Page 4 of 11
AS10.3-4 | Communication, Medical Errors and Medication Errors in Anaesthesia — SDL Guide
CLINICAL SCENARIO
In a busy morning operating list, a vial of adrenaline (1:1000) has been placed in a drug tray beside a vial of oxytocin. Both are clear solutions in similarly shaped ampoules. The anaesthetic trainee draws up what she believes is oxytocin for a third-stage prophylaxis injection — and inadvertently administers 1 mL of undiluted adrenaline (1 mg) intravenously to a postpartum woman. The result: hypertensive crisis, acute myocardial ischaemia, and a litigation case that results in a finding of systemic system failure. This is not a story of one careless doctor — it is a predictable event produced by a system that stored look-alike drugs together, had no colour-coding or double-check protocol, and relied entirely on individual vigilance under time pressure. Communication failures and medication errors are the two most preventable categories of perioperative harm, and together they account for a substantial proportion of all anaesthesia-related adverse events.
WHY THIS MATTERS
Anaesthesia is a high-stakes, fast-paced discipline in which the consequences of poor communication or drug errors can be immediate and catastrophic. AS10.3 and AS10.4 are Knowledge + Skills (KH) competencies that collectively address the human and system dimensions of patient safety: how communication failures propagate into harm; how to classify and define medical and medication errors; and what individual and system-level strategies prevent them. These competencies directly underpin the AETCOM module (Attitude, Ethics and Communication) and the NMC GMER 2023 requirement that every graduate demonstrate patient-safety awareness and professional communication skills. Understanding these principles also prepares you to participate meaningfully in morbidity-and-mortality (M&M) reviews, near-miss reporting systems, and critical-incident debriefs — the formal mechanisms by which institutions learn from error and improve.
RECALL
Before studying communication and medication errors in anaesthesia, confirm your recall of:
- The pharmacological principle of concentration and unit dose: a 1:1000 adrenaline solution contains 1 mg/mL; a 1:10,000 solution contains 0.1 mg/mL. Confusing these two concentrations is among the most consequential drug-preparation errors in emergency medicine and anaesthesia.
- The WHO Surgical Safety Checklist (from the companion SDL): Sign-In, Time-Out, Sign-Out — each pause point includes allergy and drug-reconciliation checks.
- SBAR communication framework: Situation, Background, Assessment, Recommendation — a structured handover tool adapted from military aviation for healthcare transitions.
- Drug nomenclature: generic (International Nonproprietary Name, INN) versus brand names; look-alike / sound-alike (LASA) drug pairs (e.g. dopamine/dobutamine, metformin/metronidazole, morphine/midazolam).
- ASA physical-status scale (I–VI): distinct from Mallampati (I–IV oropharyngeal view) — do not conflate these classification systems.
Role of Communication in Patient Safety (AS10.3): Mechanisms and Failure Modes
Communication is the connective tissue of safe perioperative care. The operating theatre is one of the most communication-demanding environments in medicine — a team of five to eight professionals with different training, roles, and vocabularies must share dynamic, time-sensitive information about a patient who is unconscious, in altered physiology, and entirely dependent on that team's collective situational awareness. When communication fails — through ambiguity, omission, hierarchy-induced silence, or faulty handover — the consequences are not merely inconvenient: they can be immediately life-threatening. Studies from the Joint Commission (USA), the WHO, and the National Patient Safety Agency (UK) consistently identify communication failure as a contributing factor in over 70% of sentinel events in operating theatres.
Categories of communication failure in anaesthesia:
- Authority gradient (hierarchy-induced silence): Junior team members recognise a problem but fail to speak up because of a real or perceived power differential. A circulating nurse who notices a wrong drug being drawn up but says nothing because a consultant is present. The two-challenge rule (from aviation crew resource management) requires any team member to raise a safety concern twice — if not acknowledged, they are empowered to escalate or stop the action.
- Faulty handover (the transition hazard): Clinical handovers — from operating theatre to recovery room, from recovery to ward, between anaesthetic teams during a long case — are the moments of highest information loss. Key drug infusions, allergies, blood-loss estimates, and post-operative instructions are the most frequently omitted items. Structured handover tools (SBAR, ISOBAR, I-PASS) reduce omissions by providing a cognitive scaffold that forces the sender to actively recall each category of essential information.
- Closed-loop communication failure: In an emergency, the anaesthesiologist calls for adrenaline. The scrub nurse does not verbally confirm the request and does not repeat back the drug name and dose. The anaesthesiologist assumes the instruction was heard and acted upon. Closed-loop communication requires: (a) the sender states the request explicitly, (b) the receiver repeats back the drug/dose/route, (c) the sender confirms. Any break in the loop is a communication failure.
- Distraction and interruption: The operating theatre environment generates multiple simultaneous auditory stimuli — alarms, conversation, surgical instruments, telephones. Interruptions during drug preparation are a documented cause of dose errors. The no-interruption zone concept (a protected physical and cognitive space during drug drawing and anaesthesia induction) has been adopted in many institutions to reduce distraction-related errors.
- Jargon and ambiguity: Medical shorthand and abbreviations ('U' for units, 'MS' for morphine sulphate or magnesium sulphate) are fertile ground for error. Verbal orders that use decimal points ("give zero point one mg" not "give .1 mg") and unit clarification ("milligrams, not micrograms") prevent transcription errors. The Institute for Safe Medication Practices (ISMP) publishes a list of dangerous abbreviations that should never be used.
- Situational awareness failure: A degraded mental model of the patient's status — because a team member has not been briefed, or information from a monitor was not acknowledged — results in a clinical decision made on incomplete data. Structured situation updates ("the patient's pressure has been dropping for five minutes — current BP is 70/40, pulse 110") build shared situational awareness.
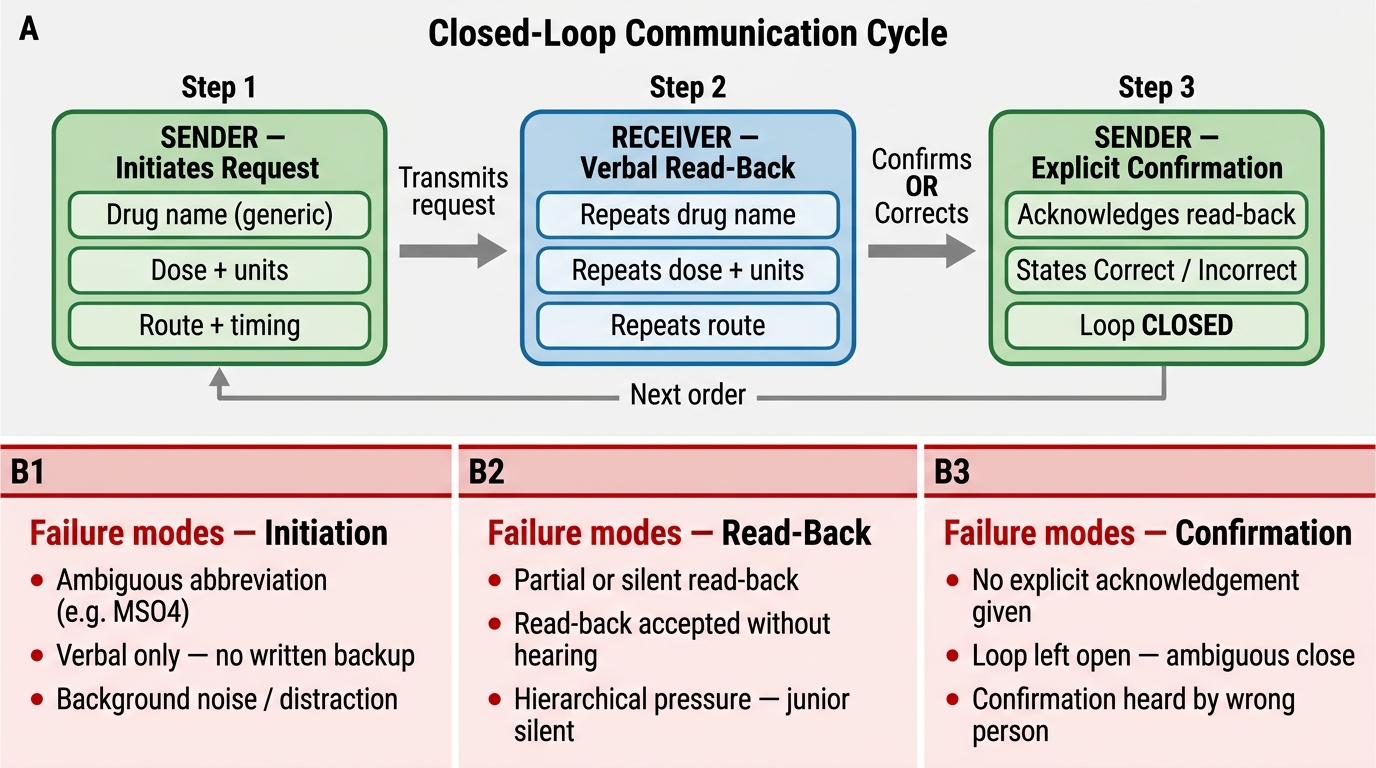
Closed-Loop Communication Cycle and Failure Modes in Anaesthesiology
Systematic interventions that reduce communication failures include:
- Crew Resource Management (CRM): adapted from aviation, CRM training teaches teams to use all available resources, assert leadership assertively-not-aggressively, challenge decisions through structured channels, and debrief after adverse events.
- Structured briefings and debriefings: a 5-minute pre-case team briefing (who is the patient, what is the procedure, what are the key anaesthetic concerns, who does what in an emergency) and a post-case debrief (what went well, what did not, what would we change) both improve future performance and team culture.
- SBAR handover tool: Situation (what is happening), Background (relevant clinical context), Assessment (what you think the problem is), Recommendation (what you are asking the receiver to do). Used at all clinical transitions.
- Respectful assertiveness: every team member has the right — and the professional duty — to raise a safety concern, regardless of hierarchy. The WHO Surgical Safety Checklist institutionalises this by requiring every team member to confirm patient identity and site aloud.
Classification of Medical and Medication Errors in Anaesthesia (AS10.4)
A medical error is defined as the failure of a planned action to be completed as intended (an error of execution) or the use of a wrong plan to achieve an aim (an error of planning). This definition, from the landmark US Institute of Medicine report To Err is Human (1999), shaped modern patient-safety science by reframing error as a predictable product of defective systems rather than solely of individual negligence. In anaesthesia, medical errors are further classified by type, by detectability, and by contribution to outcome. It is important to recognise that the same outcome — patient harm — can result from very different types of error, and that each type demands a different prevention strategy. The discipline of patient-safety science therefore begins with precise taxonomy, because naming the error correctly is the first step towards addressing its root cause.
Error taxonomy in anaesthesia:
- Active errors (sharp-end errors): committed by the person directly caring for the patient — the anaesthesiologist who draws up the wrong drug, the surgeon who operates on the wrong site. Active errors are immediately apparent and produce immediate harm, making them highly visible but not the root cause.
- Latent errors (blunt-end errors): systemic deficiencies in design, organisation, training, or maintenance that create the conditions in which active errors occur — the pharmacy that stores look-alike drugs in the same drawer, the institution that skips WHO checklist training, the hospital that has no drug-concentration labelling standard. Latent errors are the true root causes.
- Errors of omission vs commission: an error of omission is a failure to act when action was required (not administering prophylactic antibiotics before incision); an error of commission is taking an incorrect action (administering the wrong drug).
- Near miss (near-miss event): an error or unsafe condition that was detected and corrected before reaching the patient, or reached the patient without causing harm. Near misses are the most important learning resource in safety science because they occur far more frequently than adverse events and reveal system vulnerabilities at a stage when correction is still possible.
- Adverse event: harm that results from a medical intervention, not from the underlying disease. Anaesthesia-specific adverse events include anaphylaxis, awareness under anaesthesia, post-operative nausea and vomiting (PONV), nerve injury, aspiration pneumonitis, and medication-related harm.
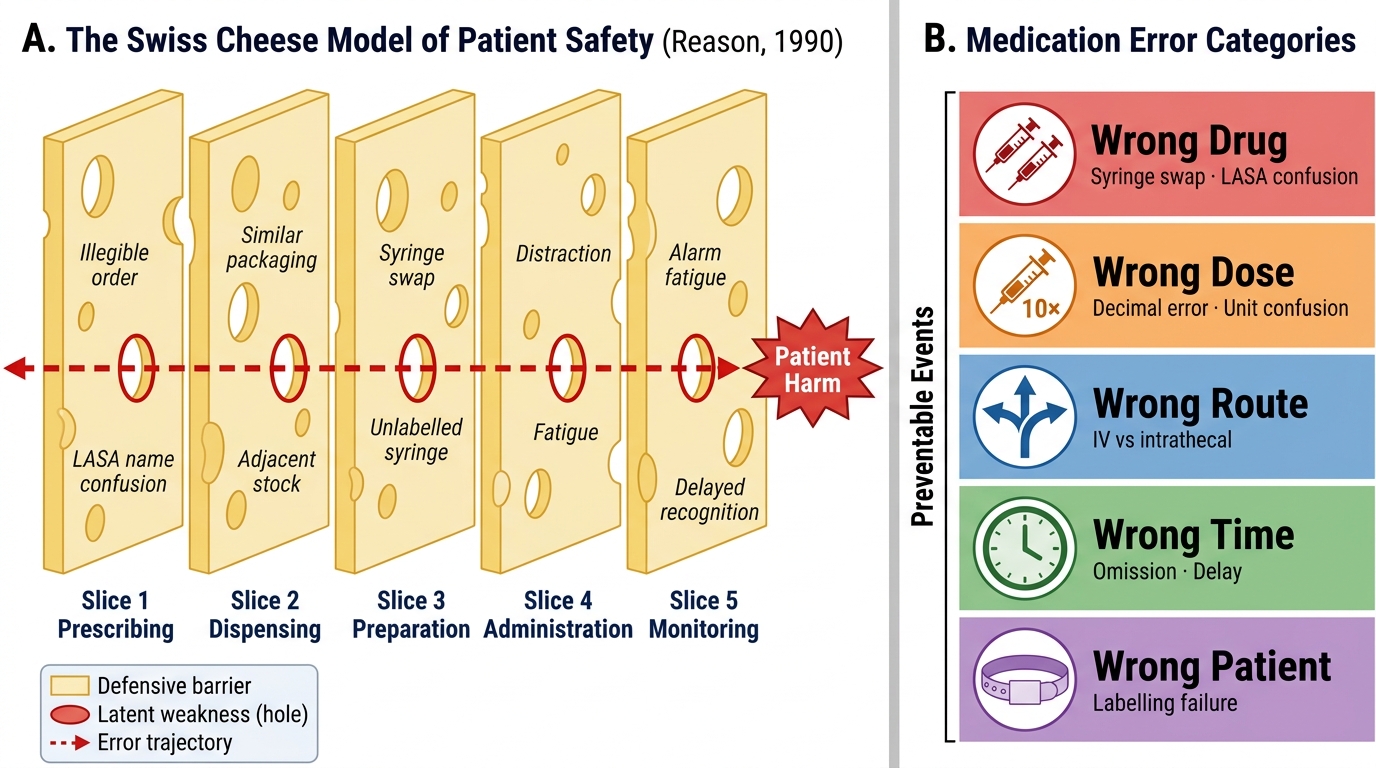
Swiss Cheese Model Applied to Anaesthetic Medication Errors (Reason, 1990)
The Swiss Cheese Model (James Reason, 1990) is the conceptual framework underlying modern patient-safety thinking. Every safety system has multiple defensive barriers (Swiss cheese slices): prescribing, dispensing, preparation, labelling, administration, monitoring. Each barrier has weaknesses (holes in the cheese). A single hole in one layer does not cause harm — the error is caught. Harm results when holes in multiple layers align simultaneously, allowing the error trajectory to pass through all defences. Interventions that prevent harm must target the holes in multiple layers simultaneously, not just the moment of active error.
Medication errors — specific taxonomy:
Medication errors are a subset of medical errors defined as any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the healthcare professional or patient. In anaesthesia, Fasting et al. and other landmark audit studies identify the following categories:
- Wrong drug: the most dramatic and most studied error. Caused by: syringe swaps (two syringes in the same tray, wrong label applied), drug-name confusion (LASA pairs — vecuronium/vasopressin, adrenaline/atropine in paediatrics), ampoule similarity (neostigmine vs atropine in identical vials), verbal orders with misheard drug names.
- Wrong dose: includes overdose (decimal-point error: 10× dose ordered as 1.0 mg, administered as 10 mg), underdose (failed dose calculation), and wrong unit (mg vs mcg confusion — commonest with fentanyl, neostigmine, and suxamethonium).
- Wrong route: intrathecal administration of an epidural drug (epidural bupivacaine concentrated formulations used intrathecally), intravenous injection of an oral liquid (especially in neonates), intra-arterial injection of a drug intended for intravenous use.
- Wrong patient: drug prescribed or administered to the wrong patient — preventable by patient-identity verification at every drug administration step.
- Wrong time: omission (antibiotic not given before incision), delay (insulin not held preoperatively leading to intraoperative hypoglycaemia), or premature administration (anticoagulant given too early before a neuraxial block).
- Wrong concentration: particularly relevant to infusion drugs — lignocaine 2% inadvertently used instead of lignocaine 0.5% for a spinal-level block, resulting in systemic toxicity. Adrenaline 1:1000 (1 mg/mL) used intravenously instead of 1:10,000 (0.1 mg/mL) as in the opening clinical vignette.
Risk Assessment and Analysis of the Error-Prone Anaesthetic Environment
The anaesthetic drug administration environment has several structural features that make it uniquely susceptible to medication error compared with other areas of hospital practice. Understanding these features is not an exercise in accepting inevitability — it is the foundation for designing targeted interventions. A structured assessment of the error-prone environment is the prerequisite for risk-reduction strategy development.
Anaesthesia-specific risk factors for medication error:
The anaesthesiologist is simultaneously prescriber, dispenser, and administrator — collapsing the three-point check system that exists in ward-based medicine (prescribing doctor, dispensing pharmacist, administering nurse). This concentration of function removes the independent check that catches most errors in other settings. The drug preparation area is a small, cluttered space where multiple syringes and ampoules are handled simultaneously at high speed. Operating-theatre lighting, though generally good, can impair label reading at angle or distance. Intraoperative emergencies create extreme time pressure that compromises the careful label-verification steps available under elective conditions.
Human factors analysis identifies six risk domains in anaesthetic drug errors:
- Similarity — look-alike/sound-alike (LASA) drug pairs whose ampoules, labels, and names are visually or phonetically similar. Recognised pairs include: adrenaline/oxytocin (both clear, similarly shaped), vecuronium/vasopressin, metaraminol/morphine, potassium chloride/sodium chloride (electrolyte concentration errors), ketamine/thiopentone (both white powders for reconstitution).
- Distraction — interruptions during drug drawing are independently associated with error. The period from opening an ampoule to labelling the syringe is the highest-risk interval.
- Fatigue and shift patterns — errors increase towards the end of long operating lists and at night. A culture of 'soldiering through' tiredness increases systemic risk.
- Novel environment — unfamiliar drug storage layouts (rotating to a new theatre, locum practice) markedly increase the probability of reaching for the wrong drug from the wrong drawer.
- Production pressure — the systemic pressure to keep the operating list moving creates implicit incentives to skip verification steps.
- Normalisation of deviance — repeated minor deviations from safe practice (drawing up without fully reading the label, skipping a verbal read-back) that pass without incident create a false sense that the deviation is safe.
Risk-scoring frameworks in anaesthesia: The Australian Patient Safety Foundation (APSF) anaesthetic incident classification and the AIMS (Australian Incident Monitoring Study) database use taxonomy-based root-cause analysis to stratify near-miss and adverse events. Locally, the National Pharmacovigilance Programme of India and hospital adverse-event reporting systems create a learning infrastructure — but only if healthcare workers report without fear of punitive consequence. Just culture (accountability without punishment for honest errors) is the prerequisite for a functioning reporting system.
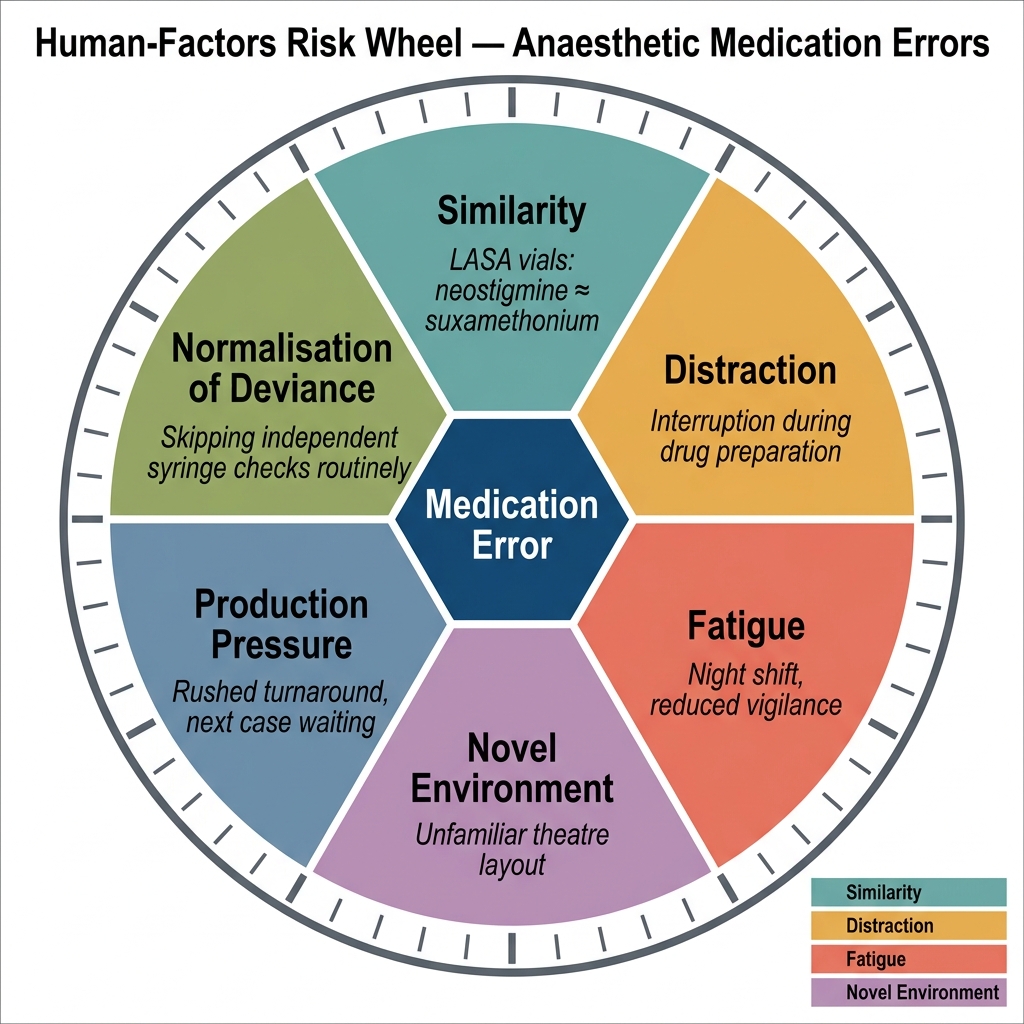
Human-Factors Risk Wheel for Anaesthetic Medication Errors
SELF-CHECK
An anaesthetic trainee draws up what she believes is neostigmine 2.5 mg for neuromuscular reversal. She inadvertently draws up suxamethonium 100 mg from an identically shaped vial. She labels the syringe and injects it before the error is detected. Which type of medication error has occurred?
A. Error of omission — a reversal agent was not given
B. Wrong drug error — a LASA drug pair was swapped during preparation
C. Wrong dose error — an incorrect weight-based calculation was used
D. Wrong route error — the drug was given by an unintended route
Reveal Answer
Answer: B. Wrong drug error — a LASA drug pair was swapped during preparation
This is a classic 'wrong drug' error caused by a look-alike/sound-alike (LASA) pair: neostigmine and suxamethonium are both available as clear aqueous solutions in similar vials and share the 'NEO-/SUXA-' prefix in their abbreviated syringe labels in busy theatres. The Swiss Cheese Model analysis reveals latent errors: ampoules stored together, no colour-coded labelling, no independent check. The active error (the trainee) was the final unguarded hole. An error of omission would mean nothing was given; a wrong-dose error would mean the correct drug was given in the wrong amount; a wrong-route error would require the drug to be given by the wrong physical route (e.g., intrathecal instead of intravenous). Prevention strategies: separate storage of LASA pairs, colour-coded labels, verbal read-back of drug name and dose before every administration.