulated hernia, non-enhancing bowel is dying bowel — operate.
Pearl 4 — Watch the caecum in LBO: A caecum approaching 9-12 cm, especially with a competent ileocaecal valve, is an imminent perforation risk and a reason to intervene urgently. And remember: free subdiaphragmatic gas on the erect film means perforation — never give barium when perforation is possible.
Self-Assessment — Intestinal Obstruction Imaging Decisions
Work through these scenarios as the surgical doctor on call, integrating the imaging findings into a management plan before reading the discussion.
Scenario A: A 60-year-old woman with previous appendicectomy and caesarean section has colicky pain, vomiting and distension. The abdominal X-ray shows central dilated loops with valvulae conniventes and air–fluid levels; CT shows dilated small bowel to a transition point at an adhesion, with normally enhancing bowel, no closed loop and no free fluid. How do you manage her?
Discussion: This is a simple adhesional small-bowel obstruction with imaging confirming viable bowel (normal enhancement) and no danger signs. The appropriate management is conservative: intravenous fluids and electrolyte correction, a nasogastric tube for decompression, nil by mouth, and close monitoring ('drip and suck'). A water-soluble contrast study may help predict resolution. Surgery is reserved for failure to settle or any sign of strangulation. The CT's demonstration of viable bowel is precisely what makes safe non-operative management possible.
Scenario B: A 48-year-old man with no prior surgery has sudden severe abdominal pain, distension and a rising heart rate. CT shows a C-shaped, fluid-filled closed loop of small bowel that does not enhance, with mesenteric oedema and free fluid. What does this represent and what is the management?
Discussion: The non-enhancing closed loop with mesenteric oedema and free fluid indicates strangulating closed-loop obstruction with bowel ischaemia — a surgical emergency. The management is urgent operation after rapid resuscitation: relieve the obstruction, assess viability and resect non-viable bowel, with antibiotics and a nasogastric tube. There is no role for prolonged conservative management here; absent enhancement is dying bowel.
Scenario C: A 75-year-old man has progressive constipation, distension and weight loss. The abdominal X-ray shows peripheral dilated loops with haustra and a caecum of 10 cm; CT confirms an obstructing sigmoid carcinoma with a competent ileocaecal valve. How do you integrate these findings into management?
Discussion: This is large-bowel obstruction due to colorectal carcinoma, and the competent ileocaecal valve with a 10 cm caecum creates a closed loop at high risk of caecal perforation — a marker of urgency. CT confirms the cause and helps stage the tumour. Management is cause-directed and urgent: options include emergency resection, a defunctioning stoma, or a colonic stent as a bridge to surgery, with the dilated caecum pushing toward prompt intervention to avert perforation. Barium studies are avoided given the perforation risk.